Cystoisospora Belli Infection in HTLV-1 Patients and Progression to Acute T-Cell Leukemia
Cystoisospora belli is a parasite in tropical and subtropical regions. It is transmitted via a direct fecal-oral cycle and is more common in areas with poor sanitation and warm weather. Severe cases have been reported in patients with HIV, organ transplants, and tumors worldwide. People with HTLV-1 are also at risk of persistent parasitic coinfections, such as S. stercoralis and C. belli. We describe a couple of cases of cystoisosporiasis in patients with HTLV-1 infection. The first case is a 45-year-old female who presented chronic watery diarrhea, for which she was diagnosed with C. belli infection. Thus, she was treated with TMP/SMX. An ATL diagnosis was made on the same admission. The second case is a 33-year-old female patient with a previous diagnosis of HTLV-1 who went to the emergency room multiple times due to recurrent watery diarrhea after multiple treatment and prophylaxis schemes. The cases suggest a potential link between C. belli infection in HTLV-1 patients and early development of ATL. Routine modified acid-fast staining should be conducted for C. belli in HTLV-1 patients. Further research is necessary to determine the potential association between this coccidia and HTLV-1.
Introduction
Cystoisospora belli, formerly known as Isospora belli, is a type of coccidian parasite that resides in the gastrointestinal tract and is transmitted via a direct fecal-oral cycle. This parasite is found globally but more commonly in tropical and subtropical regions such as Africa, the Caribbean, Central and South America, and Southeast Asia. Cystoisosporiasis is more common in areas with poor sanitation, warm weather, and crowded living conditions [1].
C. belli can cause diarrhea in healthy individuals, which usually resolves within a few days. However, people with compromised immune systems, such as those with AIDS, leukemia, lymphomas, organ transplants, or HTLV-1 infection, may experience acute or chronic enteritis with more severe symptoms [2, 3, 4, 5]. Cystoisosporiasis is characterized by watery diarrhea, abdominal pain, fever, nausea, vomiting, anorexia, and significant weight loss that can lead to dehydration and cachexia. Additionally, it may present with eosinophilia, steatorrhea, and Charcot-Leyden crystals [1].
People with HTLV-1 are also at risk of persistent parasitic coinfections, such as Strongyloides stercoralis and C. belli. The former is known to be associated with an early development of ATL in patients with HTLV-1. On the other hand, there have been reported cases of patients with HTLV-1 and C. belli developing ATL earlier [6]. Therefore, there could be an association between these pathogens, similar to that with S. stercoralis.
Cystoisospora belli infections can last for months, and relapses are common, but their reason is unknown. Two studies conducted in Peru indicated that cystoisosporiasis (8.4% to 10.6%) is one of the most common intestinal infections among HIV patients [7, 8].
This coccidial parasite can be identified by examining stool samples under a microscope with a modified acid-fast staining technique [9]. Once the diagnosis of C. belli infection is made, the recommended treatment is TMP/SMX (160/800 mg) taken orally twice daily for seven to ten days.
Here, we report two cases of C. belli-associated persistent diarrhea in HTLV-1-infected patients.
Case Report #1
A 45-year-old female patient from Lima presented to the emergency department with four weeks of watery diarrhea and diffuse abdominal pain. The diarrhea did not contain mucus or blood and occurred approximately five to six times daily. Two weeks before admission, the frequency of diarrhea increased to eight to nine times a day, and the patient began feeling weak. Therefore, the patient went to the emergency room, where she received hydration, and a stool ova & parasite test was performed, which returned negative. One week before admission, the patient’s symptoms persisted, and she began experiencing moderate to severe colicky abdominal pain. The patient’s condition deteriorated on the day of admission, and she experienced crampy muscle pain and tremors in her hands. These symptoms prompted her to seek medical attention at the emergency room, where she was subsequently admitted to the Infectious Diseases service.
Regarding her past medical history, she was previously diagnosed with HTLV-1 in 2019 after experiencing a clinical picture similar to the current one, in which she was diagnosed with cystoisosporiasis. S. stercoralis and HIV were ruled out at that time. She was started on TMP/SMX 160 mg (TMP component) orally twice daily for ten days, which led to a complete improvement of symptoms after one week. The patient had pulmonary tuberculosis when she was five years old, which was treated successfully with first-line drugs.
On the day of admission, during the patient’s physical examination, it was noticed that she had tachycardia and appeared moderately dehydrated. The laboratory tests indicated mild anemia with a hemoglobin level of 10.6 mg/dL (MCV 92.2 and MCH 30.3), WBC of 15,330/mm3 (neutrophils 3500 cells/mm3, eosinophils 80 cells/mm3, basophils 90 cells/mm3, monocytes 820 cells/mm3, lymphocytes 10,840 cells/mm3), and platelets of 241,000/mm3. Hypokalemia was also evident at 3.18 mmol/L, while sodium (141 mmol/L) and chloride (99 mmol/L) levels were within the normal range. Albumin was at 3.78 g/dL, and C-reactive protein was negative. Kidney function was normal, indicated by a serum creatinine level of 0.78 mg/dL, while liver function showed mild elevation of transaminases, with AST 109 U/L and ALT 82 U/L. The glucose level was 98 mg/dL.
The most significant finding from a biochemical perspective was the presence of hypercalcemia, with a level of 11.5 mg/dL (ionic calcium 1.57 mmol/L). The patient was administered fluids in the emergency room, which improved tachycardia and hydration status. Once hospitalized, a stool ova & parasite test was conducted, initially showing negative results. However, a modified acid-fast stain was performed, which was positive for Cystoisospora belli. Subsequently, a specific treatment was prescribed with TMP/SMX 160 mg (TMP component) twice daily orally, which led to clinical improvement.
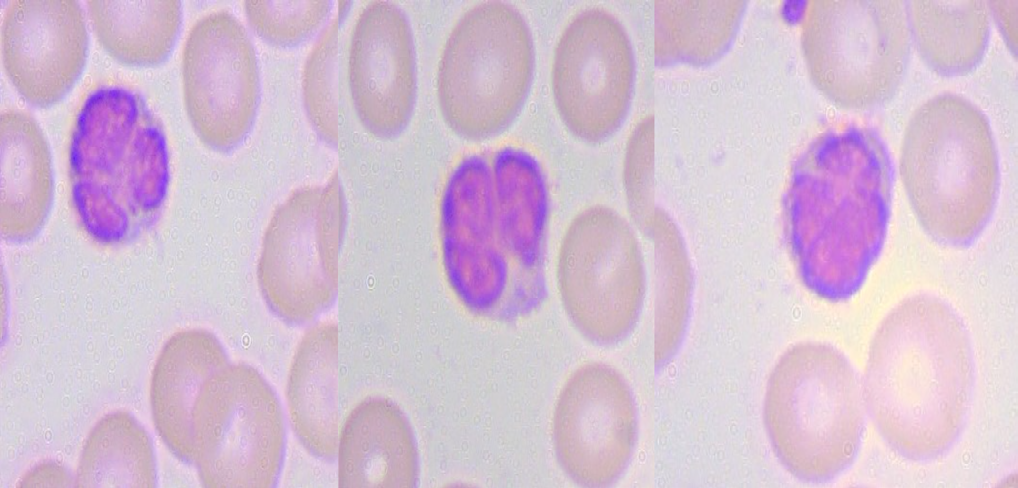
The patient was tested again for HIV, but the result was negative. Hematology and oncology were consulted, after which a peripheral blood smear was performed (Figure 1). The report showed increased lymphocyte count, atypical lymphocytes, and flower cells with no blasts. The atypical lymphocytes constituted 50% of the white blood cells, while flower cells were 5%. The red blood cells exhibited anisocytosis (1+) with no evidence of hemolysis. Platelets were within the normal range. Based on these findings, the patient was diagnosed with acute adult T-cell leukemia/ lymphoma and was referred to the oncology service to start chemotherapy.
Case Report #2
A 33-year-old female patient went to the emergency room in February 2024 due to a ten-day history of watery diarrhea, nausea, vomiting, and oral intolerance. Ten days before admission, the patient reported diffuse abdominal pain of moderate intensity and watery diarrhea without mucus and blood, around four to five liquid stools per day. The abdominal pain partially improved after defecation. Seven days before admission, the number of watery diarrheas per day increased to seven to eight. Five days before admission, she experienced refractory nausea and vomiting, and diarrhea increased to ten stools a day. Three days before admission, she stopped ingesting liquids and solids due to oral intolerance. One day before admission, she complained of fatigue and general malaise in addition to the previously mentioned symptoms. Therefore, the patient went to the emergency room and was admitted for further workup.
Among her past medical history, she was diagnosed with HTLV-1 in 2011 due to a month of weight loss and watery diarrhea. At that time, she underwent tests, and the results showed S. stercoralis infection. Thus, the patient was treated with ivermectin, which led to a complete improvement in symptoms. The patient remained asymptomatic until 2020 when she presented to the emergency room complaining of watery diarrhea with moderate dehydration. She was diagnosed with cystoisosporiasis for the first time and was treated with TMP/SMX 160 mg (TMP component) twice a day for seven days. She showed improvement in symptoms on the fourth day of treatment.
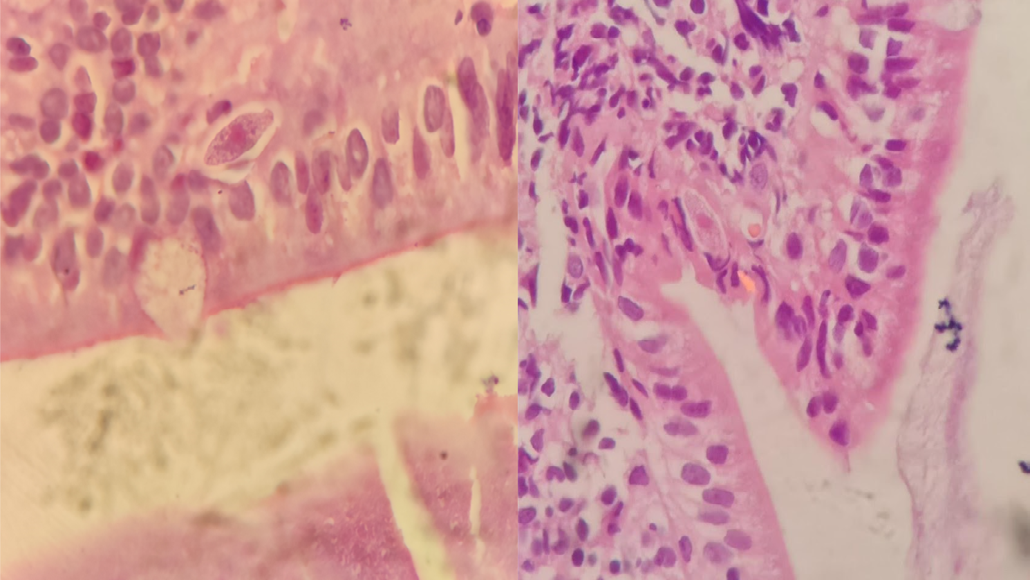
In 2022, she presented the same symptoms again, and the diagnosis and treatment were repeated. However, the regimen was extended to three weeks, improving the symptoms by the second week. During this admission, a biopsy was performed (Figure 2).
At the beginning of 2023, she was admitted again, complaining of the same clinical picture, and the same diagnosis of cystoisosporiasis was made. Thus, at discharge, it was decided to start continuous prophylaxis with TMP/ SMX 160 mg (TMP component) three times per day, pyrimethamine 25 mg orally daily, and doxycycline 100 mg twice a day orally. The patient remained asymptomatic for a year and regained weight. In October 2023, she was admitted for the same condition, subsequently treated, and discharged with prophylaxis: TMP/SMX 160 mg (TMP component) three times a day, doxycycline 100 mg twice a day orally, and loperamide 2 mg daily.
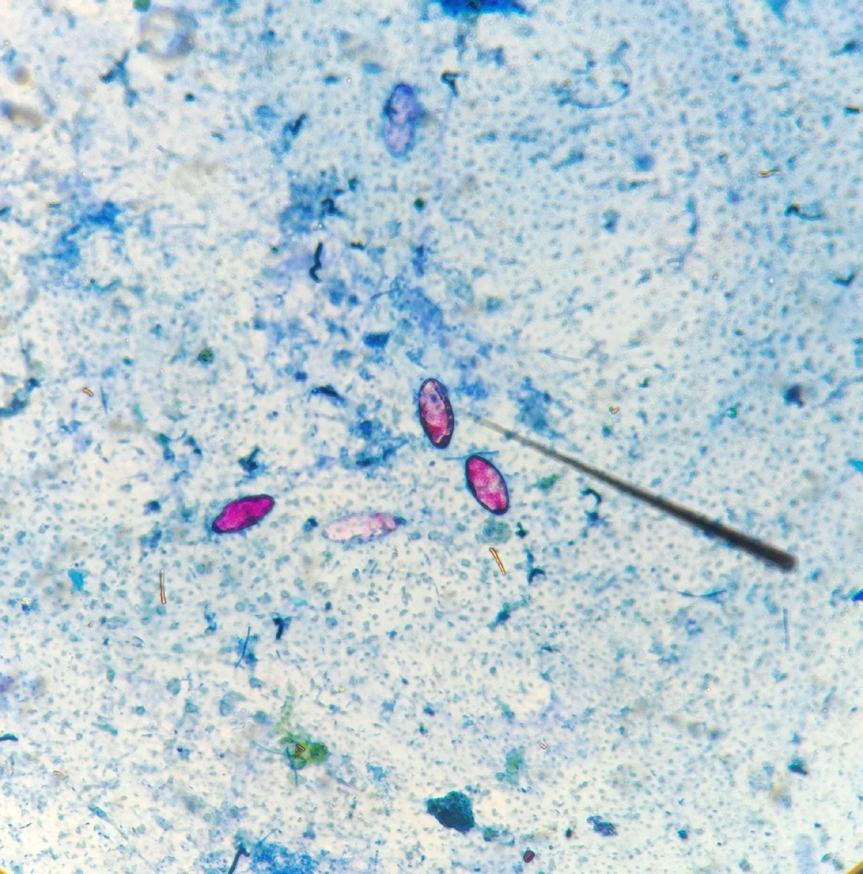
Upon the last admission in February 2024, the patient was tachycardic, in poor general condition, dehydrated, and hypotensive. The laboratory tests showed moderate anemia with a hemoglobin level of 9.8 mg/dL (MCV 97 and MCH 32), WBC of 4000 cells/mm3 (neutrophils 1870 cells/ mm3, eosinophils 130 cells/mm3, basophils 20 cells/mm3, monocytes 330 cells/mm3, lymphocytes 1650 cells/mm3), and platelets of 306,000/mm3. Potassium (3.69 mmol/L), sodium (137 mmol/L), and chloride (105 mmol/L) levels were within the normal range. Albumin was at 3.8 g/dL, and C-reactive protein was negative. Kidney function was normal (serum creatinine level of 0.46 mg/dL), while liver function showed mild elevation of transaminases (AST 116 U/L and ALT 120 U/L). The patient received intravenous fluids in the emergency room, which improved tachycardia and volume (intravascular) status. Stool ova & parasites with modified acid-fast staining was performed, which resulted in a positive finding for Cystoisospora belli (Figure 3).
Subsequently, the patient was prescribed treatment with TMP/SMX 320 mg (TMP component) three times per day intravenously and ciprofloxacin 400 mg twice daily. After four days of treatment, the nausea and vomiting ceased, and the stools decreased to three per day of semi-solid consistency. The therapy was switched to an oral regimen: TMP/SMX 320 mg (TMP component) three times daily, pyrimethamine 25 mg once daily, and doxycycline 100 mg twice daily. The patient resolved her symptoms on the eighth day of treatment and was discharged with prophylaxis with TMP/SMX 160 mg orally four times daily and ciprofloxacin 500 mg three times daily.
Discussion
Cystoisospora belli infection is a significant cause of acute and chronic watery diarrhea in immunosuppressed patients, especially those with HIV, which can lead to high rates of morbidity and mortality [4]. This pathogen is a coccidian parasite that lives in the gastrointestinal tract and is present worldwide, particularly in tropical and subtropical regions. The parasite is spread through a fecal-oral transmission cycle, where humans become infected after ingesting oocysts in contaminated food or water [1].
While C. belli can cause diarrhea in healthy individuals, it typically clears up within a few days. However, in immunocompromised patients, it tends to be more severe and persistent, even with relapses [10]. Cystoisosporiasis is an indicator of AIDS infection, although its incidence is low [11]. In immunocompromised patients, the disease is characterized by watery diarrhea, colicky abdominal pain, fever, nausea, vomiting, anorexia, malabsorption, and significant weight loss, which may lead to dehydration and cachexia [1]. Eosinophilia is often observed in laboratory studies [1].
On the other hand, HTLV-1 infection can conduct to two main complications: tropical spastic paraparesis (TSP) and adult T-cell leukemia/lymphoma (ATL). TSP causes subacute or chronic spastic weakness in both legs, urinary retention, and constipation [12]. ATL is a hematological malignancy that usually emerges many years after infection [13]. Moreover, atypical T cells in the blood smear consist of malignant infected flower cells due to their nucleic pattern, as seen in the first case’s blood smear [14].
The potential interaction between HTLV-1 and C. belli has not been further analyzed beyond case reports. Some cases describe HTLV-1 patients who were diagnosed during their admission with ATL. Two ATL cases, one in Sudan and the other in Haiti, presented chronic diarrhea that improved initially with the regular TMP/SMX regimen [6, 15]. However, after a few months, both became reinfected with C. belli, similar to the first case we presented. The Haitian patient responded well to treatment and was discharged with secondary prophylaxis. Nevertheless, the Sudanese patient did not improve with TMP/SMX treatment and died due to persistent dehydration and hydroelectrolytic imbalances. In our second case, we present a patient with similar features regarding the persistence of the coccidial infection. HTLV-1 would predispose patients to persistent and/or recurrent C. belli infections. If left untreated or without prophylaxis, this could lead to fatal consequences.
Additionally, there have been two cases in Japan whereby patients with ATL responded positively to standard treatment for C. belli infection [16, 17]. However, one of them presented symptoms once again after a few days. Similar to this case, it has been demonstrated that patients with HIV/AIDS can experience chronic and recurring cystoisosporiasis due to the reactivation of tissue cysts formed by the sporozoites. These cysts can be found in extraintestinal organs or the gut lamina propria. Among the extraintestinal organs involved, the most common are the spleen, liver, mediastinum, bronchus, and mesenteric lymph nodes. This phenomenon occurs more frequently in immunosuppressed individuals.
A fatal case of C. belli infection in HTLV-1 without ATL has been described in Iran [18]. Even though this patient responded well to treatment for C. belli infection, she died due to malabsorption syndrome, which depicts the severity of this parasitic infection in HTLV-1 patients. Although none of the cases we presented has died, the patient of the second case suffered from severe weight loss and cachexia, similar to what happens in malabsorption syndrome.
A modified acid-fast staining technique is widely used and approved to diagnose Cystoisospora belli infection in its oocyst form. When this coccidia is detected in stools, it is essential to thoroughly investigate the underlying causes of immunocompromise, such as HIV, hematologic malignancies, or HTLV-1/2 [18, 19, 20]. Conversely, in patients diagnosed with HTLV-1, routine stool examination should be performed to detect C. belli infection. Furthermore, in HTLV-1 patients diagnosed with cystoisosporiasis, prophylaxis with TMP/ SMX should be considered, especially in those with ATL. This is due to the high risk of relapses and its potential association with an earlier development of this malignancy.
Our cases were treated according to current guidelines for immunocompromised patients: TMP/SMX (160/800 mg) given orally twice daily for seven to ten days [21]. Although the patient in the first case improved with this regimen, the second did not. Recommendations are established to increase the dosage and frequency of administration if symptoms worsen or persist, as was done for the second patient. Depending on the clinical response, the regimen could be extended up to three or four weeks [22].
The route of administration depends on the severity of the case. Oral administration is preferred for mild to moderate cases, while intravenous administration is indicated for severe cases (malabsorption syndrome or oral intolerance) [21]. The first patient responded well to the treatment, while the second case required intravenous medications due to the severity of the case.
There is no clear indication to start secondary prophylaxis in immunocompromised patients other than those with HIV and a CD4 cell count of less than 200 cells/ul. Studies suggest that this measure should be discussed while considering the underlying disease, drug tolerability, and interactions. The prophylaxis regimen usually consists of TMP-SMX (160/800 mg) taken orally thrice weekly [23]. In our second case, the patient underwent different prophylaxis regimens due to constant failure and relapses. The various schemes were developed by reviewing the literature and consulting with experts.
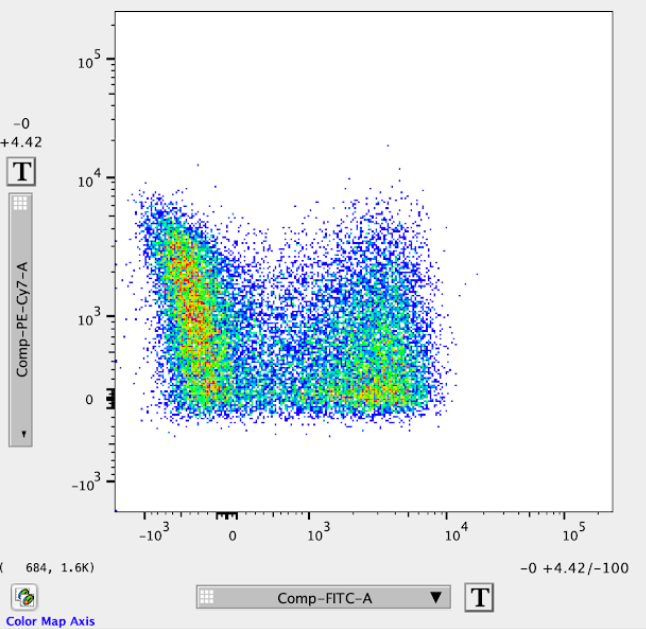
For study purposes, flow cytometry through the BD FACSCanto II system from Case #2 was performed after extracting PBMCs and marking them with human antibodies directed to the following markers: CD3, CD4, CD8, CD7, and CADM1. T-helper cells were selected through gating to find the percentage of cells that expressed high levels of CADM1 and low levels of CD7. This was performed to analyze a potential malignant transformation.
Compared to a flow cytometry result of an average ATL patient, which usually presents a clear CADM1+ CD7- T-helper cell subset, the results obtained for this patient do not demonstrate such a clear population [24]. Nevertheless, as seen in Figure 4, two clear T-helper cell groups are divided by the expression of CADM1 (attached to FITC). On the other hand, the division by CD7 expression (attached to PE-Cy7) is not that marked. However, T-helper cells expressing different amounts of CD7 on their surface could be due to a transition status of CD7 downregulation. This flow cytometry pattern has been associated with clonal expansion in ATL patients [24]. Recognizing this, it is noteworthy to mention that a few cases in Japan have reported a potential association between C. belli infection in HTLV-1 patients and the onset of ATL or malignant lymphoma [18, 25]. Therefore, flow cytometry may be a valuable method for further investigation into cases of C. belli infection in HTLV-1 patients and the early stages of malignant transitions, such as the development of early ATL.
Conclusion
The cases discussed suggest that there might be a link between C. belli infection in patients with HTLV-1 and the early development of ATL. The first case involved a patient who had recently been diagnosed with ATL and had a history of cystoisosporiasis. On the other hand, the second case showed an HTLV-1 patient with recurrent C. belli infections, whose flow cytometry results suggested a potential future transformation to ATL.
Similar to the recommended serial stool ova and parasite tests to search for S. stercoralis in HTLV-1 patients, modified acid-fast staining should be conducted routinely to search for C. belli in this group of patients. Additionally, in patients diagnosed with cystoisosporiasis, all causes of immunosuppression, including HTLV-1, must be ruled out, especially in endemic countries.
Further research is necessary to determine the potential association between this coccidia and HTLV-1.
Conflicts of Interest
There is no conflict of interest in this publication.
Authority contribution
All authors participated in writing the article, collecting and interpreting data, conducting a bibliographic review, critically reviewing the paper, and approving the version to be published.
Ethical approval
Written informed consent was obtained from the patients to publish this case report.
Acknowledgments
We want to finish by acknowledging and thanking the people living with HTLV–1 who have generously participated in this research. We also wish to acknowledge the grant from R01 AI136870 – “The effect of Strongyloides stercoralis on HTLV-1 disease progression” – NIAID, NIH (PI: Martin Montes). The content is solely the authors’ responsibility and does not necessarily represent the official views of the National Institutes of Health.
Funding
R01 AI136870 - “The effect of Strongyloides stercoralis on HTLV1 disease progression” – NIAID, NIH (PI – Martin Montes).
References
-
Dubey JP, Almeria S (2019) Cystoisospora belli infections in humans: the past 100 years. Parasitology 146(12): 1490-1527.
-
Gupta S, Narang S, Nunavath V, Singh S (2008) Chronic diarrhoea in HIV patients: prevalence of coccidian parasites. Indian J Med Microbiol 26(2): 172-175.
-
Vignesh R, Balakrishnan P, Shankar EM, Murugavel KG, Hanas S, et al. (2007) High proportion of isosporiasis among HIV-infected patients with diarrhea in southern India. Am J Trop Med Hyg 77(5): 823-824.
-
Tsutsui T, Kakizaki Y, Miyashita Y (2021) Cystoisospora belli associated persistent diarrhea in an AIDS patient. J Infect Chemother 27(2): 348-349.
-
Usluca S, Inceboz T, Unek T, Aksoy U (2012) Isospora belli in a patient with liver transplantation. Turkiye Parazitol Derg 36(4): 247-250.
-
Ud Din N, Torka P, Hutchison RE, Riddell SW, Wright J, et al. (2012) Severe Isospora (Cystoisospora) belli Diarrhea Preceding the Diagnosis of Human T-Cell-Leukemia- Virus-1-Associated T-Cell Lymphoma. Case Rep Infect Dis 2012: 640104.
-
Omayra CL, Bernabé-Ortiz A, Samalvides F, Soto L, Gotuzzo E, et al. (2009) Infecciones parasitarias intestinales y factores asociados a la infección por coccidias en pacientes adultos de un hospital público de Lima, Perú. Rev Chil Infectol 26(5): 440-444.
-
García C, Rodríguez E, Do N, Castilla DL, Terashima A, et al. (2006) Parasitosis intestinal en el paciente con infección VIH-SIDA. Rev Gastroenterol Perú 26(1): 21- 24.
-
DeHovitz JA, Pape JW, Boncy M, Johnson WD Jr (1986) Clinical manifestations and therapy of Isospora belli infection in patients with the acquired immunodeficiency syndrome. N Engl J Med 315(2): 87-90.
-
Assefa S, Erko B, Medhin G, Assefa Z, Shimelis T (2009) Intestinal parasitic infections in relation to HIV/AIDS status, diarrhea and CD4 T-cell count. BMC Infect Dis 9: 155.
-
Gautam N, Khurana S, Sharma A, Sehgal R (2014) Isosporiasis in a tertiary care center of North India. Indian J Pathol Microbiol 57(2): 272-274.
-
Bangham CRM, Araujo A, Yamano Y, Taylor GP (2015) HTLV-1-associated myelopathy/tropical spastic paraparesis. Nat Rev Dis Primers 1: 15012.
-
Matsuoka M, Jeang K-T (2007) Human T-cell leukaemia virus type 1 (HTLV-1) infectivity and cellular transformation. Nat Rev Cancer 7(4): 270-280.
-
Peloponese J-M Jr, Kinjo T, Jeang K-T (2007) Human T-cell leukemia virus type 1 Tax and cellular transformation. Int J Hematol 86(2): 101-106.
-
Hasan M, Bishburg E, Nagarakanti S (2017) Recurrent Cystoisospora belli in a patient with HTLV-1 infection. IDCases 10: 122.
-
Kawano F, Nishida K, Kurisaki H, Tsukamoto A, Satoh M, et al. (1992) [Isospora belli infection in a patient with adult T-cell leukemia]. Rinsho Ketsueki 33(5): 683-687.
-
Yamane T, Takekawa K, Tanaka K, Hasuike T, Hirai M, et al. (1993) [Isospora belli infection in a patient with adult T cell leukemia]. Rinsho Byori 41(3): 303-306.
-
Shafiei R, Najjari M, Kheirabad AK, Hatam G (2016) Severe Diarrhea Due To Cystoisospora belli Infection in an HTLV-1 Woman. Iran J Parasitol 11(1): 121-125.
-
Agholi M, Hatam GR, Motazedian MH (2013) HIV/AIDS- associated opportunistic protozoal diarrhea. AIDS Res Hum Retroviruses 29(1): 35-41.
-
Resiere D, Vantelon JM, Bourée P, Chachaty E, Nitenberg G, et al. (2003) Isospora belli infection in a patient with non-Hodgkin’s lymphoma. Clin Microbiol Infect 9(10): 1065-1067.
-
University of Alabama at Birmingham (2013) Drugs for Parasitic Infections.
-
La Hoz RM, Morris MI, AST Infectious Diseases Community of Practice (2019) Intestinal parasites including Cryptosporidium, Cyclospora, Giardia, and Microsporidia, Entamoeba histolytica, Strongyloides, Schistosomiasis, and Echinococcus: Guidelines from the American Society of Transplantation Infectious Diseases Community of Practice. Clin Transplant 33(9): e13618.
-
Kaplan JE, Benson C, Holmes KK, Brooks JT, Pau A, et al. (2009) Guidelines for prevention and treatment of opportunistic infections in HIV-infected adults and adolescents: recommendations from CDC, the National Institutes of Health, and the HIV Medicine Association of the Infectious Diseases Society of America. MMWR Recomm Rep 58(RR-4): 1-207.
-
Kobayashi S, Nakano K, Watanabe E, Ishigaki T, Ohno N, et al. (2014) CADM1 expression and stepwise downregulation of CD7 are closely associated with clonal expansion of HTLV-I-infected cells in adult T-cell leukemia/lymphoma. Clin Cancer Res 20(11): 2851- 2861.
-
Ohtaki M, Michimata Y, Suzuki T, Oikawa K, Mikami M (1976) Malignant lymphoma initiated with malabsorption syndrome due to Isospora belli infection and lymphocytosis. Tohoku J Exp Med 120(1): 43-51.
- hMPV: Is It Another Covid-19 Like Situation?
- Streptomyces: Sources of Novel Discoveries in Antibiotic Research to Combat Antimicrobial Resistance
- A Review of Mosquitoes (Diptera: Culicidae) and Their Biodiversity, Medical and Veterinary Importance
- Past and Current Immunotherapy in Cancer
- Hematological Cancer and Viral Infection
- The Growing Threat of Antimicrobial Resistance in India: Challenges and Solutions