Prevelence of Hepatitis C, in Catchment Area of Khairpure Medical College Hospital Khairpure Mirs Pakistan
Hepatitis C is emerging as the major threat for the population of Pakistan and This infection of the liver is caused by the hepatitis C virus. About 3.9 million people in the U.S. have the disease. But it causes few symptoms, so most of them don't know, This disease is prevalent in khairpure Mirus, Pakistan, yet up-to-date data on the epidemiology of hepatitis C in Khairpure Mir’s catchment area of Teaching hospital, KMC, khairpure, were not available before this. This study was undertaken to determine the current prevalence and distribution of Hepatitis C is first insight study in khairpure medical college khairpure Mirus catchment area. Methodology: one thousand, seven hundred and ninety four patients were referred to pathological laboratory of KMC teacing hospital khairpure Pakistan, who were suspected for hepatitis HCV, from different area of KMC teacing hospital khairpure Mirs Pakistan catchment area OPDs, and data was collected from January 2017 to august 2017 from which eleven hundred seventy were positive on Elisa method, were screened for HCV. Patients of either sex, with more than thirty years of age were included. From which 1170 HCV were positive on Elisa method. Result: Data were collected from January 2017 to august 2017 from which were Eleven hundred seventy were positive out of seventeen hundred and ninety four on Elisa method, were screened for HBV. Patients of either sex, with more than thirty years of age were included. From which 1170 HBV were positive on Elisa method. Data suggest a moderate to high prevalence of HBV, at KMC Hospital catchment area Khairpure Mirs, Pakistan. The modes of transmission of hepatitis C in Pakistan implicate contaminated needle use in medical care, drug abuse, unsafe blood and blood product transfusion as the major causal factors. Data suggest a moderate to high prevalence of HBV, at KMC Hospital catchment area Khairpure Mirs, Pakistan. Conclusion: Data suggest a moderate to high prevalence of HBV, at KMC Hospital catchment area Khairpure Mirs, Pakistan. Data suggest high prevalence of HCV and is alarming situation and silent threat to the population, at KMC Hospital catchment area Khairpure Mirs, Pakistan. The modes of transmission of hepatitis C in Pakistan implicate contaminated needle use in medical care, drug abuse, unsafe blood, and unlawful and without proper equipped laboratories running blood bank, and supplying blood to these areas people in this area and blood product transfusion as the major causal factors.
Introduction
Infection with hepatitis C virus (HCV) is a major global health concern. With an estimated 170 million people infected with HCV worldwide, this disease is proving to be an escalating economic, social and health burden Even though the prevalence in Asia has been estimated to be a little above 2%, it varies greatly between individual countries [1]. Mongolia has the highest HCV prevalence (above 10%), followed by Uzbekistan and Pakistan where, according to some reports, around 6% of the total population is infected with HCV [1, 2]. Although the prevalence of HCV infection seems to have declined in the past two decades in the United States [3, 4]. Awareness, improved safety of blood products, the availability of affordable and effective HCV therapies have contributed significantly to the decline in HCV in developed countries. However, lack of awareness, inadequate blood screening facilities, nosocomial transmission and a lack of effective treatments (due to various reasons) have so far been the major factors responsible for seemingly inexorable rise in HCV infection in many developing countries. The prevalence of HCV varies by region. Western Europe, the Americas and Australia are considered regions of low HCV prevalence (<2%). African and the eastern Mediterranean are areas with the highest HCV prevalence [2, 5]. In Egypt, the prevalence of HCV is greater than 14%, the highest of any country in world [6, 7, 8]. Even though the prevalence in Asia has been estimated to be a little above 2%, it varies greatly between individual countries [1]. Mongolia has the highest HCV prevalence (above 10%), followed by Uzbekistan and Pakistan where, according to some reports, around 6% of the total population is infected with HCV [1]. Our understanding of HCV epidemiology in Pakistan has been greatly improved by the numerous studies conducted over the span of the past two decades. Additionally, a comprehensive nation-wide survey of HBV/HCV prevalence, probably the first of its kind, was carried out in the years 2007-2008 [9] and a national hepatitis sentinel site surveillance system has been fully operational since June 2010 [10]. Data on the prevalence of HCV in Pakistan has previously been comprehensively reviewed [6, 11, 12]. Recent years have seen an increased focus among Pakistani researchers on the study of HCV prevalence patterns and frequency distribution of its genotypes. At least eighty six relevant studies have been published in national and international journals since the publication of aforementioned reviews (2009,2010). These newer studies have not only explored HCV prevalence in previously uncovered areas such as Azad Kashmir [13] and Baluchistan [14, 15] but have also shed light on the possible connection between underdevelopment and high HCV prevalence (for example, 23.83% prevalence in peri- urban areas of country’s largest city Karachi [16] and 25.1% in rural Sindh [17]. This highlights the importance and need for integration of newer reports in a comprehensive updated analysis. Above all, given the fact that some 15%-45% HCV infected patients may spontaneously clear the virus but still remain seropositivity for HCV [18, 19], results from seroprevalence studies may end up exaggerating the actual burden of disease. Recent World Health Organization (WHO) guidelines also recommend that polymerase chain reaction (PCR) based HCV diagnosis should be carried out not only to confirm HCV seropositivity but also to distinguish persons with active HCV infection from those with resolved past infection [20]. Not much attention has been paid to the categorical estimation of active HCV infection as determined by HCV nucleic acid testing (NAT) in previous systematic reviews [6, 11, 12]. Our understanding of HCV epidemiology in Pakistan has been greatly improved by the numerous studies conducted over the span of the past two decades. Additionally, a comprehensive nation-wide survey of HBV/HCV prevalence, probably the first of its kind, was carried out in the years 2007-2008 [9] and a national hepatitis sentinel site surveillance system has been fully operational since June 2010 [10]. Five single facility- based sentinel sites (located in four provincial capitals and Islamabad) have so far been established. Nonetheless, due to limited catchment areas of these facilities, data related to the incidence of new cases and ongoing transmission patterns and trends in the majority of the population remains inadequate. Also, the scope of the national survey was limited only to screening for HBV/HCV seropositivity among healthy individuals. Thus the survey did not encompass HCV prevalence in high risk groups and the frequency distribution of HCV genotypes was also not studied. Even a cumbersome endeavor like national survey therefore did not provide data of such high translational importance. Intravenous drug use is one of the most important risk factors in HCV transmission worldwide [1]. However, its relative contribution to the HCV endemic in Pakistan is not clear. According to a recent United Nations Office on Drugs and Crime report, some 6-7 million Pakistanis admitted using drugs in the past one year, around half million of which were regular intravenous drug users (IDUs) [21]. Unfortunately, not many studies are available which have focused on serofrequency of HCV infection in this high risk group. Only two recent studies reported HCV prevalence in various districts of KPK province [22, 23]. These reports show a prevalence of HCV infection among IDUs to range from 14.3% to 35%. Similarly, only two reports have been published on active HCV infection among IDUs (intravenous drug users. in Pakistan since 2010 [22, 23]. While Ali and colleagues found 14.3% active HCV infection among a small group of 42 IDUs [22], a study by Rehman, et al. [23] reported a very high (24%) HCV prevalence among 200 IDUs. Active HCV infection has not been adequately investigated in other population subsets, particularly the high risk groups. Except for dialysis patients, for whom two reports are available [22], only one report each was published for blood donors [24], health care workers [25], pregnant women [26], multi-transfused patients and patients undergoing major surgery [22]. Screening of patients suffering from diseases, which are not considered a direct consequence of HCV infection or do not directly pose an increased risk of contracting HCV infection, except for the risk of nosocomial and iatrogenic transmission, is also an important surveillance strategy. Firstly, it can provide a window into the prevalence in general population and secondly, for an infection like HCV, it can also provide useful insights into the possible risk factors involved in the transmission of this virus. At least thirteen studies reported the prevalence of HCV in patients [22, 27, 28, 29]. These patients visited/attended hospitals with various complaints ranging from general mild sickness requiring outpatient care, to major and gynecological surgeries as well as dermatological and urological disorders (Figure 1).
![Figure 1: Polymerase Chain Reaction (PCR). Infection with hepatitis C virus (HCV) is a major global health concern. With an estimated 170 million people infected with HCV worldwide, this disease is proving to be an escalating economic, social and health burden [1,2]. Although the prevalence of HCV infection seems to have declined in the past two decades in the United States [3,4], Western and Northern Europe [5,6], Japan [7] and Australia [8], the burden of this disease in many of the lesser developed and developing countries is continuously on the rise [2]. Awareness, improved safety of blood products, the availability of affordable and effective HCV therapies have contributed significantly to the decline in HCV in developed countries. However, lack of awareness, inadequate blood screening facilities, nosocomial transmission and a lack of effective treatments (due to various reasons) have so far been the major factors responsible for seemingly inexorable rise in HCV infection in many developing countries [2,9].](/fulltextimages/1740/fig_1.png)
Figure 1: Polymerase Chain Reaction (PCR). Infection with hepatitis C virus (HCV) is a major global health concern. With an estimated 170 million people infected with HCV worldwide, this disease is proving to be an escalating economic, social and health burden [1, 2]. Although the prevalence of HCV infection seems to have declined in the past two decades in the United States [3, 4], Western and Northern Europe [5, 6], Japan [7] and Australia [8], the burden of this disease in many of the lesser developed and developing countries is continuously on the rise [2]. Awareness, improved safety of blood products, the availability of affordable and effective HCV therapies have contributed significantly to the decline in HCV in developed countries. However, lack of awareness, inadequate blood screening facilities, nosocomial transmission and a lack of effective treatments (due to various reasons) have so far been the major factors responsible for seemingly inexorable rise in HCV infection in many developing countries [2, 9].
Methodology
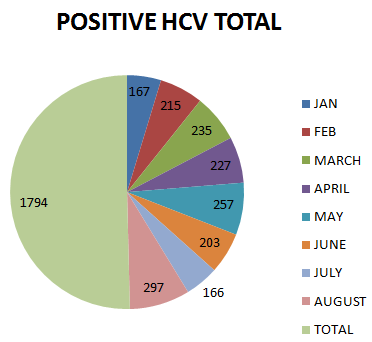
One thousand, seven hundred and ninety four patients were referred to pathological laboratory of KMC teaching hospital khairpure Pakistan, who were suspected for hepatitis HCV, from different area of KMC teaching hospital khairpure Mirs Pakistan catchment area OPDs, and data was collected from January 2017 to august 2017 from which eleven hundred seventy were positive on Elisa method, were screened for HCV (Figure 2). Patients of either sex, with more than thirty years of age were included. From which 1170 HCV were positive on Elisa method (Table 1).
- Results
- Discussion
- August, 2017 (HCV Positive Cases)
- Total Attenepatient
- Positive HCV on
- Positive Cases for HCV ELIZA in
- ELIZA
- Method
- Jan
- 167
- 139
- Feb
- 215
- 111
- March
- 235
- 141
- April
- 227
- 156
- May
- 257
- 188
- June
- 203
- 171
- July
- 166
- 134
- August
- 297
- 130
- Total
- 1794
- 1170
- Months
- OPD
- References
Table 1: Month Wise Eliza Report from January, 2017 to
Conclusion
Data suggest high prevalence of HCV and is alarming situation and silent threat to the population, at KMC Hospital catchment area Khairpure Mirs, Pakistan. The modes of transmission of hepatitis C in Pakistan implicate contaminated needle use in medical care, drug abuse, unsafe blood, and unlawful and without proper equipped laboratories running blood bank, and supplying blood to these areas people in this area and blood product transfusion as the major causal factors. Hence Data suggest a moderate to high prevalence of HBV, at KMC Hospital catchment area Khairpure Mirs, Pakistan.
Data shows during the period of study total number of patients attended the OPD and was advise for Hepatitis C screening, out of 1794, 1170 stands 65% were positive which is very alarming situation in catchment of area of khairpure Medical college hospital khairpure, which coincide with the statement of that is Awareness, improved safety of blood products, the availability of affordable and effective HCV therapies have contributed significantly to the decline in HCV in developed countries. However, lack of awareness, inadequate blood screening facilities, nosocomial transmission and a lack of effective treatments (due to various reasons) have so far been the major factors responsible for seemingly inexorable rise in HCV infection in many developing countries [2, 9]. Meaning that the developing countries are at high risk of hepatitis C, spreading and should be care about and should take strict measures, regarding, the modes of transmission of hepatitis C in Pakistan implicate contaminated needle use in medical care, drug abuse, unsafe blood, and unlawful and without proper equipped laboratories running blood bank and supplying blood to these areas people in this area and blood product transfusion as the major causal factors.
1. Lavanchy D (2011) Evolving epidemiology of hepatitis C virus. Clin Microbiol Infect 17(2): 107-115.
2. Hajarizadeh B, Grebely J, Dore GJ (2013) Epidemiology and natural history of HCV infection. Nat Rev Gastroenterol Hepatol 10(9): 553- 562.
3. Armstrong GL, Wasley A, Simard EP, McQuillan GM,
Kuhnert WL, et al. (2006) The prevalence of hepatitis C virus infection in the United States, 1999 through 2002. Ann Intern Med 144(10): 705-714.
4. Williams IT, Bell BP, Kuhnert W, Alter MJ (2011)
Incidence and transmission patterns of acute hepatitis C in the United States, 1982-2006. Arch Intern Med 171(3): 242-248.
5. Lavanchy D (2009) The global burden of hepatitis C. Liver Int 29(1): 74-81.
6. Waheed Y, Shafi T, Safi SZ, Qadri I (2009) Hepatitis C
virus in Pakistan: a systematic review of prevalence, genotypes and risk factors. World J Gastroenterol 15(45): 5647-5653.
7. Guerra J, Garenne M, Mohamed MK, Fontanet A
(2012) HCV burden of infection in Egypt: results from a nationwide survey. J Viral Hepat 19(8): 560-567.
8. Mohamoud YA, Mumtaz GR, Riome S, Miller D, Abu-
Raddad LJ (2013) The epidemiology of hepatitis C virus in Egypt: a systematic review and data synthesis. BMC Infect Dis 13: 288.
9. Qureshi H, Bile KM, Jooma R, Alam SE, Afridi HU
(2010) Prevalence of hepatitis B and C viral infections in Pakistan: findings of a national survey appealing for effective prevention and control measures. East Mediterr Health J 16: S15-23.
10. Centers for Disease Control and Prevention (CDC)
(2011) Establishment of a viral hepatitis surveillance system--Pakistan, 2009-2011. MMWR Morb Mortal Wkly Rep 60(40): 1385-1390.
11. Umar M, Bushra HT, Ahmad M, Data A, Ahmad M, et al. (2010) Hepatitis C in Pakistan: a review of available data. Hepat Mon 10(3): 205-214.
12. Bosan A, Qureshi H, Bile KM, Ahmad I, Hafiz R (2010)
A review of hepatitis viral infections in Pakistan. J Pak Med Assoc 60(12): 1045-1058.
13. Abbas S, Ali M, Muhammad A, Shaw S, Abbas S (2009)
Frequency of HCV infection and its genotypes among patients attending a liver clinic and voluntary blood donors in a rural area of pakistan. Pak J Med Sci 25(4): 579-582.
14. Ahmed F, Irving WL, Anwar M, Myles P, Neal KR
(2012) Prevalence and risk factors for hepatitis C
virus infection in Kech District, Balochistan, Pakistan: most infections remain unexplained. A cross-sectional study. Epidemiol Infect 140(4): 716-723.
15. Khan A, Tareen AM, Ikram A, Rahman H, Wadood A, et al. (2013) Prevalence of HCV among the young male blood donors of Quetta region of Balochistan, Pakistan. Virol J 10: 83.
16. Janjua NZ, Hamza HB, Islam M, Tirmizi SF, Siddiqui A,
et al. (2010) Health care risk factors among women and personal behaviours among men explain the high prevalence of hepatitis C virus infection in Karachi, Pakistan. J Viral Hepat 17(5): 317-326.
17. Aziz S, Khanani R, Noorulain W, Rajper J (2010)
Frequency of hepatitis B and C in rural and periurban Sindh. J Pak Med Assoc 60(10): 853-857.
18. Gerlach JT, Diepolder HM, Zachoval R, Gruener NH,
Jung MC, et al. (2003) Acute hepatitis C: high rate of both spontaneous and treatment-induced viral clearance. Gastroenterology 125(1): 80-88.
19. Thomson EC, Fleming VM, Main J, Klenerman P,
Weber J, et al. (2011) Predicting spontaneous clearance of acute hepatitis C virus in a large cohort of HIV-1-infected men. Gut 60(6): 837-845.
20. World Health Organization (2014) WHO Guidelines
Approved by the Guidelines Review Committee. Guidelines for the Screening, Care and Treatment of Persons with Hepatitis C Infection. Geneva 124.
21. Jadoon NA, Shahzad MA, Yaqoob R, Hussain M, Ali N
(2010) Seroprevalence of hepatitis C in type 2 diabetes: evidence for a positive association. Virol J 7: 304.
22. Khan NU, Ali I, Ahmad NU, Iqbal A, Rehman LU, et al.
(2011) Prevalence of active HCV infection among the blood donors of Khyber Pakhtunkwa and FATA region of Pakistan and evaluation of the screening tests for anti-HCV. Virol J 8: 154.
23. Aziz S, Hossain N, Karim SA, Rajper J, Soomro N, et al.
(2011) Vertical transmission of hepatitis C virus in low to middle socio-economic pregnant population of Karachi. Hepatol Int 5(2): 677-680.
24. Sami S, Korejo R, Bhutta SZ (2009) Prevalence of hepatitis B and C: a Jinnah Postgraduate Medical
Centre experience. J Obstet Gynaecol Res 35(3): 533- 538.
25. Ali I, Siddique L, Rehman LU, Khan NU, Iqbal A, et al.
(2011) Prevalence of HCV among the high risk groups in Khyber Pakhtunkhwa. Virol J 8: 296.
26. UNODC. Drug Use in Pakistan 2013.
27. ur Rehman L, Ullah I, Ali I, Khan IA, Iqbal A, et al.
(2011) Active hepatitis C infection and HCV genotypes prevalent among the IDUs of Khyber Pakhtunkhwa. Virol J 8: 327.
28. Khan S, Attaullah S, Ayaz S, Niaz Khan S, Shams S
(2011) Molecular epidemiology of HCV among health care workers of khyber pakhtunkhwa. Virol J 8: 105.
29. Waheed A, Zafar-ul-Ahsan FA, Shariff MM, Qayyum A
(2010) Operating in a yellow nation; the frequency of hepatitis B and hepatitis C positive at a tertiary care teaching hospital. J Pak Med Assoc 60(12): 1058- 1060.
- Update on Malariology and Malaria Vaccines
- Addressing Vaccine Hesitancy in the Age of Measles Resurgence: A Mini-Review
- Exploring Barriers and Facilitators of Group Antenatal Care Implementation in Kaduna State, Nigeria: A Qualitative Evaluation
- The Role of IL-11 in Regenerative Medicine and Tissue Engineering
- New Prediction of Mortality rate of Covid -19 According to WHO Estimation
- Measles Vaccine in Kano, Northern Nigeria: Past, Present and Future