Onset of Protection of FeLV Vaccine Containing Purified P45 FeLV-Envelope Antigen after One Single Injection of Primary Vaccination in Cats
Feline Leukaemia Virus (FeLV) is a viral pathogen causing fatal disease in cat populations worldwide, mainly in young kittens with outdoor access. This study aimed to assess the protection against feline leukaemia virus (FeLV), provided by a FeLV vaccine containing purified p45 FeLV-envelope antigen (Leucogen®) after one single injection of primary vaccination in kittens. Twenty-five 9-week-old cats, negative for FeLV antibodies and antigens the day of vaccination, were randomized into two groups. One group of 10 kittens was not vaccinated and kept as control, and one group of 15 animals received one dose of Leucogen® vaccine. The serological response was measured 14 and 21 days post vaccination. Three weeks after the vaccination, all kittens were inoculated by oronasal route with a virulent FeLV-A strain. The development of persistent viraemia was monitored for 15 weeks following inoculation. The animals were clinically monitored closely during the experimental phase. All cats remained in good health, presented physiological growth along the study and did not show any unexpected reaction after vaccination. In the control group, 90% of cats (9/10 cats) developed a persistent infection, confirming that this experimental infection model was valid, since the minimum of 80% required by the European monograph was achieved. On the other side, 73% of the vaccinated cats (11/15 cats) did not develop a persistent infection following the challenge strain inoculation. In the FeLV vaccinated group, 73% of cats were protected from the first vaccine injection. The first injection of primary vaccination with Leucogen® vaccine provided complete protection against FeLV persistent viraemia in 73% of the kittens. The second injection of the primary vaccination is necessary to ensure a complete protection of the whole population and a long lasting immunity. The early protection against FeLV infection conferred after one single injection of primary vaccination with FeLV vaccine containing purified p45 FeLV-envelope antigen could be a contributing factor in the reduction of prevalence of FeLV infection.
Introduction
Feline Leukaemia Virus (FeLV) is a viral pathogen causing fatal disease in feline populations worldwide, mainly in young kittens with outdoor access. Feline leukaemia virus (FeLV) is a gamma retrovirus affecting domestic cats worldwide. After exposure to FeLV, the cats may present a progressive infection with a persistent viraemia and express p27 free viral antigen in the blood. The consequences are FeLV-associated disease with poor prognosis. These cats shed the virus that is a risk of contamination for other cats. In some other cats, viraemia may be overcome by the immune system. The cats present a regressive infection with a transient viraemia or an abortive infection with virus elimination [1, 2, 3]. Clinical signs of a FeLV infection are variable. It can cause neoplasia (mainly lymphoma and leukaemia), bone marrow suppression (mainly non-regenerative anaemia, thrombocytopenia, neutropenia, pancytopaenia), chronic or recurrent infection suggesting immunosuppression, chronic gingivostomatitis, immune-mediated haemolytic anaemia, neurological signs, reproductive disorders, fading kitten syndrome and other disorders such as immune-mediated uveitis or erosive polyarthritis [2].
The use of vaccines, combined with the increase of routine testing contributed to the reduction of the prevalence of FeLV infection in domestic cat populations [2, 4, 5]. Various vaccines have been commercialised and have been shown to protect against persistent viraemia [6, 7, 8, 9]. Nevertheless, this prevalence is still high in some areas and it can exceed 20% in high-risk cat populations, confirming the need for effective vaccines [2, 10].
The risk factors are mixed breed, free-ranging or feral cats, cats from households with FeLV-positive cats, cats from areas with high FeLV-prevalence. Transmission of infection occurs through viral shedding (mainly saliva but also nasal secretions, milk, faeces) by FeLV-infected cats, mainly through friendly contact (mutual grooming), but also through biting and blood transfusion [2]. As FeLV infects predominantly young animals, it is important that these vaccines protect as early as possible [10].
The purpose of this study was to investigate the protection against Feline Leukaemia Virus (FeLV) provided by FeLV vaccine containing purified p45 FeLV-envelope antigen (Leucogen®), three weeks after one single injection of primary vaccination in kittens.
Methods
The design of the study received a favourable opinion of the ethics committee. The study was accepted by the competent authority. The study was conducted according to the European Pharmacopoeia. The design was based on the requirements of the guidelines for the evaluation of efficacy of veterinary vaccines. This included the conduct of the vaccination, followed by a challenge with virulent virus and subsequent follow-up of the animals. The number of animals per test group had been decided to correspond strictly to the number of animals recommended by the European Pharmacopoeia. The animals were housed and cared for in compliance with current regulation and after approval by the Ethics Committee.
Animals and Housing
Twenty-five specific-pathogen free European kittens (63-67 days old; average body weight of 1.02 ± 0.18 kg on day 0, ranging from 0.7 to 1.5 kg) were allocated into two groups: group A (vaccinated with Leucogen®), group B (control, not vaccinated). The cats were acclimated for 5 days to the animal housing conditions before vaccination. The animals were fed with a complete diet for growing kittens, and food and water were provided ad libitum. On the day of the challenge strain inoculation, feed and water were withdrawn prior to sedation and returned when all cats had recovered from sedation.
Vaccine and Vaccination
Leucogen® has been granted a European marketing authorisation (centralised procedure). It is presented as a liquid fraction containing the recombinant FeLV-envelope antigen p45 (derived from FeLV gp70) with aluminium hydroxide gel and Quillaja saponaria QA-21 adjuvants. The vaccine vials were stored at temperature between + 2°C and + 8°C before administration.
The cats were allocated into two groups according to age, weight, sex and avoiding having a group consisting of animals from the same litter. Cats assigned to group A received each one dose of Leucogen® vaccine administered subcutaneously halfway between the right shoulder and the right hip (on the flank). The injection site was clipped and disinfected prior to vaccination. Cats assigned to group B were not vaccinated.
Challenge
Three weeks after vaccination, at day 21 (Week Post Challenge 0), all cats were inoculated with a virulent strain of Feline Leukaemia virus, FeLV subgroup A (FeLV-A 13.04). The origin of this challenge strain seed is cells infected with FeLV-A, provided by Cambridge Biosciences Corporation. They were anesthetized, and 1 ml of a viral suspension was inoculated per cat by oro-nasal route (0.25 ml in each nostril and 0.5 ml in the mouth). They were then observed for 15 weeks, until day 126 (Week Post Challenge 15). This FeLV
subgroup A strain is the dominant subgroup found in cats. The oronasal route is selected to abide by the European Pharmacopoeia and also to try to be as close as possible to the natural infection. The transmission by FeLV-infected cats occurs through viral shedding mainly in saliva and mainly through friendly contact.
Monitoring and Samples
During the whole study, cats were observed daily for any abnormal behaviour, clinical sign, aspect of faeces, food intake, and general health status. Furthermore, a complete clinical examination, including weighing and rectal temperature measurement, was carried out on a weekly basis. Additional clinical examinations were conducted when clinical findings were observed. Blood samples of at least 2 mL were collected at day 0 before vaccine administration and then at day 14. On the day of challenge (WPC0), blood collection was carried out prior to virus inoculation. After the challenge, one blood sample was collected on a weekly basis from day 42 (WPC3) till day 126 (WPC15). Serum was collected by these samples and stored at kept frozen (≤ 15°C) until analysis.
Laboratory Analyses and Scoring
Titration of Antibodies against FeLV p45 Protein: Antibodies against FeLV p45 protein were dosed using ELISA test in serum samples collected during the vaccinal phase. Plates were firstly coated with the FeLV p45 protein, identical to that contained in Leucogen® vaccine (0.5 µg/well in carbonate buffer). After blocking of non-specific sites with 1% BSA TNE buffer, several dilutions of each serum (three fold serial dilutions in 0.1% BSA TNE buffer: 1/150th to 1/36450th) were added to the plate. Positive and negative sera were diluted the same way and used as controls. After incubation, the antibodies specifically bound to the p45 protein were revealed with a specific peroxidase conjugated antibody (ABTS coloration). The titre corresponding to the first dilution with an optical density at 405 nm inferior to 0.5 was recorded. The positivity threshold was set up at 1/450.
Detection of FeLV p27 Antigen Protein: Detection of FeLV p27 protein in serum samples collected during the challenge phase was performed using the commercial IDEXX ELISA FeLV Antigen test kit (Référence IDEXX du kit: 99-07896). This test kit uses 12-well strips coated with anti-p27 antibodies. Samples were added in the wells previously coated and incubated with anti-FeLV antibodies conjugated to HorseRadisch PerOxidase (HRPO). If present in the sample, the FeLV antigen binded with both the antibody coated in the well and the HPRO/antibody, conjugate. After washing the wells, the substrate and the chromogen were added. The change in blue colour of the patch corresponding to “Ag FeLV” indicates the presence of FeLV-derived P27 antigens in the sample tested. The test is valid if the possible appearance of background colour doesn’t prevent the reading, the patch corresponding to the positive control turns in blue colour and the patch corresponding to the negative control is not (or very slightly) coloured. In the case of a valid test, the result is negative if only the patch corresponding to the positive control turns in blue colour. In case of a valid test, the result is positive if the patch corresponding to the positive control and the patch corresponding to “Ag FeLV” turn in blue colour.
Statistical Tests: The statistical analysis is performed using SAS 9.3 software. The proportion of cats persistently infected in vaccinated and control groups is compared using Fisher’s Exact Test. A p value < 0.05 is considered significant.
Results
Vaccination Phase (day 0 to day 21)
Clinical Monitoring and Safety: During the vaccinal phase, the cats remained in good health, with a normal increase of their body weight and a rectal temperature within the physiological range. No specific clinical findings were observed during or shortly after vaccination. No unexpected general or local reactions were reported after vaccination. On a single occasion (day 28), a pin head-sized subcutaneous swelling at the injection site (right thoracic wall) was observed in one out of 15 vaccinated animals. The injection site swelling was movable and not painful. This transient finding may be considered to be due to the vaccination and represents a not unexpected finding.
Immune Response: Prior to vaccination, all cats were free from antibodies against FeLV p45 protein. The control cats remained seronegative from day 0 to day 21. After vaccination with Leucogen®, 4 cats out of 15 seroconverted to the vaccine protein from day 14, with antibody titres ranging from 1/450 to 1/1350. 3 additional cats seroconverted from day 21, with antibody titres of 1/450.
Post-Challenge Phase (day 21 to day 126)
Clinical Monitoring: After inoculation of the challenge strain, the cats remained in good health, with the body weight increase expected for cats at this age and a rectal temperature within the physiological range. During this 15- week period, enlarged superficial lymph nodes (lymph node mandibularis, and popliteus superficialis) were recorded after the inoculation in both groups. In the control group, 9 out of 10 (90%) not vaccinated cats showed enlarged peripheral lymph nodes for at least 7 weeks, consecutive or not. In the vaccinated group, peripheral lymph nodes appeared enlarged in only 8 out of 15 cats (53%). The challenge with virulent FeLV led to the occurrence of enlarged peripheral lymph nodes at a higher incidence in the control group (9/10 cat i.e. 90%) compared to the vaccinated group (8/15 cats i.e. 53%). FeLV infection related clinical signs (oedematous swelling at the head, moderately impaired general condition, enlarged superficial lymph nodes, pale mucosa, no feed consumption) were observed in one control animal from D56 to D70. Similar findings were not found in the animals of the vaccinated group.
P27 Antigenemia Follow-Up: The number and percentage of animals with circulating P27 viral antigen in the blood at each time point and the persistent infection status at the end of the study are summarised in Table 1. All kittens were negative for FeLV p27 antigen prior to inoculation of the challenge strain (WPC0). Three weeks later, on WPC3, 80% of the control cats (8/10) and 33% of the vaccinated cats (5/15) were positive for FeLV p27 antigen. During the rest of the post-challenge phase, the percentage of positive animals ranged from 70 to 90% in the control group whereas it dropped to 27% in the vaccinated group from WPC4 and remained stable until the end of the study.
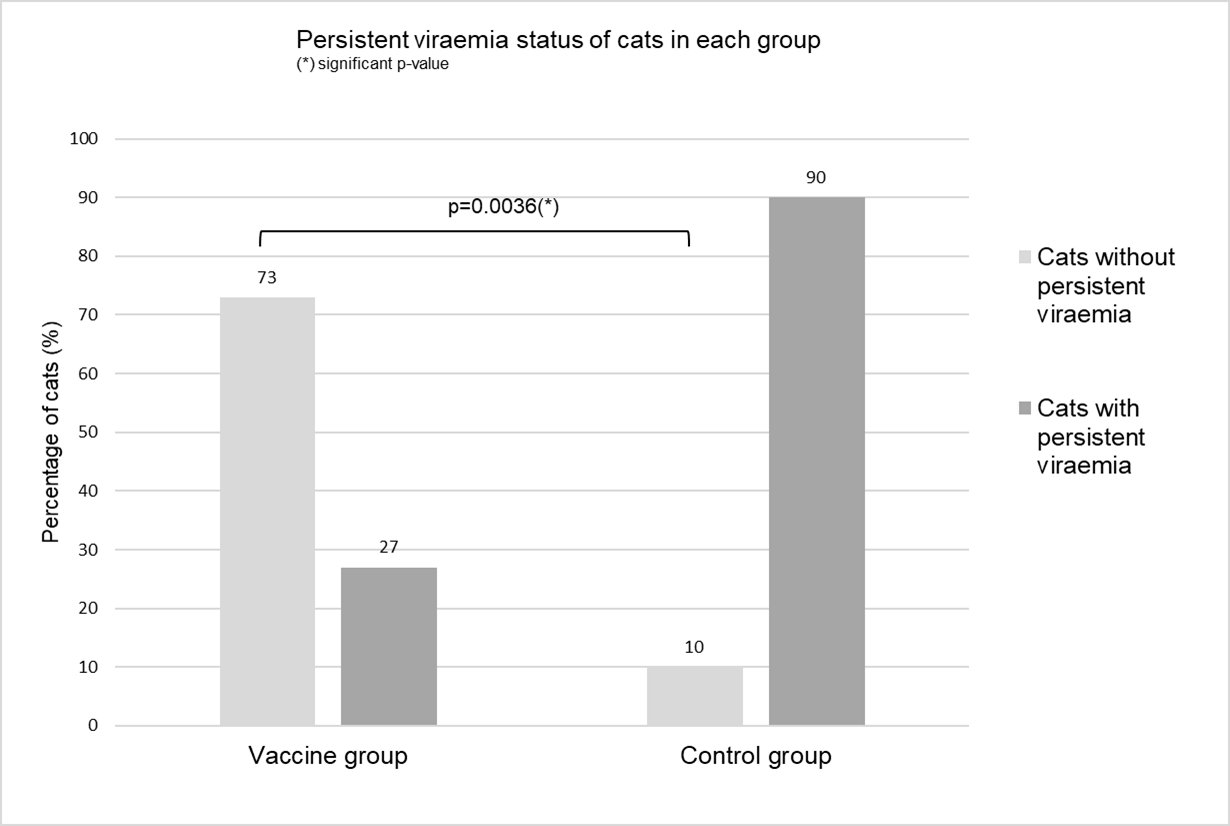
Persistent Viraemia Status: According to the European Pharmacopoeia Monograph n°1321 (Feline Leukemia Vaccine Inactivated), a cat is considered as persistently infected if it shows positive P27 antigenaemia either during three consecutive weeks or on five occasions, consecutive or not, between the third and the fifteenth week post-challenge. The persistent infection status was determined for each cat (Table 1). Following administration of the virulent FeLV strain, 9 control cats out of 10 (90%) and 4 Leucogen® vaccinated cats out of 15 (27%) met the criteria for a persistent infection. According to the European Monograph, a FeLV challenge was valid when at least 80% of control animals revealed a persistent infection. The validity of this experimental infection model used for assessing FeLV vaccine efficacy is confirmed by the results obtained in the control group, as 90% of the control cats developed a persistent infection. After one injection of Leucogen® vaccine, 11 vaccinated cats out of 15 (73%) did not develop a FeLV persistent viremia. Statistical analyses showed that the proportion of cats persistently infected was significantly lower in the vaccinated group than in the control group (p=0.0036). The status of cats regarding persistent infection post challenge were presented in Figure 1.
Vaccine Efficacy Assessment: Persistent viraemia preventable fraction was calculated as follows: (% of controls with a persistent infection - % of vaccinates with a persistent infection) / % of controls with a persistent infection. The vaccine efficacy measured as the persistent viraemia preventable fraction for Leucogen® vaccine was equal to 70%.
| Group | Identifi cation | Weeks post-challengea | Persi stent infec tion | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 0 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | |||
| Leucogen® (n=15) | 1b | (-) | + | + | + | + | + | + | + | + | + | + | + | + | + | Yes |
| 2b | (-) | (-) | (-) | (-) | (-) | (-) | (-) | (-) | (-) | (-) | (-) | (-) | (-) | (-) | No | |
| 3 | (-) | + | (-) | (-) | (-) | (-) | (-) | (-) | (-) | (-) | (-) | (-) | (-) | (-) | No | |
| 4 | (-) | + | + | + | + | + | + | + | + | + | + | + | + | + | Yes | |
| 5 | (-) | + | + | + | + | + | + | + | + | + | + | + | + | + | Yes | |
| 6 | (-) | + | + | + | + | + | + | + | + | + | + | + | + | + | Yes | |
| 7b | (-) | (-) | (-) | (-) | (-) | (-) | (-) | (-) | (-) | (-) | (-) | (-) | (-) | (-) | No | |
| 8 | (-) | (-) | (-) | (-) | (-) | (-) | (-) | (-) | (-) | (-) | (-) | (-) | (-) | (-) | No | |
| 9b | (-) | (-) | (-) | (-) | (-) | (-) | (-) | (-) | (-) | (-) | (-) | (-) | (-) | (-) | No | |
| 10 | (-) | (-) | (-) | (-) | (-) | (-) | (-) | (-) | (-) | (-) | (-) | (-) | (-) | (-) | No | |
| 11 | (-) | (-) | (-) | (-) | (-) | (-) | (-) | (-) | (-) | (-) | (-) | (-) | (-) | (-) | No | |
| 12b | (-) | (-) | (-) | (-) | (-) | (-) | (-) | (-) | (-) | (-) | (-) | (-) | (-) | (-) | No | |
| 13b | (-) | (-) | (-) | (-) | (-) | (-) | (-) | (-) | (-) | (-) | (-) | (-) | (-) | (-) | No | |
| 14b | (-) | (-) | (-) | (-) | (-) | (-) | (-) | (-) | (-) | (-) | (-) | (-) | (-) | (-) | No | |
| 15 | (-) | (-) | (-) | (-) | (-) | (-) | (-) | (-) | (-) | (-) | (-) | (-) | (-) | (-) | No | |
| Number (%) of positive cats c | 0 (0%) | 5 (33%) | 4 (27%) | 4 (27%) | 4 (27%) | 4 (27%) | 4 (27%) | 4 (27%) | 4 (27%) | 4 (27%) | 4 (27%) | 4 (27%) | 4 (27%) | 4 (27%) | 4 (27%) | |
| Control (n=10) | 16 | (-) | + | + | + | + | + | + | + | + | + | + | + | + | + | Yes |
| 17 | (-) | + | + | + | + | + | + | + | + | + | (-) | + | (-) | (-) | Yes | |
| 18 | (-) | + | + | + | + | + | + | + | + | + | + | + | + | + | Yes | |
| 19 | (-) | + | + | + | + | + | + | + | + | + | + | + | + | + | Yes | |
| 20 | (-) | + | + | + | + | + | + | + | + | + | + | + | + | + | Yes | |
| 21 | (-) | + | + | (-) | (-) | + | (-) | (-) | + | + | + | + | + | + | Yes | |
| 22 | (-) | + | + | + | + | + | + | + | + | + | + | + | + | + | Yes | |
| 23 | (-) | (-) | (-) | + | + | + | + | + | + | + | (-) | + | + | + | Yes | |
| 24 | (-) | + | + | + | (-) | + | + | + | + | (-) | + | + | + | + | Yes | |
| 25 | (-) | (-) | + | + | (-) | (-) | (-) | (-) | (-) | (-) | (-) | (-) | (-) | (-) | No | |
| Number (%) of positive cats c | 0 (0%) | 8 (80%) | 9 (90%) | 9 (90%) | 7 (70%) | 9 (90%) | 8 (80%) | 8 (80%) | 9 (90%) | 8 (80%) | 7 (70%) | 9 (90%) | 8 (80%) | 8 (80%) | 9 (90%) |
Table 1: Post-Challenge FeLV p27 antigenaemia status and persistent infection status of cats in each group.
a: (-) absence of circulating FeLV p27 protein in the blood; (+) detection of circulating FeLV p27 protein in the blood b: cat showing antibody response post-vaccination c Number (percentage) of cats positive for FeLV p27 antigen or positive for persistent infection Table 1: Post-Challenge FeLV p27 antigenaemia status and persistent infection status of cats in each group.
Discussion
As young kittens are more susceptible to FeLV infection than adults, rapid onset of immunity after vaccination is particularly important. Thus, efficacy of Leucogen® vaccine was investigated after a single injection, corresponding to the first injection of a primary vaccination protocol, through a virulent FeLV challenge in kittens.
In the present trial, nine-week-old kittens were immunised with Leucogen® vaccine and challenged with a virulent FeLV strain at twelve weeks of age. The FeLV strain used for this challenge belongs to subgroup A, the dominant subgroup found in all infected cats [2]. This strain was therefore considered relevant to assess protection against any FeLV field strain. Moreover, oro-nasal inoculation was performed in order to have a model as close as possible to the natural conditions of infection. In natural conditions, the infection occurs mainly via saliva, mainly through friendly contact [2]. In these conditions, 90% of the control cats developed a persistent viraemia, confirming the validity of the experimental infection model used in our study for assessing FeLV vaccine efficacy in young animals.
In the present study, 73% of the vaccinated kittens did not develop persistent viraemia following challenge strain inoculation. In these experimental conditions, the preventable fraction of Leucogen® vaccine was calculated as 70%. The P27 persistent viraemia preventable fraction was considered as a measure of vaccine efficacy. This indicates that a majority of kittens vaccinated with Leucogen® are protected from the first vaccine injection. However, even if this early protection has been shown in young kittens, known to be the most susceptible population, we can suppose that a single administration induces a similar efficacy in adult cats. Induction of very rapid protective immune response could be due to the presence of the purified extract of Quillaja saponaria adjuvant contained in Leucogen® vaccine [11, 12]. Indeed, it has been shown that saponin-based adjuvants strongly stimulate humoral and cell-mediated immunity, enhance the speed and the duration of the immune response [11, 13], and thus could contribute to early induced-vaccine protection [14, 15]. A similar virulent challenge trial, Gueguen, et al. [16] showed a prevention of persistent infection in 9 out of 10 (90%) cats vaccinated with 2 injections of Leucogen®, corresponding to a prevention fraction of 87.5% [16]. Therefore, the second injection of the primary vaccination remains necessary to ensure a complete protection of the whole population as well as a long-lasting immunity. Following a first booster vaccination one year after the primary vaccination course with Leucogen®, a duration of immunity of 3 years has been demonstrated [17, 18]. Serological analyses performed post-vaccination showed a moderate antibody response to the FeLV p45 vaccine protein in 7 kittens out of 15. Moreover, there was no correlation between antibody secretion and protection since 1 kitten that seroconverted after vaccination, developed persistent infection after challenge, and conversely 5 kittens that had no detectable antibodies were protected. These observations confirm the strong role of the cell-mediated immunity in the control of this viral infection as previously described [13, 14]. A complete and detailed analysis of cell- mediated response after vaccination, particularly of the cytotoxic T-lymphocyte response, would lead to a better understanding of these mechanisms and identification of relevant markers of protection [19, 20].
During our laboratory challenge experiment, cats were classified as infected according to their status towards persistent viraemia. The latter was characterized by continuous expression of free p27 viral antigen in the blood. However, no data is available on Leucogen® impact on transient viraemia. Transient viraemia could be detected by the measurement of FeLV proviral DNA in the blood. [4]. It can thus be assumed that the animals protected against persistent viraemia in the present study would have also been negative for proviral DNA and thus for transient viraemia. Determination of the proviral DNA by Polymerase Chain Reaction would have been useful in our study to confirm this hypothesis. Leucogen® vaccine is a monovalent vaccine that can be used mixed with Feligen® RCP a trivalent vaccine against feline calicivirosis, feline parvovirus, and feline herpesvirus produced by the same manufacturer (the combination is named Leucofeligen® FeLV/RCP). A similar efficacy of Leucogen® vaccine has been demonstrated when it is administered alone or in combination with Feligen® RCP [16, 18].
Conclusion
This study investigated the efficacy of Leucogen®, a FeLV vaccine containing purified P45 FeLV-envelope antigen, to protect kittens against FeLV after the first injection of the primary vaccination protocol. This study demonstrated that Leucogen® induces a protection against FeLV persistent viraemia in 73% of the cats after a single injection of primary vaccination. The second injection of the primary vaccination is necessary to ensure a complete protection of the whole population and a long lasting immunity. The early protection to FeLV infection conferred after one single injection of primary vaccination with Leucogen®, could be a contributing factor in the reduction of prevalence of FeLV infection.
Conflicts of Interest, Acknowledgements and Funding
All the authors of this paper were employed by Virbac.
References
-
Hartmann K (2012) Clinical aspects of feline retroviruses: a review. Viruses 4(11): 2684-2710.
-
Lutz H, Addie D, Belák S, Boucraut-Baralon C, Egberink H, et al. (2009) Feline leukaemia. ABCD guidelines on prevention and management. J Feline Med Surg 11(7): 565-574.
-
Torres A, Mathiason CK, Hoover EA (2005) Re- examination of feline leukemia virus: host relationships using real-time PCR. Virology 332(1): 272-283.
-
Day MJ, Horzinek MC, Schultz RD, Squires RA (2016) WSAVA Guidelines for the vaccination of dogs and cats. J Small Anim Pract 57(1): E1-E45.
-
Horzinek MC (2006) Vaccine use and disease prevalence in dogs and cats. Veterinary Microbiology 117(1): 2-8.
-
Marciani DJ, Kensil CR, Beltz GA, Hung CH, Cronier J, et al. (1991) Genetically-engineered subunit vaccine against feline leukaemia virus: protective immune response in cats. Vaccine 9(2): 89-96.
-
Stuke K, King V, Southwick K, Stoeva MI, Thomas A, et al. (2014) Efficacy of an inactivated FeLV vaccine compared to a recombinant FeLV vaccine in minimum age cats following virulent FeLV challenge. Vaccine 32(22): 2599- 2603.
-
Patel M, Carritt K, Lane J, Jayappa H, Stahl M, et al. (2015) Comparative Efficacy of Feline Leukemia Virus (FeLV) Inactivated Whole-Virus Vaccine and Canarypox Virus- Vectored Vaccine during Virulent FeLV Challenge and Immunosuppression. Clin Vaccine Immunol 22(7): 798- 805.
-
Grosenbaugh DA, Frances-Duvert V, Abedi S, Feilmeier B, Ru H, et al. (2017) Efficacy of a non-adjuvanted recombinant FeLV vaccine and two inactivated FeLV vaccines when subject to consistent virulent FeLV challenge conditions. Biologicals 49: 76-80.
-
Wilson S, Greenslade J, Saunders G, Holcroft C, Bruce L, et al. (2012) Difficulties in demonstrating long term immunity in FeLV vaccinated cats due to increasing age- related resistance to infection. BMC Vet Res 8: 125.
-
Rajput ZI, Hu SH, Xiao CW, Arijo AG (2007) Adjuvant effects of saponins on animal immune responses. J Zhejiang Univ Sci B 8(3): 153-161.
-
Aido V, Pliasas VC, Neasham PJ, North JF, McWhorter KL, et al. (2021) Novel vaccine technologies in veterinary medicine: A Herald to human medicine vaccines, Front Vet Sci 8: 654289.
-
Greene CE, Schultz RD (2006) Immunoprophylaxis. In: Greene CE, et al. (Eds.), Infectious Diseases of the Dog and Cat. 3rd(Edn.), Saunders Elsevier, St Louis, pp: 1069- 1119.
-
Saalmuller A (2006) New understanding of immunological mechanisms. Veterinary Microbiology 117(1): 32-38.
-
Chalmers WSK (2006) Overview of new vaccines and technologies. Veterinary Microbiology 117(1): 25-31.
-
Gueguen S, Martin V, Bonnet L, Saunier D, Mähl P, et al. (2000) Safety and efficacy of a recombinant FeLV vaccine combined with a live feline rhinotracheitis, calicivirus and panleukopenia vaccine. Vet Rec 146(13): 380-381.
-
Jarrett O, Ganière JP (1996) Comparative studies of the efficacy of a recombinant feline leukaemia virus vaccine. Vet Rec 138(1): 7-11.
-
Hoffmann-Lehmann R, Cattori V, Tandon R, Boretti FS, Meli ML, et al. (2007) Vaccination against the feline leukaemia virus: outcome and response categories and long term follow-up. Vaccine 25(30): 5531-5539.
-
Flynn JN, Hanlon L, Jarrett O (2000) Feline leukaemia virus: protective immunity is mediated by virus-specific cytotoxic T lymphocytes. Immunology 101(1): 120-125.
-
Flynn JN, Dunham SP, Watson V, Jarret O (2002) Longitudinal analysis of Feline Leukemia Virus-Specific Cytotoxic T lymphocytes: correlation with recovery from infection. Journal of Virology 76(5): 2306-2315.
- Update on Malariology and Malaria Vaccines
- Addressing Vaccine Hesitancy in the Age of Measles Resurgence: A Mini-Review
- Exploring Barriers and Facilitators of Group Antenatal Care Implementation in Kaduna State, Nigeria: A Qualitative Evaluation
- The Role of IL-11 in Regenerative Medicine and Tissue Engineering
- New Prediction of Mortality rate of Covid -19 According to WHO Estimation
- Measles Vaccine in Kano, Northern Nigeria: Past, Present and Future