Adverse Effects Following Immunization (AEFI) with CovaxinTM and Vaccine Reluctance among Adolescent Teenagers (14-18 Years) and Their Parents: A Descriptive Cross-Sectional Study in Delhi, India
Objective: Mild adverse effects following immunization (AEFI) are inevitable and generally tolerable. The primary objective of study is to know the prevalence of AEFI with COVID-19 vaccine (CovaxinTM ) in age group between 14-18 years. Study also aimed to assess the factors responsible for vaccine hesitancy among adolescents and their parents. Methodology: The prospective observational study was conducted using self structured validated Google form questionnaire among the CovaxinTM recipients (N= 262) between June 2022 to August 2022. IBM-SPSS version 22 Chicago, USA was used for data analysis. Observations and Results: Around 50% and 26.3% participants reported at least one of the AEFI following first and second dose of CovaxinTM respectively. No severe life threatening adverse events were reported with any dose. The common AEFI were pain at the injection site (13%, 7.3%), fever (37%, 19.1%), and generalized body aches (27.1%, 11.1%) respectively following first and second dose. The prevalence of AEFI was higher following the first dose compared to the second dose except for hair fall (7.2%). Hair fall was found statistically significant (p
Introduction
Immunization against Covid-19 is relatively new to curb Corona virus pandemic, which originated in Wuhan, China in 2019 [1]. A variety of vaccines against Covid-19 were developed using fast track technology globally and received emergency approvals for use (EAU) including first indigenous vaccine (CovaxinTM) of India. CovaxinTM (BBV152, whole virion inactivated vaccine) was the second Covid-19 specific vaccine preceded by Covishield™ (adenovirus vector vaccine) in India [2].
Initially Covishield™ developed by Serum Institute of India and Oxford-AstraZeneca became part of vaccination drive with effect from on January 16, 2021 in Health care professionals (HCPs) and front line workers (FLWs) [3]. On Jan 3, 2021, 'Covaxin™' (BBV152, Bharat Biotech) got approval for emergency use in adult population by DCGI [4]. The safety data on AEFI with Covaxin™ is required to educate public, avoid misinformation, which will overcome vaccine hesitancy [5].
AEFI can be defined as any untoward medical occurrence following immunization which does not necessarily have a causal relationship to the vaccine [5]. Vaccination against Covid-19 is new and therefore needs to be continuous monitoring of AEFI through post marketing as surveillance [6]. The purpose of vaccine surveillance is to identify serious and unexpected AEFI, to reduce the associated morbidity and mortality, to educate public, avoid misinformation and to overcome vaccine hesitancy among eligible population [5, 7, 8].
Till date adequate studies have been done on AEFI by Covid-19 vaccines in adult and elderly populations. But safety data on AEFI using Covaxin™ among children and adolescents is relatively inadequate. This is to note that only Covaxin™, which is made available for vaccinating Indian population under 18 years of age at the time of study proposal submission. There is an urgent need to generate safety data on Covaxin™ among teenagers in India.
Vaccine reluctance/hesitancy has also been seen among adolescents and parents. Vaccine reluctance is hesitancy of people to accept vaccine that has been made safe and effective to protect them against an Infectious disease [9].
The present study is a descriptive cross-sectional study conducted on Indian adolescent teenagers (14-18 years of age), willing to participate in the study. The primary objective of the study is to estimate prevalence of AEFI with Covaxin™ among adolescents between ages 14-18 years. The secondary objective is to determine factors responsible for causing vaccine hesitancy among adolescents (14-18 years of age) and their parents during mass vaccination drive in India. Study has been conducted to bridge the gaps in literature pertaining to AEFI and vaccine reluctance, targeted exclusively to 14-18 years of age group. The data generated will be beneficial to all stakeholders and policy makers for opting right decisions for strengthening mental and physical well-being of teenagers, following re-opening of schools almost after 2 years in India. This could also prove useful for motivating, creating awareness and convincing parents and school going children about benefits of getting vaccinated, to avoid future lockdowns in schools for their positive physical and mental health.
Material and Methods
Study Type, Design and Sample Size
The present survey was an original research study with descriptive cross-sectional design using a self structured questionnaire. We used a sample size of 262 participants between age 14-18 years, with 10% adjustment for non responders/incomplete responses using the set formula.
Formula:
$$n = Z^2 p \frac{(1 - p)}{d^2}$$
Z= Confidence level (95%)
p= 20% (expected proportion from previous pilot studies)
d= 5% of true value (0.05)
Inclusion and Exclusion Criteria
Survey included adolescents (14-18 years), both male and female, who had received at least 1 dose of vaccine and belong to Delhi, India. Those who did not give consent and assent were excluded from study.
Time Frame of Study
The time frame for the study was 4-5 months. Sample collection was completed in 2 months from the date of receiving Ethical clearance and data analysis and STS-ICMR report writing was done in subsequent months.
Methodology
Questionnaire was validated for the content and face validation before conducting the study, by getting the questionnaire filled among 20 known participants. Questionnaire was edited and updated as per feedback by participants. These 20 participants were excluded from the main study. The final questionnaire was approved by Institutional Ethical Committee (IEC), Jamia Millia Islamia, and Delhi. (IEC approval no.2/6/390/JMI/IEC/2022).
A questionnaire link was generated and request message to fill the Google questionnaire form was shared in Whatsapp groups and emails among known and unknown contacts to achieve target sample size. Questionnaire with information regarding purpose of study and benefits of study was accessed by participants by clicking on the link shared as mentioned above. Participants were invited to participate following acceptance to informed consent/assent as asked on first page of Google form. Each participant was asked multiple choice questions (MCQs) related to demography followed by MCQs related to CovaxinTM including reasons for any hesitancy/reluctance for vaccination at any time. Participants submitted their responses at last page after attempting questionnaire by clicking on ‘Submit’ icon. The acknowledgement was provided to each participant on submission of responses.
Responses received were saved in Google drive and downloaded in a Microsoft excel spread sheet which was later transferred to IBM-SPSS version 22 Chicago, USA for statistical analysis. Quality control of data collection was done and maintained by checking entries/ responses on daily basis by principal Investigator and co-investigator. Personal identity of participants was never revealed at any point of time of study conduct.
Data Analysis
Results from the data obtained were depicted in the form of tables, charts and graphs as percentages. IBM-SPSS version 22 Chicago, USA was used for analysis of results.
Results
Following are the observations and results depicted in the form of tables, pie charts and graphs as shown below.
The mean age of the participants (N=262) was 16 years (ranging from 14-18 years). Out of 262 participants, 7.3% reported history of pre-existing medical illness/co- morbidity. Around 100 (38.2%) participants had to take any form of analgesic drug before or after the vaccination. None of the participants reported any active clinical symptom at the time of vaccination (Table 1).
| Demographic Variables | Observations | Prevalence, N= 262 (Percentage %) |
|---|---|---|
| Age | 14 years | 22 (8.4%) |
| 15 years | 35 (13.4%) | |
| 16 years | 45 (17.2%) | |
| 17 years | 37 (14.1%) | |
| 18 years | 123 (46.9%) | |
| Area of residence in Delhi | North Delhi | 151 (57.6%) |
| South Delhi | 30 (11.5%) | |
| East Delhi | 38 (14.5%) | |
| West Delhi | 43 (16.4%) | |
| Educational level | 9th class | 18 (6.9%) |
| 10th class | 49 (18.7%) | |
| 11th class | 23 (8.8%) | |
| 12th class | 63 (24%) | |
| Undergraduate | 94 (35.9%) | |
| Any other | 15 (5.7%) | |
| Pre-existing self-reported Co-morbidities (diabetes, hypertension, bronchial asthma, vitiligo, cutaneous allergy, polycystic ovarian disease PCOD, thyroid dysfunction, liver function abnormality, Recurrent infections, renal stones, migraine etc) | Present | 19 (7.3%) |
| Not present | 243 (92.7%) | |
| Analgesic, Antipyretic medicines use (pre or post vaccination) | Consumed | 100 (38.2%) |
| Not consumed | 162 (61.8%) |
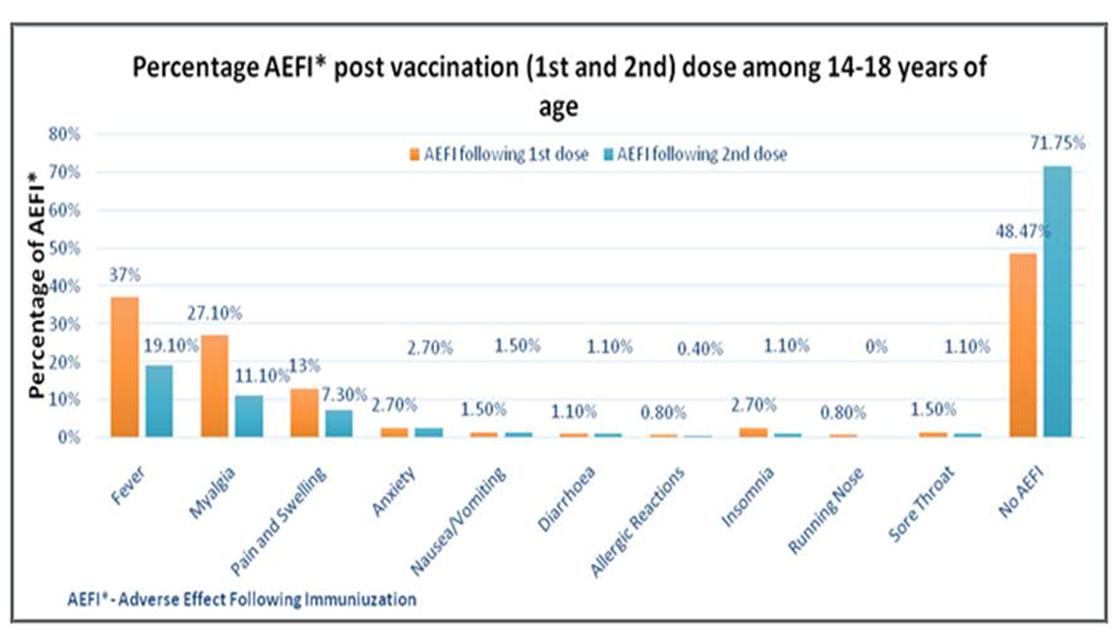
Table I: Demographic details of participants. N=Sample size The AEFI symptoms following first and second dose of CovaxinTM, experienced by the participants are shown in Figure 1. Out of 262 participants, 92 (35%) reported local symptoms of pain and swelling following first dose in contrast to 52 (20%) participants experiencing pain and swelling following second dose. The most common symptom was fever in 97 (37%) and in 50, (19.1%) followed by generalized body ache in 71 (27.1%) and in 29, (11.1%) following first and second dose of vaccine respectively (Figure 1).
Self-Reported AEFI by Participants
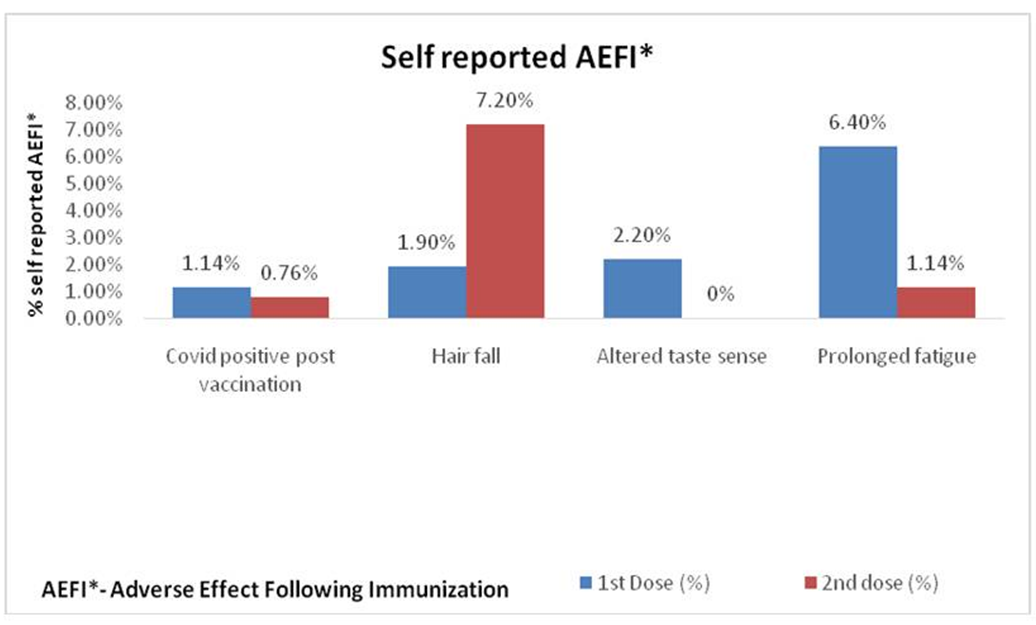
The self-reported AEFI were; Covid-19 positive status among 3 participants, (1.14%) and 2 participants (0.76%) following first and second dose respectively. Excess hair fall within 1 month of first and second dose of vaccination was reported by 5 participants (1.9%) and 19 participants, (7.2%) respectively. Hair fall after the second dose was found to be statistically significant at p<0.05. Altered taste sense was reported only after the first dose of Covid-19 vaccine among 6 participants (2.2%). Generalized fatigue and weakness was to the extent of 17 (6.4%) and 3 (1.14%) following first and second dose respectively (Figure 2).
Duration of AEFI
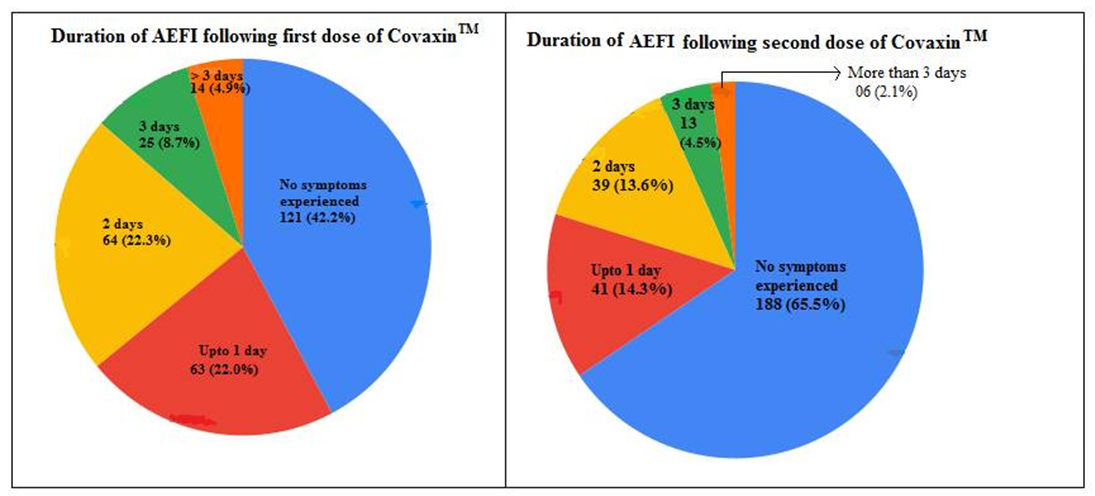
Majority of the participants (22.3%) experienced AEFI symptoms up to 2nd day and very few 4.9% beyond 3 days following first dose of Covid-19 vaccine. Only 2.1% of participants experienced AEFI symptoms beyond 3 days following vaccination with the 2nd dose. Overall duration of persistence of AEFI was lower following 2nd dose of vaccination. A majority of the study participants reported complete recovery within 24 hours following the first and second dose of vaccine. Complete recovery was seen in all the study participants maximum by 12-14 days post vaccination (Figure 3).
There was statistically significant role of social media in 92 (35.1%), friends/relatives/family in 55 (21%) and television (news) in 16 (6.1%) in affecting the psychology of participants where p<0.05 found significant. Irrespective of completing the vaccine course (two shots), 52 (20%) of study participants were reluctant /hesitant to take vaccine shot pre or post first shot.
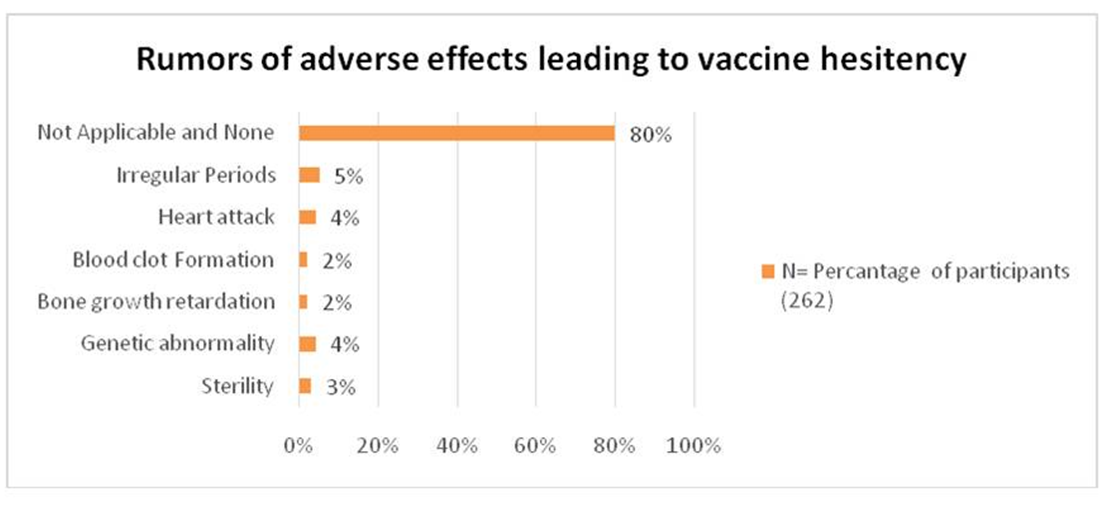
The rumors of adverse effects that led to vaccine hesitancy were irregular periods in 16(5%), heart attack in 12(4%), blood clot in 5(2%), bone growth retardation in 7(2%), genetic abnormality 11(4.2%), and sterility in 8 (3.1%) (Figure 4).
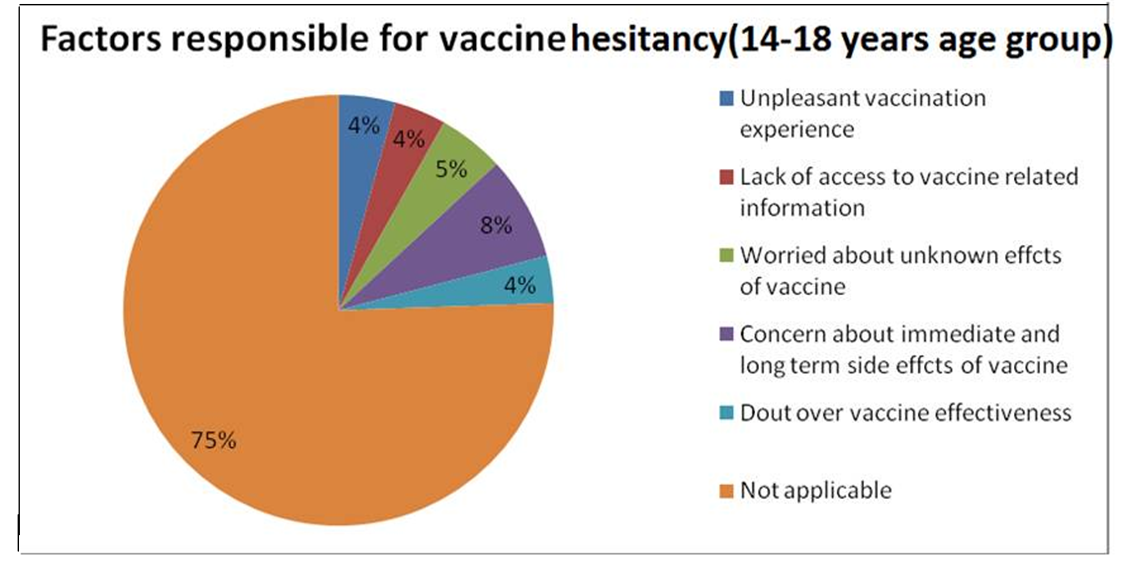
The factors which precipitated vaccine reluctance were unpleasant vaccination experience due to lack of confidence in vaccinators (nurse/technical staff at vaccination centre) and poor management at vaccine centre, 10(4%), lack of access to vaccine related information, 11(4.2%), apprehension about known and unknown immediate and delayed adverse effects post vaccination, 14(5.4%), doubtful vaccine effectiveness, 10(4%) (Figure 5).
Statistical Analysis
Data Analysis was done using IBM-SPSS version 22 Chicago, USA.
Discussion
In India, only CovaxinTM was approved for vaccinating teenagers of more than 14 years till 18 years of age at the time of study proposal submission. CovaxinTM roll out for vaccinating adolescents was done on 10 January 2022 after undergoing through the rigorous, multistage testing process and phase III clinical trials to ensure it’s the safety [10].
There are very limited studies on the AEFI with CovaxinTM on Indian population. We did not find any study on AEFI during literature search, for CovaxinTM among adolescent teenagers (14-18 years of age). The majority of the studies available in search literature were on CovishieldTM (ChAdOx1) and BNT162b2.
In our study, the most common AEFI symptoms after the first and second dose were fever (37% & 19.1%) followed by generalized myalgia (27.1% & 11.1%) and local pain/ swelling at injection site (13% & 7.3%) and respectively. AEFI reported by subjects in our study are 2-3 times higher compared to available studies on CovaxinTM. Houshmand B, et al in their study have shown similar adverse effects as found in our study except for very rare adverse effects in the form of diarrhea, arthralgia, nasal and oral bleeding with CovaxinTM in middle age adults [11]. The difference in response may be related to higher immune response seen in children and adolescents compared to adults and elderly.
In the study by Ella R, et al. (2021) in their phase III trials of CovaxinTM, 12.5% adult participants experienced at least one AEFI. No serious adverse effects were reported by subjects except for Immune thrombocytopenia (1/5959) participants. Overall AEFI were lower following second dose (4.3%) compared to first dose (5.9%) of CovaxinTM. Frequently reported local Adverse effects were local injection site pain, induration and erythema and common systemic adverse effects were headache, myalgia and mild to moderate grade fever. Around 9% subjects reported AEFI within 7 days post vaccination. Only 0.1% and 0.04% subjects reported immediate adverse effects within 30 minutes of vaccination following first and second dose respectively [12].
In contrast to study by Ella R et al, we in our study found that majority of subjects (22.3%) experienced adverse effects up to the duration of 24-48 hours following first and second dose of vaccine, the symptoms resolved after 2nd day post vaccination. Only 4.9% of subjects had AEFI symptoms beyond 72 hours (3 days) post first dose and 2.1% subjects had AEFI symptoms beyond 72 hours (3 days) post second dose of vaccine. In general, the AEFI were mild, self limiting and tolerable in most of the subjects following first in 127 (48.4%) and second dose in 181 (71.7%) respectively. AEFI symptoms were relatively more after first dose compared to second dose of CovaxinTM. This finding was similar to a study conducted by Kaur, et al. (2021) in North India; they have reported 40% and 16.6% of the AEFI among first and second dose beneficiaries, respectively [13, 14].
Study by Zhu F et al on AEFI of adenovirus vaccine, found a 69% overall AEFI incidence within 14 days post vaccination in subjects aging 6-17 years. Also overall AEFI in the vaccine group was significantly higher than that in the placebo group (22%). In contrast to the RNA vaccine, fewer adverse events were reported in the adenovirus vector vaccine group following Dose 2 than after Dose 1. The most common adverse events with adenovirus vaccine were injection-site pain, fever, headache, and fatigue. Most adverse events were not serious and resolved in few days. Incidence of local and systemic adverse events, were higher in the vaccine group than in the placebo group [15].
The reported AEFI in our study was higher than that of the Phase 2 trial of CovaxinTM. Ella et al reported 21% AEFI for BBV152 (CovaxinTM) with 6 µg Algel IMDG and 17% with 3 µg Algel IMDG. However, Kamal, et al. (2021) reported a 57% rate of AEFI among the study participants. The difference may be due to the difference in vaccines [16, 12].
Kaur, et al. (2021) in their study finding, shown majority of the AEFI to be among the younger age groups compared to elderly [13]. In our study 7.3% of participants had pre- existing medical conditions including diabetes, bronchial asthma, hypertension, cutaneous allergies, polycystic ovarian disease, liver and renal stones, thyroid dysfunction and migraine. Also hypersensitivity in the form of allergic rash within one week, were to the extent of 0.8% (2) and 0.4% (1) following first and second dose respectively.
In our study, few participants reported additional AEFI beyond study questionnaire. Self reported adverse effects in our study were positive Covid-19 test within 14 days of vaccination, excess hair fall, altered taste sensation, profound generalised weakness and fatigue. These AEFI symptoms were more following first dose compared to second dose except for hair fall (7.2% after second dose compared to 1.9% after first dose). Hair fall was significant with a p < 0.05 (Figure 2). Few studies have also reported similar adverse effects post vaccination [17, 18].
We did not find any serious adverse events in our study. Kim, et al. (2021) in South Korea reported only one serious AEFI in the form of severe vomiting [19]. In our study, overall 38.2% of the participants had self-medicated with analgesic antipyretic (paracetamol) pre and post vaccination. Our finding was similar to a study by Shrestha, et al. (2021) [20]. In our study we also made an attempt to explore the factors responsible for vaccine hesitancy (Figure 5). Vaccine hesitancy rapidly rose due to growing number of cases who developed vaccine-related severe or permanent adverse events such as myocarditis, hypertension, acute respiratory failure, septic shock, sudden hearing loss, and thrombo- embolic events [21, 22, 23].
Our study present a well-documented safety profile of CovaxinTM, even in co-morbid younger patients (14-18 years of age) may ameliorate the safety concerns associated with vaccine. Vaccination plays an important role in protecting the health of children. In the previous study by MacDonald NE, few determinants of vaccine hesitancy have been categorized as contextual influences (due to historic, political, environmental and health systems), individual and group influences arising due to personal/group perception of subject/subjects and vaccine-/vaccination-specific issues directly related to vaccine contents or vaccination process. We consider that these determinants are largely influenced by disseminating correct information about vaccine, AEFI reporting and causality assessment influences these determinants. Although vaccination should certainly not be made compulsory, it is important that parents make the right decision by allowing children to be vaccinated without hesitation [24].
Strengths and Limitations of Study
To our best of knowledge, present prospective observational study is the first ever study on AEFI of CovaxinTM and vaccine hesitancy among 14-18 years age, in India. Certain notable limitations in our study are probability of selection bias which could have risen due to incorporating subjects reporting more AEFI unintentionally.
Conclusion and Recommendations
Present study has indicated an acceptable safety profile of COVID-19 vaccine (CovaxinTM) approved for 14-18 years of age group in India. The study will encourage children, adolescents and their parents to take vaccine shots to curb resurgence of pandemic. Overall, CovaxinTM is well tolerated and projects a good safety profile in young adolescents even with pre-existing co-morbidities. Since CovaxinTM is a killed (inactivated vaccine), it appears to be relatively safer compared to other available vaccines available in India. Monitoring and assessment of long-term adverse events needs to be done through active surveillance. There is a need to address safety concerns related to vaccine using Television, social media and print media. Adequate and valid explanation and preparation for expected adverse effects (AEs) is essential to promote widespread vaccination coverage.
Acknowledgement
We are thankful to Indian Council of Medical Research (ICMR), Delhi for providing the opportunity to take on this STS-ICMR research project. Our sincere gratitude to our participants, without whom the study could not have been possible.
Financial Support
It is a self-funded research project.
Conflict of Interest
None declared
References
-
Yi-Chi W, Ching-Sung C, Yu-Jiun C (2020) The outbreak of COVID-19: An overview. J Chin Med Assoc 83(3): 217- 220.
-
World Health Organization (2020) COVID-19 vaccines: safety surveillance manual.
-
Kant R, Dwivedi G, Zaman K, Sahay RR, Sapkal G, et al. (2021) Immunogenicity and safety of a heterologous prime-boost COVID-19 vaccine schedule: ChAdOx1 vaccine Covishield followed by BBV152 Covaxin. Journal of Travel Medicine 28(8): 1-4.
-
Ahmed TI, Rishi S, Irshad S, Aggarwal J, Happa K, et al. (2022) Inactivated vaccine Covaxin/BBV152: A systematic review. Front Immunol 13: 863162.
-
Jeon M, Kim J, Oh CE, Lee JY (2021) Adverse Events Following Immunization Associated with Coronavirus Disease 2019 Vaccination Reported in the Mobile Vaccine Adverse Events Reporting System. J Korean Med Sci 36(17): e114.
-
Chandler RE (2020) Optimizing safety surveillance for COVID-19 vaccines. Nat Rev Immunol 20(8): 451-452.
-
Pawar PN, Chavhan SS, Jadhao VF, Adsul BB, Kumbhar MA, et al. (2022) To study the adverse effect following immunization (AEFI) and Covid-19 infection and Covid-19 vaccine benefeciaries. J Assoc Physicians India 70(2): 11-12.
-
Joshi RK, Muralidharan CG, Gulati DS, Mopagar V, Dev JK, et al. (2021) Higher incidence of reported adverse events following immunisation (AEFI) after first dose of COVID-19 vaccine among previously infected health care workers. Med J Armed Forces India 77(Suppl 2): S505-S507.
-
Danabal KGM, Magesh SS, Saravanan S, Gopichandran V (2021) Attitude towards COVID 19 vaccines and vaccine hesitancy in urban and rural communities in Tamil Nadu, India – a community based survey. BMC Health Serv Res 21(1): 994.
-
India Covid-19 Vaccine Tracker (2020) Ministry of Health and Family Welfare Government of India.
-
Houshmand B, Keyhan SO, Fallahi HR, Ramezanzade S, Sadeghi E, et al. (2022) Vaccine-associated complications: a comparative multicenter evaluation among dental practitioners and dental students-which candidate vaccine is more safe in SARS COV II, Gam-COVID-Vac (Sputnik V), ChAdOx1 nCoV-19 (AstraZeneca), BBV152 (Covaxin), or BBIBP-CorV(Sinopharm)?. Maxillofac Plast Reconstr Surg 44(1): 3.
-
Ella R, Reddy S, Jogdand H, Sarangi V, Ganneru B, et al. (2021) Safety and immunogenicity of an inactivated SARS-CoV-2 vaccine, BBV152: interim results from a double- blind, randomized, multicentre, phase 2 trial and 3 month follow up of a double blind, randomized phase 1 trial. Lancet Infecr Dis 21(7): 950-961.
-
Parida SP, Sahu DP, Singh AK, Alekhya G, Subba SH, et al. (2022) Adverse events following immunization of COVID‐19 (Covaxin) vaccine at a tertiary care center of India. Journal of medical virology 94(6): 2453-2459.
-
Kaur U, Ojha B, Pathak BK, Singh A, Giri KR, et al. (2021) A prospective observational safety study on ChAdOx1 nCoV-19 corona virus vaccine (recombinant) use in healthcare workers- first results from India. E Clinical Medicine 38:101038.
-
Zhu F, Jin P, Zhu T, Wang W, Ye H, et al. (2022) Safety and immunogenicity of a recombinant adenovirus type-5- vectored COVID-19 vaccine with a homologous prime boost regimen in healthy participants aged 6 years and above: a randomised, double-blind, placebo controlled phase 2b trial. Clin Infect Dis 75(1): e783-e791.
-
Kamal D, Thakur V, Nath N, Malhotra T, Gupta A, et al. (2021) Adverse events following ChAdOx1 nCoV-19 Vaccine (COVISHIELD) amongst health care workers: A prospective observational study. Medical Journal Armed Forces India 77(2): S283-S288.
-
Scollan ME, Breneman A, Kinariwalla N, Soliman Y, Youssef S, et al. (2022) Alopecia areata after SARS-CoV-2 vaccination. JAAD Case Rep 20: 1-5.
-
Jerome RL Diallo AO, Dachy B, Bon SDL, Maniaci A, et al. (2021) COVID-19: Post-vaccine Smell and Taste Disorders: Report of 6 Cases. Ear, Nose & Throat J 1: 1455613211033125.
-
Kim SH, Wi YM, Yun SY, Ryu JS, Shin JM, et al. (2021) Adverse Events in Healthcare Workers after the First Dose of ChAdOx1 nCoV-19 or BNT162b2 mRNA COVID-19 Vaccination: a Single Center Experience. J Korean Med Sci 36(14): e107.
-
Shrestha S, Devbhandari RP, Shrestha A, Aryal S, Rajbhandari P, et al. (2021) Adverse events following the first dose of ChAdOx1 nCoV-19 (COVISHIELD) vaccine in the first phase of vaccine roll out in Nepal. Journal of Patan Academy of Health Sciences 8(1): 9-17.
-
Kewan T, Flores M, Mushtaq K, Alwakeel M, Burton R, et al. (2021) Characteristics and outcomes of adverse events after COVID-19 vaccination. J Am Coll Emerg Physicians Open 2(5): e12565.
-
King WW, Peterson MR, Matar RM, Budweg JB, Cuervo PL, et al. (2021) Myocarditis following mRNA vaccination against SARS-CoV-2, a case series. Am Heart J Plus 8: 100042.
-
Houghton DE, Wysokinski W, Casanegra AI, Padrnos LJ, Shah S, et al. (2022) Risk of venous thromboembolism after COVID‐19 vaccination. Journal of Thrombosis and Haemostasis 20(7): 1638-1644.
-
Fernandes N, Costa D, Costa D, Keating J, Arantes J (2021) Predicting COVID-19 vaccination intention: the determinants of vaccine hesitancy. Vaccines 9(10): 1161.
- Update on Malariology and Malaria Vaccines
- Addressing Vaccine Hesitancy in the Age of Measles Resurgence: A Mini-Review
- Exploring Barriers and Facilitators of Group Antenatal Care Implementation in Kaduna State, Nigeria: A Qualitative Evaluation
- The Role of IL-11 in Regenerative Medicine and Tissue Engineering
- New Prediction of Mortality rate of Covid -19 According to WHO Estimation
- Measles Vaccine in Kano, Northern Nigeria: Past, Present and Future