Successful Management of Heterotropic Pregnancies with Favorable Outcomes
Introduction: Heterotrophic pregnancy, or coexistence of intrauterine and extra uterine pregnancy, is a rare entity, with a difficult pre-operative diagnosis. The incidence in the general population is estimated to be 1 in 30,000 to 1 in 40,000. Cases: We present two interesting cases of heterotrophic pregnancies with successful outcomes. The illustrated cases did not have any risk factor for the heterotypic gestation and presented in early gestation with abdominal pain. Both the patients were taken up for operative management and we were able to continue the intrauterine pregnancy further to a term delivery. Prompt diagnosis and management could save the intrauterine pregnancies and the ectopic pregnancies were treated timely. Conclusion: The two cases represent heterotypic pregnancy in patients with no risk factors. Quick operative intervention is the mainstay of management.
Case 1
History: A 25 years old female, G3P1L1A1, with previous one normal vaginal delivery, came to the emergency with the complaint of pain abdomen on the right side since two days. She was overdue by eight days and had a positive urine pregnancy test the period of gestation corresponded to 5+4 weeks. She had an ultrasound report showing an intrauterine gestational sac with a yolk sac and a fetal pole and there was no positive adnexal finding noted. The other report showed a thickened endometrial with 2.7x2.7 cm mass on the right adnexa with increased vascularity. There was mild free fluid. On examination the uterus appeared bulky there was some tenderness on the right adnexa. The left adnexa appeared to be normal. There was no bleeding or cervical motion tenderness. Her blood pressure was 110/60 mm Hg and pulse rate was 97/minute. There was no pallor clinically. The past medical and surgical histories were unremarkable. Investigations: Since the reports were conflicting, an emergency USG was done in our institute, which showed an intrauterine gestational sac with no obvious fetal pole and no intrauterine findings. However the endometrial appeared thickened, i.e. 16 mm. Patient was admitted and investigated and kept under close monitoring. Her Beta HCG was 2343 MIU. The other investigations i.e. liver function tests, kidney function tests and hemogram were normal.

Figure 1: TVS showing an adenxal mass with an intrauterine gestational sac. Management: A decision of laparoscopic examination was made on the basis of clinical signs. On laparoscopy, the uterus was enlarged and there was around 200 cc hemoperitonem and left sided mass of around 4x4 cms with clotted blood and products of conception inside .The left tube appeared vascular and edematous, the fibril end was completely embedded in clots and appeared agglutinated. The clots and products were removed and sent for histopathology. There were flimsy adhesions on the right fibril end to the lateral pelvic wall. Right tube was grossly normal. Findings were consistent with tubal abortion.

Figure 2: Hemoperitoneum and products of conception in the Pouch of Douglas as seen in laparoscopic examination. Follow up: Patient discharged in a satisfactory condition after 1 week with a confirmed intrauterine cardiac activity and increasing trend of B Hcg. Histopathology of adnexal tissue showed products of conception. Patient continued the pregnancy till term and went into spontaneous labor and delivered a female baby of 3.08kg at 39 weeks of gestation.
| 40,000 [1]. | The risk of HP following in vitro fertilization | ||
|---|---|---|---|
| (IVF) has been estimated as high as 1:100 women [2,3]. | |||
| Risk factors for ectopic pregnancy | are tubal or pelvic | ||
| diseases, prior pelvic surgeries and multiple ovulations or | |||
| multiple Embryo Transfers. | If diagnosed timely, it can be |
Case 2
History
A 27 years old primigravida came to the casualty with amenorrhea of six weeks and with the complaint of pain in abdomen since four days. It was a spontaneous conception. There were episodes of spotting P/V off and on but no active bleeding and noepisode of fainting. She had consulted a private doctor and got an ultrasound done. There was no past history of infertility, tuberculosis and past surgeries. Patient was hemodynamically stable at the time of presentation. Vaginal examination revealed a bulky uterus and right sided fornicial tenderness. Investigations Her hemoglobin was 9.7mg/dl and other parameters in the complete blood count were normal. Liver funvction tests, renal function tests and coagulation profile were normal. Her betaHcg was 2380MIU/ML and the ultrasound scan findings were suggestive of a thickened endometrium and an right adnexal mass of 3x3 cms with a gestational sac and a yolk sac with increased vascularity and moderate free fluid in pouch of Douglas.

Figure 3: Intrauterine gestational sac and mild free fluid in the pelvis. Management: Patient was taken up for an emergency laprotomy and a note of left sided tubal abortion was made with a gravid uterus. The right tube and ovary werenormal. Hemoperitonem of around 200 cc was present along with some old clots. The left tube was densely adherent to the bowel. Left salpingectomy was done after minimal adhesiolysis. Patient remained stable in the post operative period.
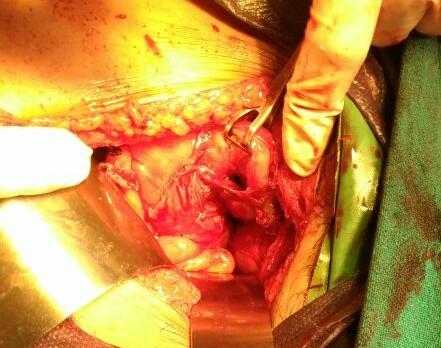
Figure 4: Right tubal abortion and adhesions of the right tube (held with Babcock’s forceps) to bowel. Follow up: Patient was kept under observation for five days. She was discharged with a positive cardiac activity and an increasing trend of B Hcg. She was kept on progesterone support till 32 weeks as a precautionary measure. Pregnancy remained uneventful and she had a normal vaginal delivery of a 2.7 kg healthy male baby.
Discussion
The incidence of heterotopic pregnancy (HP) has been reported varying from 1:4000 to 1:30,000 women in the general population [2, 3]. The risk of HP following in vitro fertilization (IVF) has been estimated as high as 1:100 women, though both the patients reported here had spontaneous conception [1, 2, 3]. The hydrostatic forces generated during embryo transfer may contribute to the increased risk [4]. The risk factors for HP are past tubal or pelvic diseases, surgeries and multiple ovulations or multiple ET.
In a study by Tal et al it was reported that 70% of the heterotopic pregnancies were diagnosed between 5 to 8 weeks of gestation, 20% between 9 to 10 weeks and only 10% after 11 weeks of gestation [5]. The most common site of ectopic gestation in a heterotopic pregnancy is the fallopian tube. However, there are reports of cervical and ovarian heterotopic pregnancies also [6, 7].
Around 50% of heterotopic pregnancies do not have any symptoms [8]. It poses a big diagnostic dilemma. The common presenting signs and symptoms are abdominal pain, adnexal mass, peritoneal irritation and an enlarged uterus [9]. It should be considered in cases when a patient has undergone assisted reproduction technique, with persistent or rising chorionic gonadotropin levels after dilatation and curettage for an induced/spontaneous abortion, when the uterine fundus is larger than for menstrual date, when more than one corpus luteum is present in a natural conception and when vaginal bleeding is absent in the presence of signs and symptoms of ectopic gestation [10].
The differential diagnosis is corpus gluteal hematoma, ectopic pregnancy and other surgical causes coexisting with pregnancy. Corpus gluteal cyst can mimic an extra- uterine pregnancy. Both the pathologies can present as acute pain and tenderness. However, a corpus luteumcyst, includes decreased wall echogenicity compared with the endometrial and is anechoic. Also, a corpus luteum moves with the ovary on bimanual sonographic exam, while an extra-uterine pregnancy moves separately from the ovary, ultrasonography can be used to differentiate the two conditions. Sometimes heterotopic pregnancy mimics a ruptured ovarian cyst. The signs of a developing trophoblast on ultrasonography are seen as a high velocity, low resistance Doppler signal. If this type off lowpattern is seen in an adnexal mass usingtrans abdominal ultrasound the sensitivity for thediagnosisofanectopicpregnancygoesupto 73% from 53%.
The recent advances in transvaginal sonography (TVS) helped in the early diagnosis of heterotropic pregnancy. However, the sensitivity of TVS in diagnosing heterotropic pregnancy is only 56% at 5–6 weeks [11]. In TVS, the typical image of a heterotopic pregnancy is the presence of an IU gestation coexisting with an ectopic cornual pregnancy containing an embryo. High resolution transvaginal ultrasound with color Doppler will be helpful as the trophoblastic tissue in the adnexa in a case of heterotopic pregnancy shows increased flow with significantly reduced resistance index [12]. The most common extra-uterine images in transvaginal 2D ultrasound in heterotopic pregnancies consist of complex cysts or adnexal masses, which may comprise hematosalpinx, tubal ring, or even a live embryo, with or without accompanying free fluid in the peritoneal cavity [13]. However, 2D ultrasound may often be indeterminate, and in such cases, MRI of the pelvis may be used to assist in the diagnosis [14].
Surgery continues to be the mainstay of management for heterotopic pregnancy, with laparotomy being the preferred technique. The majority of cases (58.9% to 73.8%) are diagnosed at the time of surgical exploration [5]. The treatment of a heterotopic pregnancy is laparoscopy/laparotomy for the tubal pregnancy [10].
| References |
1. Barnhart K. (2009) Ectopic pregnancy. N Engl J Med
361: 379-387.
2. Barrenetxea G, Barinaga Rementeria L, Lopez de Larruzea A, Agirregoikoa JA, Mandiola M, et al. (2007) Heterotopic pregnancy: two cases and a comparative review. Fertil Steril 87(2): 417. e9-15.
3. Clayton HB, Schieve LA, Peterson HB, Jamieson DJ,
Reynolds MA, et al. (2006) Ectopic pregnancy risk with assisted reproductive technology procedures. Obset Gynecol 107(3): 595-604.
| Lyons EA, Levi CS, Sidney M (1998) In: | Rumak CM, et | |
|---|---|---|
| al. (Eds), | 2nd | |
| (Edn.), 2, Mosby, pp: 999. |
5. Tal J, Haddad S, Gordon N, Timor Tritsch I (1996)
Heterotopic pregnancy after ovulation induction and assisted reproductive technologies: a literature review from 1971 to 1993. Fertil Steril 66(1): 1-12.
6. Hirose M, Nomura T, Wakuda K, Ishguro T, Yoshida Y
(1994) Combined intrauterine and ovarian pregnancy: A case report. Asia Ocaena J ObstetGynaecol 20(1): 25-29.
7. Peleg D, Bar Hava I, Neaman-Leavin M, Ashkena, Ben
Rafaelz IJ (1994) Early diagnosis and successful non surgical treatment of viable combined intrauterine and cervical pregnancy. Fertil Steril 62(2): 405-408.
8. Louis Sylvestre C, Morice P, Chapron C, Dubuisson JB
(1997) The role of laparoscopy in the diagnosis and management of heterotopic pregnancies, Human Reproduction 12 (5): 1100-1102.
9. Reece EA, Petrie RH, Sirmans MF, Finster M, Todd WD
(1983) Combined intrauterine and extrauterine gestations: a review. Am J Obstet Gynecol 146(3): 323-330.
| Obstetrics. | 21st (Edn.), Multifocal Ectopic Pregnancy | |
|---|---|---|
| in Chapter 34, pp: 888-889. |
11. Dündar O, Tütüncü L, Müngen E, Muhcu M, Yergök YZ
(2006) Heterotopic pregnancy: Tubal ectopic pregnancy and monochorionic monoamniotic twin pregnancy: A case report. Perinat J 14: 96-100.
12. Glassner MJ, Aron E, Eskin BA (1990) Ovulation
induction with clomiphene and the rise in heterotopic pregnancies: A report of two cases. J Reprod Med 35(2): 175-178.
13. Elito Junior J, Montenegro NA, Soares Rda C, Camano
L (2008) Unruptured ectopic pregnancy—diagnosis and treatment. State of art. Rev Bras Ginecol Obstet 30(3): 149-159.
14. Tamai K, Koyama T, Togashi K (2007) MR features of ectopic pregnancy. Eur Radiol 17(12): 3236-3246.
15. Cohen J, Mayaux MJ, Guihard Moscato MI, Schwartz D
(1986) In vitro fertilization and embryo transfer: a collaborative study of 1163 pregnancies to the incidence and risk factors of ectopics pregnancies. Hum Reprod 1(4): 255-258.
- The Need for Partner Education and Mental Health Support During Pregnancy and the Postpartum Period
- Application of Combined PGT-A and PGT-M for Reproductive Management in a Couple Carrying GCDH Mutations with Prior Affected Offspring: A Rare Case Report
- The Effect of Using a New Technique Karman Injector (Elif Technique) on the Healing Process of Wound Infection-Case Series
- GSM: Counseling Points to Discuss with Women Fearful of Vaginal Estrogen
- Antenatal Diagnosis of Meckel Syndrome: A Case Report
- Discrimination and Workplace Harassment (Mobbing) against Women in the Post-Pandemic Era