Carcinoma of Vagina in Women with Utero Vaginal Prolapse: Presentation of Two Cases and the Review of Literature
Primary vaginal cancer in women with utero vaginal prolapse is an uncommon entity. We report two women with longstanding third degree prolapse presented with ulcerated lesions. Both had vaginal hysterectomy and anterior colporrhaphy. Histology revealed moderately differentiated squamous cell carcinoma. One woman developed advanced malignancy in three months of surgery and the other is surviving after five years. The latter developed a lesion in the vagina recently and biopsy revealed poorly differentiated squamous cell carcinoma. Review of the literature and personal experience suggest that vaginal hysterectomy and repair should be offered to women developing utero vaginal prolapse as when longstanding chances of developing cancer of vagina becomes significant.
Introduction
Primary carcinoma of vagina is a rare disease. The disease is uncommon in women with utero vaginal prolapse. Women with prolapse developing this condition are in their old age and the problem caused by the carcinoma should not be underestimated.
This paper elaborates the occurrence of squamous cell carcinoma of vagina on two women with longstanding utero vaginal prolapse presented at the Teaching Hospital, Batticaloa, Sri Lanka. One woman had died of the cancer within few months of initial surgery and the other had survived about five years and is still living.The literature cited for this case report are taken from recent studies and these studies covered wide range of literature in this field.
Case 1: Mrs. J N 58 years old post menopausal woman presented in the year 2008 with utero vaginal prolapse of six years duration. An ulcer had developed for three months with foul smelling discharge at times blood stained. She also complained dysuria. She also had a history of hypertension of three years duration which was under control with treatment. Examination showed an otherwise healthy obese woman. Genital examination revealed a third degree prolapse with a discharging ulcer about 50mm diameter on the anterior vaginal wall towards the left. The ulcer had a hard surface with adjacent induration. Discharge was evident. Uterine cervix appeared healthy.
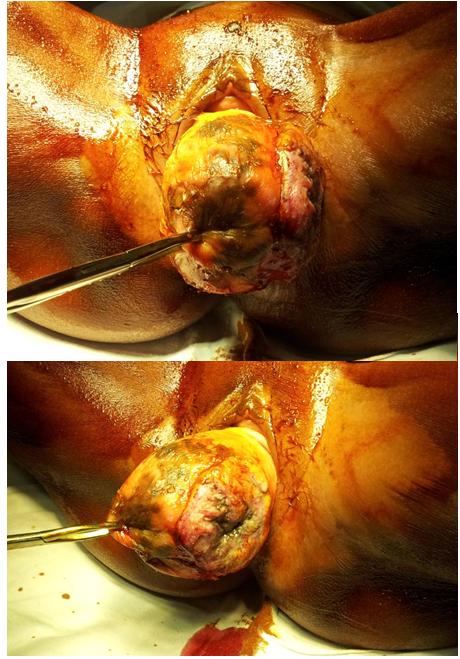
Vaginal hysterectomy and anterior colporrhaphy was performed on her. Difficulties encountered to have an adequately clear margin of the ulcer on the left lateral wall of the vagina. Post operative recovery was uneventful. Histology revealed squamous cell carcinoma of vagina. She defaulted adjuvant therapy. Three months later she got admitted to the ward with severe whitish discharge, urinary incontinence, and miserably emaciated. The cancer appeared widespread and succumbed to the illness. Case 2: Mrs. P K 67 yearsold post menopausal woman presentedin June 2013 with Lump at vulva for 40 years’ duration. She also developed retention of urine for one week and blood stained vaginal discharge for one month. Examination revealed an average built woman, mildly pallor and had third degree utero vaginal prolapse with an indurating ulcer on the anterior vaginal wall. The ulcer was of 45mm maximum diameter near the uterine cervix with everted margins. Cervix was clinically uninvolved (Figure 1).
Initially upon admission a biopsy was taken from the ulcer to exclude malignancy and histology revealed as “Pseudo epitheliomatous hyperplasia”. However vaginal hysterectomy and anterior colporrhaphy was performed owing to the indurated ulcer with malignant features. Post-surgical recovery was uneventful.Histology revealed a well differentiated ulcerated squamous cell carcinoma of vagina infiltrating into 12mm thickness, 15mm away from closest resection margin.She had been followed up closely. She did not have any significant features of malignancy, except the complaint of abdominal discomfort.
She presented in June 2018 at her age of 72 years with Blood stained vaginal discharge and back ache. Examination revealed a lesion 3 cm size, appearing as ulcer, tender with indurations, at the inside the introitus on left side. Biopsy of the growth revealed moderately differentiated squamous cell carcinoma. She is referred to Oncologist for further care (Figure 2).

Discussion
Primary vaginal cancer is a rare disease [1], about 1 - 2% of the female genital tract [2]. About 80% of the vaginal cancers are metastatic, primarily from the cervix or endometrium. Women previously undergone hysterectomy are also at risk of developing primary vaginal cancer [3, 4]. Commonest Risk factor for Carcinomas of vagina is Human Papilloma virus infection (HPV) [4, 5, 6]. Multiple pregnancies, having first child at a young age (before 17 years), vaginal irritation, poor genital hygiene, genital warts, in situ or invasive cervical cancer treated previously have also been the risk factors[2, 4, 5, 6]. Vaginal irritation caused by uterine prolapse and using a pessary are also known to increase the risk of cancer [2, 5].
About 80% of the cases presented with carcinoma of vagina are squamous cell carcinoma [2, 4, 7, 8, 9, 10, 11, 12] at the age between 60 – 80 years. The Lesion is usually exophytic with papillary configuration. Ulcerative and infiltrating as well as flat superficially spreading forms are also seen. The full extent of the tumour and its relationship to cervix urethra, hymenal ring or vulva must be appreciated for treatment planning [3]. The ulcer is presented with hard base and raised edges which leads to bleeding and discharge [2]. This is specially seen in the cases with utero vaginal prolapsed [7].
In our study both women had developed longstanding utero vaginal prolapse; one woman for an incredible forty years duration. Both had developed ulcers which appear to be the feature in prolapsed vagina. Carcinoma of vagina with utero vaginal prolapse is rare and a very uncommon condition [8, 10, 11, 12].
Women with longstanding utero vaginal prolapse are of old age and seek health care mostly when they develop symptoms significant enough to cause much discomfort to them. Poor ability in maintaining a good hygiene of the prolapsed organ, poor nutritional status in old age too would contribute to this status. Therefore, although rare, chances of developing malignant lesion in the prolapsed vagina are of significance and it was reported that 13,6% to 16.3% of total vaginal cancer coexist with prolapsed [9].
Radiotherapy is the recommended therapy for squamous cell carcinoma of vagina and surgery has a limited role [2, 3, 12]. However, surgery is the suggested choice in the cases with utero vaginal prolapse [7, 11] with satisfactory outcomes.
In our study, both women had vaginal hysterectomy with anterior colporrhaphy. This type of surgery becomes necessary owing to the prolapsed nature of the uterus and vagina. Clinical evaluation showed that the ulcer base was palpably not deep and urinary bladder was free without induration. In our first case (Mrs. JN) the ulcer extended in the anterior vaginal wall without adequate margin on the left side for resection. Nevertheless, after surgery the wound healed well and she was strongly advised to seek oncology care. Despite such strong advice she defaulted and succumbed to the illness within a few months of surgery. This would be a disadvantage as surgery brought an immediate cure and would be the reason for her default. The second case (Mrs. PK) however had surgical resection of the ulcer, minimum of 15 mm from the closest resection margin with infiltration of 12 mm indicating an early lesion with complete resection. She had been having regular health visits and had been free from developing the illness until recently. These would be the reasons for her survival for five years. The 5-year disease specific survival is reported to be 84% for stage I, 75% for stage II vaginal cancers [12]. Developing a malignant lesion in five years could be a fresh illness.
In conclusion although rare, impact of vaginal cancer in women’s health should not be under estimated. This is specially so to women with utero vaginal prolapse who had a higher tendency in developing squamous cell carcinoma of vagina. Almost all reported cases have the longstanding prolapse indicates that specially the post menopausal women when presents with utero vaginal prolapse they be offered vaginal hysterectomy and repair and if pessary is preferred vaginal cytology too should be performed on regular basis since the precursor lesion VAIN could be detected.
Conflict of Interest
None
References
-
Beller U, Benedet JL, Creasman WT, Ngan HYS, Quinn MA, et al. (2006) Carcinoma of the Vagina. Int J Gynaecol Obstet 95 Suppl 1:S29-S42.
-
Tumours of the vagina (2014) In: Malhotra N, et al. (Eds.), Jeffcoat’s Principles of Gynaecology, 8th(Edn.), pp: 426.
-
Tumours of Vagina (1993) In: Morrow CP, et al. (Eds), Synopsis of Gynecologic Oncology. Churchill Livingstone, pp: 93-97.
-
Sueblinvong T, Carney ME (2009) Vaginal Cancer. In: Paola Gehrig, et al. (Eds.), Gynecologic Oncology, Landes Bioscience, pp: 197.
-
Bardawil T (2015) Vaginal Cancer.
-
Cancer of vagina (2011) In: Dizon DS, et al. (Eds), Gynecologic Cancer, Jones and Bartlett, pp: 117.
-
Ghosh SB, Tripathi R, Mala YM, Khurana N (2009) Primary invasive carcinoma of vagina with third degree uterovaginal prolapse: a case report and review of literature. Arch Gynecol Obstet 279(1): 91- 93.
-
Kim HG, Song YJ, Na YJ, Choi OH (2013) A Case of Vaginal Cancer with Uterine Prolapse. J Menopausal Med 19(3): 130-142.
-
Fedus T, Raś R, Książek M, Filipowska J, Kaznowska E, et al. (2017) Primary vaginal squamous cell carcinoma with bladder involvement in uterine prolapsed patient: Case report. Medicine (Baltimore) 96 (50): e8993.
-
Acharya S, Uprety DK (2012) Carcinoma of vagina in utero-vaginal prolapse: a rare presentation. JNMA J Nepal Med Assoc 52(186): 82-84.
-
Wang Y, Li Q, Du H, Lv S, Liu H (2014) Uterine prolapse complicated by vaginal cancer: a case report and literature review. GynecolObstet Invest 77(2): 141-144.
-
Shrivastava SB, Agrawal G, Mittal M, Mishra P (2015) Management of Vaginal Cancer. Rev Recent Clin Trial 10(4): 289-297.
- The Need for Partner Education and Mental Health Support During Pregnancy and the Postpartum Period
- Application of Combined PGT-A and PGT-M for Reproductive Management in a Couple Carrying GCDH Mutations with Prior Affected Offspring: A Rare Case Report
- The Effect of Using a New Technique Karman Injector (Elif Technique) on the Healing Process of Wound Infection-Case Series
- GSM: Counseling Points to Discuss with Women Fearful of Vaginal Estrogen
- Antenatal Diagnosis of Meckel Syndrome: A Case Report
- Discrimination and Workplace Harassment (Mobbing) against Women in the Post-Pandemic Era