Triple-Negative Breast Cancer: A Rare Tumor Type Presenting in Pregnancy-Case Report
Introduction: Breast Cancer diagnosis during pregnancy is a relatively rare event, affecting about 1 in 1,000 pregnancies and representing 0.1% or less of all cancers. However, when it occurs, it is found to be more aggressive with the worst prognosis during pregnancy. Most notable reasons include delayed diagnosis due to changes in breast parenchyma in pregnant and lactating women, and the higher incidence of the poor prognostic subtype (triple-negative) among premenopausal patients. Aim: We present a 28year old nullipara with triple-negative right breast cancer in the third trimester of pregnancy. Methodology: Description of a successfully managed breast cancer disease in pregnancy and the histological diagnosis.
Case Report
Mrs. JS presented with a painless lump progressing in size, located at the upper outer area of her right breast covered with normal skin with no nipple discharge. Her pregnancy was in the third trimester. The clinical triple assessment revealed a hard-irregular 4x6cm lump in the upper outer quadrant with no axillary nodes with no evidence of metastasis. The contralateral breast was normal Immunohistochemistry revealed a triple negative invasive ductal carcinoma. The breast MDT team counselled and administered 3 courses of neoadjuvant chemotherapy after delivery followed by Mastectomy with axillary dissection. The postoperative period was uneventful and the patient had a good clinical response and is currently on follow-up, awaiting radiotherapy.
Background
Breast cancer is the commonest malignancy affecting women, with a lifetime risk of 1 in 8 [1]. Breast cancer is also a global health problem, with more than 1 million cases of breast cancer diagnosed worldwide each year [2]. It also remains the leading cause of cancer-related deaths, most resulting from metastatic disease [3]. Cancer diagnosis during pregnancy is relatively rare, affecting about 1 in 1,000 pregnancies and representing 0.1% or less of all cancers [2, 3]. However, when it occurs, it is found to be more aggressive with a worse prognosis than when it happens outside pregnancy [4, 5]. Various reasons have been given, but two of particular note include delayed diagnosis due to physical changes in the breast of pregnant and lactating women, including hormonal changes during or shortly after pregnancy [4, 5] and a higher incidence of a particularly poor prognostic subtype called triple-negative breast cancer which is common among premenopausal patients [4, 5]. These triple-negative tumours have other characteristics, diagnosis at an advanced stage with a high rate of lymph node metastasis and a large tumour size, including harbouring a subtype of tumours called basal-like cancers, which may harbour carriers of BRCA1 mutation.
Breast cancers are classified into four biological subtypes [5, 6], luminal A (ER + and/or PR+, HER2-), luminal B (ER + and/or PR+, HER2+), HER2-enriched (HER2+, ER-, PR-) and TN or triple negative (negative for all three markers [5, 6]), the type discovered in our patient. Severe financial constraints in a resource-poor environment make testing for these receptors difficult, and treatment is also a challenge, especially in patients who are not economically empowered. We may note that in this environment, late presentation is the norm. Breast cancer and pregnancy are two opposed but progressive conditions in that the fear of death1 eclipses the joy of a new life. The overall incidence of triple-negative
breast cancer is 10-17% [1, 5]. We present a 28year old primigravida with invasive ductal triple negative right breast cancer in the third trimester of pregnancy. Our aim is the description of successful management of triple-negative invasive ductal cancer in a primigravida in a low-resource center where modern treatment facilities are absent.
Mrs. JS presented to our surgical outpatient department in the third trimester with a six-month history of a right breast lump initially about the size of her right thumb but increased over the six months to occupy the upper outer aspect with no similar swellings in the axilla. The skin over the lump was intact, and the lump was not fixed to the underlying structures. Triple assessment, including clinical, radiological, and pathological, showed a hard-irregular lump in the upper outer quadrant, no axillary nodes, multifocal multicentre, and no abdominal or chest metastatic tumour, which turned out to be an invasive ductal cancer with triple- negative biology. A multidisciplinary team made available the treatment options, and the patient made an informed choice to keep the pregnancy and to have neoadjuvant chemotherapy after delivery. Surgery was done after three cycles with a good response, and Hormonal and targeted therapy was not given.
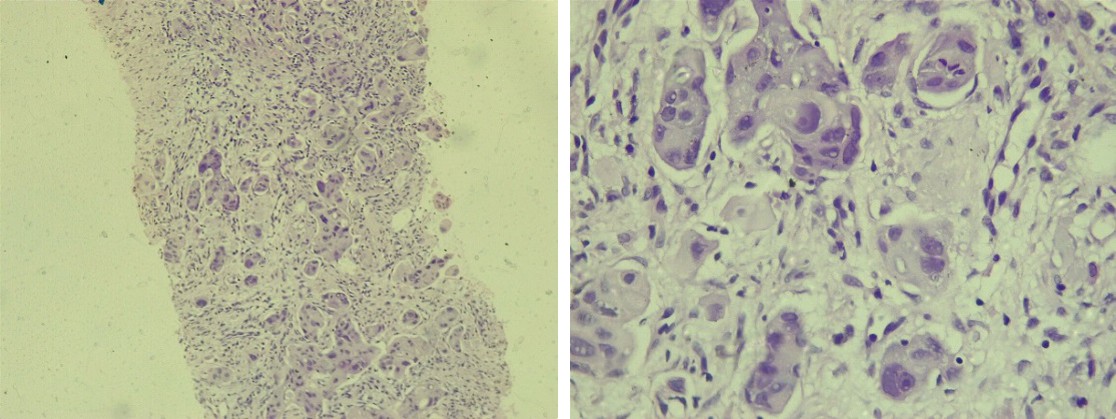
Figure A,B: Show an infiltrative tumour disposed in nests and cords showing malignant ductal cells. A x100, Bx 400.
Discussion
Breast cancer is a challenge in many resource-poor countries [1, 5]. Surgery is the mainstay of management; however, this is hampered by late presentation [1, 3, 5]. Pregnancy-associated breast cancer is diagnosed during pregnancy or within two years after pregnancy [1, 2, 3, 4, 5]. Breast changes in pregnancy further make diagnosis difficult [1, 3, 5]. The factors determining the treatment modality of breast cancer in pregnancy include, among others, trimester of pregnancy, tumour stage, histology, grade, and tumour biology or receptor status [1, 2, 3, 4, 5].
Delay in referring this patient to our centre resulted from the diagnostic difficulty associated with the physiologic changes in pregnancy [1, 3, 4, 5, 6, 7, 8]. Histological specimens were obtained through core cut needle biopsy while ultrasound and chest X-ray were used to stage the patient [9]. The patient had a multidisciplinary team review and still chose to wait until after delivery before chemotherapy despite its safety in the third trimester [10, 11]. She had three cycles before surgery and three cycles after surgery. In the first trimester, organogenesis is in progress; therefore, chemotherapy and radiotherapy greatly risk the fetus [1, 2, 3, 4, 5]. Chemotherapy may be done in the second trimester. In contrast, in the third trimester, it will need to be suspended at least three weeks before surgery to avoid the complications of platelet abnormality and leukopenia from bone marrow suppression. The patient is currently awaiting radiotherapy. If facilities were available, the patient might benefit from screening for BRCA, risk assessment, and counselling for siblings. Further useful tests may include analysis for Basal-like cancer cells.
Conclusion
Breast cancer in pregnancy is rare, and triple-negative breast cancers are also rare. Thorough history and examination with an index of suspicion are required to avoid diagnosis delay. Treatment should be individualized taking into consideration the trimester of pregnancy, stage of disease, histology, tumor biology including receptor status, and available facilities
References
-
Gianfranco M, Dennis R (2020) A case of Triple Negative Breast Cancer diagnosed-case study. JNDS 1(3): 1-5.
-
Hideo S, Shinji O, Daisuke Y, Taizo H (2017) A case report of locally advanced triple negative breast cancer showing pathological complete response to weekly paclitaxel with bevacizumab treatment following disease progression during anthracycline-based neoadjuvant chemotherapy. Int J Surg Case Rep 39: 293-296.
-
Kelly KH, Marjorie CG, Thomas AB (2019) Sabistons`s textbook of surgery Disease of the breast In: Townsend CM, et al. 19th (Edn.), Elsevier, Philadelphia pp: 824-869.
-
Lefrere H, Lenaerts L, Borges VF, Schedin P, Patrick N, et al. (2021) Postpartum breast cancer: mechanisms underlying its worse prognosis, treatment implications, and fertility preservation. Int J Gynecol Cancer 31: 412- 422.
-
Rambau P, Nestory M, Kahima J, Philipo C, Patrizia S, et al. (2014) Triple negative breast cancer in a poor resource setting in North-Western Tanzania: a preliminary study of 52 patients. BMC Research Notes 7: 399.
-
Harri S, Johan L, Mikael L, Tiina L, Ari R, et al. (2011) Breast cancer biological subtypes and protein expression predict for the preferential distant metastasis sites: a nationwide cohort study. Breast Cancer Res 13(5): R87.
-
Virginia FB, Traci RL, Doris G, Pepper S (2020) Postpartum Involution and Cancer: An Opportunity for Targeted Breast Cancer Prevention and Treatments? Cancer Res 80(9): 1790-1798.
-
Krishna I, Lindsay M (2013) Breast cancer in pregnancy. Obstetrics & Gynecology Clinics of North America 40(3): 559-571.
-
Amant F, Loibl S, Neven P, Calsteren KV (2012) Breast cancer in pregnancy. The Lancet 379(9815): 570-579.
-
Amant F, Calsteren KV, Halaska MJ, Gziri MM, Hui W, et al. (2012) Longterm cognitive and cardiac outcomes after prenatal exposure to chemotherapy in children aged 18 months or older: an observational study. The Lancet Oncology 13(3): 256-264.
-
Loibl S, Han SN, Minckwitz GV, Bontenbal M, Ring A, et al. (2012) Treatment of breast cancer during pregnancy: an observational study. The Lancet Oncology 13(9): 887- 896.
- The Need for Partner Education and Mental Health Support During Pregnancy and the Postpartum Period
- Application of Combined PGT-A and PGT-M for Reproductive Management in a Couple Carrying GCDH Mutations with Prior Affected Offspring: A Rare Case Report
- The Effect of Using a New Technique Karman Injector (Elif Technique) on the Healing Process of Wound Infection-Case Series
- GSM: Counseling Points to Discuss with Women Fearful of Vaginal Estrogen
- Antenatal Diagnosis of Meckel Syndrome: A Case Report
- Discrimination and Workplace Harassment (Mobbing) against Women in the Post-Pandemic Era