Recurrent Miscarriage
Recurrent failure, the heartbreaking knowledge of couples who find it difficult to start or extend their families, is a baffling and excitedly distressing generative strength issue. Defined as the incidence of three or more successive pregnancy misfortunes before the 20th temporal length of the event or entity’s existence of a process of early development, recurrent failure influences about 1-2% of couples in general. This abstract delves into the causes, diagnostic approaches, and administrative policies for repeating miscarriages. The study of repeated failure in animals is multifactorial, encompassing hereditary, fundamental, endocrine, immunologic, and tangible factors. Key demonstrative forms include karyotyping, Hysterosalpingography, and hormonal evaluation. Management designs depend on the fundamental causes and accompanying interference’s, ranging from behavioral modifications and pharmacological situations to surgical interference’s. Psychological support is an essential component of caring for the sentimental toll that repeated failure takes on couples. Recent advances in research have cleared potential attacks to a degree of preconception through historical experiments and immunomodulatory remedies. Furthermore, continuous studies are examining the role of behavioral determinants, including diet and stress, in repeated failures.
Introduction
Recurrent failure (RM), the established definition of which is three or more consecutive miscarriages, is relatively exceptional, moving about 1-2% of couples the one created. Three ropes of evidence support the contention that RM is a different clinical body that occurs absolutely by chance. First, the noticed occurrence of RM is significantly above that wanted by accident alone (0.4%); second, a woman’s risk of mis- delivery of freight is straightforwardly connected with the consequence of her prior pregnancies [1]; and tertiary, in contrast to scattered mis-delivery of freight, wives accompanying RM likely to avoid pregnancies with a rational deoxyribonucleic acid complement, suggesting the presence of a continuous fundamental cause for gestation misfortune among women [2, 3].
Despite significant advances in our understanding of the etiology of RM over the last 20 years, even after a comprehensive review, no cause of gestational defeat has been identified in approximately 50% of couples. This has influenced the position where daughters accompanying RM have happened and continue to be, assigning examinations and situations established informal evidence, factual beliefs, and the personal prejudices of their clinicians [4]. This stage aims to determine an inclusive, evidence-located approach to the study and situation of RM while at the same time emphasizing new avenues of research Aetiology Genetic.
Parental Chromosome Abnormalities
In support of common Geisma banding methods, a parental fundamental deoxyribonucleic acid irregularity was identified in between 3 and 5% of couples accompanying RM. A coarser abnormality is an equalized or alternate translocation. While aircraft carriers of an equalized exchange fluctuation are phenotypically normal, bizarre separation at a person’s friend leads to the middle between 50 and 70% of their gametes, and therefore, embryos are unbalanced. Twice as many women are distinguished, and accompanying men are identified as having a structural deoxyribonucleic acid abnormality. This is seemingly due to fundamental irregularities among men guided by sterility. While translocations have occurred for all chromosomes in a variety of combinations, dispassionate failure rates and subsequent gestation consequences for various abnormalities have been reported.
- Male and female parental blood karyotypes
- Lupus anti-coagulant
- IgG and IgM anticardilipin antibodies
- Factor II genotype
- Factor V genotype
- Activated protein C resistance
- Pelvic ultrasound to determine ovarian morphology and uterine anatomy
- Early follicular phase PSH
- Insulin resistance status
Table 1: Contemporary investigative screen for recurrent
Currently, little-lived treatment may be presented to those accompanying a parental karyotype anomaly, apart from referral to an ancestral jurisprudent for conversant advice concerning the forecast of a future pregnancy. This transformation was accompanied by the inauguration of in vitro procreation (IVF) and pre-opinion genetic disease (PGD), at which point fluorescence in seated position hybridization (FISH) was used to determine the historical status of a fetus from a distinct container biopsied three days after implantation. However, before journeying this treatment path, it endures sports that the live birth rate/ phase for those accompanying a reciprocal fluctuation sustaining PGD is lower than anticipated – betwixt 29%/ oocyte retrieval climbing to 38%/fetus transfer [5]. This has to be distinguished to the live beginning rate between those with an exchanged translocation the one persevere accompanying impulsive beginning where the chance of a profitable pregnancy, even after three miscarriages, is betwixt 50 and 65% [6] (Table 1).
Fetal Aneuploidy
Aneuploidy (trisomy or monosomy) is the most commonly identified deoxyribonucleic acid anomaly in individuals, and fetal aneuploidy is the most prevalent cause of failure. Approximately 30% of all miscarriages are trisomic, and a further 10% are due to either sex deoxyribonucleic acid monosomy or polyploidy.
The occurrence of pre-birth trisomy increases with increasing age of the parent, whereas sexuality- deoxyribonucleic acid monosomy and polyploidy do not. The theory of restricted oocyte pool, in which the effect of adulthood is due to a relative shortage of oocytes at optimum stages of development, has existed for a long time [7]. In support of this hypothesis, daughters who have extinct, not completely individual, trisomic embryos have been reported to have a belittled ovarian reserve and record midlife depression at a former age, as distinguished from those with no specific history [8].
Few girls with accompanying RM may be more dependent on hetero-trisomy (the frequency of various trisomies after a trisomic pregnancy). Rubio, et al. [9], utilizing FISH to screen the embryos of couples accompanying RM seeing IVF, reported a significantly higher incidence of abnormal embryos (70%) in an age-doubled control group with no record of RM.
Endocrinopathies
As expected, many RM cases occur secondary to fundamental endocrine defects. However, the following aforementioned defect has convinced evasive Interest has traditionally centered on the idea of defi- client discharge of progesterone for one oeuvre luteum lead- an insult to early miscarriage. This has evolved to be dubbed the luteal point defect, which has been reported to be between 23 and 60% in girls with RM. The diagnosis of a luteal chapter defect is an established luteal state that supports progesterone levels and endometrial biopsies in nonproductive cycles. This is doubtful, as skilled is a depressed agreement middle from two points of endocrine and histological variables in consecutive cycles. Moreover, pre-abstract birth control methods that support files are comparable between successful pregnancies and those that fail [10].
Historically, pro gestational powers existed secondhand from the early beginning in an attempt to prevent miscarriage. This practice is not based on the results of two reasons for the use of progesterone to overcome the failure rate among women with infrequent failure [11, 12]. It endures being eminent; however, a subgroup analysis between mothers with unexplained first trimester RM desires that progesterone use in the first trimester concedes the possibility of benefit.
Well-regulated diabetes is not a risk factor for RM. While the predominance of thyroid autoantibodies is raised among girls with accompanying RM, the anticipated live birth rate among girls with RM who have thyroid antibodies is similar to that of those who do not have these antibodies [13]. Of interest is the relationship between polycystic spasm ovaries (PCO), miscellaneous endocrinopathies that guide polycystic ovarian conditions (PCOS), and RM. The prevalence of PCO, utilizing settled ultrasound tests, was significantly higher among women with RM (40%) and those with an easy reproduction history. Hypersecretion of the luteinizing birth control method (LH) is a new pregnancy misfortune involving mothers undergoing helped ideas and those conceiving instinctively. This is no longer understood to be the case. An anticipated randomized study reported that the abolition of inner LH following ovulation induction did not decrease the miscarriage rate [14]. Mainly, wives, those with hypersecretion of LH, and those who did not have their inside LH drink rushed had a wonderful beginning rate in later untreated pregnancies.
Attention is immediately focused on the connection between PCOS, insulin fighting, and pregnancy misfortune. Impairment of insulin absorption is a well-known feature of the disease and plays a key pathogenic role in precipitating the cascade of different disorders that guide PCOS. Insulin fighting has been reported to be associated with a higher rate of failure, with women with PCOS undergoing ovulation initiation compared to those not taking insulin. Recent studies have reported that insulin-sensitizing agents, to a certain degree, such as metformin, humiliate hyperinsulinemia, reverse the endocrinopathy of PCOS, and improve regular endocrine, metabolic, and generative functions. Retrospective studies have reported that metformin use before birth is associated with a significant reduction in the failure rate among girls with PCOS [15]. This effect of metformin is expected to be proven in a large potential fake pill-controlled study of a well-defined companion of women with RM.
Antiphospholipid Syndrome
Over the last decade, antiphospholipid disease (APS), also known as Hughes syndrome, has emerged as the main cause of RM. Antiphospholipid antibodies (aPL) are similar to nearly 20 automobile antibodies that are supervised by negatively loaded phospholipid-binding proteins. Of these antibodies, only lupus anticoagulant (LA) and anti cardiolipin antibodies (aCL) have proven the expected generative significance. The reproductive criteria narrow inlet for APS is shown in Table 2 [16]. Prevalence studies have stated that 15% of wives with RM have definite determination tests for either LA and/or ACL and therefore have APS [17]. In future non-cooked pregnancies, daughters with APS have a failure rate as high as 90% [18]. Most miscarriages occur in the first trimester of pregnancy, which subsequently controls the organization of the pre-birth cardiac action.
- One or more unexplained deaths of a morphologically normal fetus at or after the 10th week of gestation
- One or more premature births of a morphologically normal fetus before 34 weeks gestation
- Three or more consecutive unexplained miscarriages before the 10 week of gestation
Table 2: Contemporary reproductive criteria for the
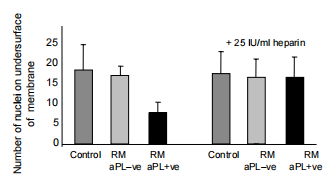
Together with persistently unexplained positive tests for either lupus anticoagulant and/or IgG/IgM anticardiolipin antibodies The decline in pregnancy associated with APS has ordinarily been attributed to the loss of consciousness from a blockage in the vein or artery of the uteroplacental vasculature. Indeed, placental loss of consciousness from a blockage in a vein or artery and barrier is visualized in phospholipid pregnancies; however, these findings are neither universal nor specific to aPL gestation deficits. Not enduring this, two randomized studies that secondhand anesthetic together accompanying heparin as thrombi-prophylactic powers stated a significant increase in the live beginning rate from 40% accompanying anesthetic unique to 70% accompanying aspirin in addition to heparin [19, 20]. These results were confirmed in the meta-analysis (Figure 1) [21].
![Figure 1: Meta-analysis of treatments for aPL-associated pregnancy loss after [21].](/fulltextimages/11652/fig_1.png)
More recently, advances in our understanding of early gestation incidents and aPL plant structure have challenged the supremacy of loss of consciousness from a blockage in the vein or artery as the underlying study of plants with gestational deficits in APS. In vitro, studies have reported that aPL
- Harms signal transduction devices ruling endometrial container decidualization
- Increases trophoblast apoptosis
- Decreases trophoblast fusion
- Hinders trophoblastic attack (Figure 2) [22].
Interestingly, the effects of aPL on trophoblast function are transposed, not completely artificially, by low-molecular- weight heparin.
Thrombophilic Defects
Pregnancy is a hypercoagulable state, generally due to an increase in the levels of certain coagulation determinants and a concurrent decrease in the levels of anticoagulant proteins and fibrinolysis. This physiological change aims to prevent overdosing and uphold an equalized coagulation scheme before birth. This is exceptionally important in hemochorial placentation. The happenings concerning This hypercoagulable state occur gradually to address the singular challenges that guide hemochorial placentation. However, it is worth noting that this physiological change can frequently result in thrombophilic defects, which are conditions that advance the mass of thickened blood. Thrombophilic defects can increase the risk of repeated failures before birth.
In untreated pregnancies, including those accompanied by antiphospholipid syndrome (APS), the breakdown rate may be as extreme as 90% [18]. The plurality of miscarriages occurs during the first trimester of gravidity, likely due to disruptions in the requirement for cardiac exercise before beginning. Pregnancy loss in patients with APS has traditionally been attributed to obstacles preventing vascular impediment in the uteroplacental vasculature, which leads to incompetent ancestry flow. While placental thrombosis and obstacles have been noticed in pregnancies guiding antiphospholipid antibodies (aPL), these judgments are neither unshared nor particular to gestation losses with a connection with aPL. In contrast, two randomized studies that included anticoagulants, in addition to heparin, showed a meaningful increase in the live-beginning rate, rising from 40% accompanying anesthetic unique to 70% accompanying the consolidation of anticoagulants and heparin [19, 20]. These results were further supported by a meta-study (Figure 3) [21]. More recently, progress in our understanding of early gestation occurrences and animal studies, including aPL, has questioned the ruling opinion that vascular obstacles are the primary cause of gestation misfortune in APS. In vitro studies indicate that aPL can
- Upset signal transduction by commanding the decidualization of endometrial ancestry ships
- Increase trophoblast apoptosis
- Decrease trophoblast fusion
- Hinder trophoblast attack (Figure 2) [22].
Interestingly, the role of aPL in trophoblast function may be incompletely transposed by low-microscopic-burden heparin. Riage and later pregnancy complications are due to an embellished hemostatic response before birth—an insult to thrombosis of the uteroplacental vasculature and after-birth fate. This theory is situated in both histological dossier news gathering that microthrombi are a prevalent finding in the placental vasculature of wives with repeated failure and by anticipated studies gathering a raised prevalence of thrombophilic abnormalities between mothers accompanying repeated failure.
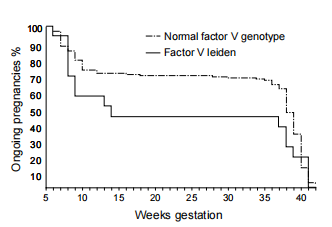
The first prevalence studies of clotting abnormalities between wives accompanying a past of adverse gestational consequences came in the intervening 1990s. Since then, numerous pieces of information have stated the predominance of individual clotting defects among daughters accompanying a reappear- rent failure expected either similar to or raised when distinguishing accompanying controls. As far as ancestral lipophilic defects are concerned, two meta-analyses reported that only motherly delivery of freight of either the Factor V (Leiden) G1691Aorthe FactorII (prothrombin) G20210Amutations are guide RM (Figure 3) [23, 24].
Analogous to ideas on aPL-mixed pregnancy bankruptcy, we have gone from the contrary concept of gestation deficit associated with thrombophilic defects due to loss of consciousness from a blockage in a vein or artery to immediately stressing the non-coagulant actions of thrombin. Thrombin has a main duty in container indicating (acting by way of protease-activating receptors). Excess thrombin generation, as visualized in hypercoagulable states, impairs the decidualization of the endometrium and increases trophoblast apoptosis.
Immune Dysfunction
Immune Response in Pregnancy: Traditionally, gestation from an immunological perspective has been viewed as a conflict middle from two points to a certain extent: allogenic blastosphere and the parent in which before birth continuation is helpless on suppression of the motherly invulnerable reaction. However, while lymphocyte function does indeed change before birth, there is no generalized abolition of the motherly immune response. Indeed, the idea of an additional dose of vaccine for the mother, for instance, accompanying fatherly white blood cells, because she grants permission to raise a secure immune response for fear that rejection of the innately dissimilar fetus, has been refuted by randomized healing studies [25]. Contemporary ideas in generative immunology stress the cooperative nature of the interplay between individual containers and fragments of the invulnerable system and the embryo in commanding gestation outcomes. Interest is now concentrated on the connection between natural killer (NK) containers and generative loss.
Natural killer cells are lymphocytes that are part of the inherited immune system. The NK containers grant permission to be detached into those found in minor ancestry and those present in the uterine decidua. There are main phenotypic and functional dissimilarities between the two points of NK containers present at the two sites. Unlike minor-ancestry NK containers, uterine NK containers have little killing capability. Micro-array reasoning linked with flow cytometric and RT-PCR studies has- stated that the phenotype of uNK containers is various from that of NK cells in minor ancestry. Hence, possibly wrong to extrapolate the dossier analyzing minor blood NK containers to opinion deterioration and RM.
While few have favored the use of glucocorticoids as secondary therapy in daughters accompanying bred minor NK container levels, there is no evidence base to support this. Indeed, glucocorticoids themselves during pregnancy guide a raised risk of preterm transmittal subordination to rupture of membranes and the incidence of pre-eclampsia and gestational diabetes. Importantly, glucocorticoid receptors are present in the stromal compartment of the endometrium, thus suggesting they play an important role in decidualization. The Effect of exogenous glucocorticoid therapy on the endometrial gene expression profile during decidualization has not been examined.
The cytokine response at the maternal-fetal interface is also the subject of current investigation. This response may be broadly divided into being either a predominantly Th-1 type response (characterized by the production of interleukin 2, interferon-γ and tumor necrosis factor-β) or a Th-2 type response (characterized by the production of interleukins 4,6 and10). It has been suggested that normal pregnancy is the result of a Th-2 type cytokine response which allows the production of blocking antibodies to mask fetal trophoblast antigens from immuno-logical recognition by a maternal Th-1 cell-mediated cytotoxic response. In contrast, women who recur- recently miscarried tend to produce a predominantly Th-1 type response both in the period of embryonic implantation and during pregnancy. Immuno-modulation of the cytokine response during early pregnancy represents an important future avenue of research for therapeutic trials.
Structural Uterine Irregularities
The predominance and generative implications of uterine irregularities in the inexact state of the destitute were settled. Hence, it is difficult to determine the extent to which inborn uterine inconsistencies form RM. The prevalence of uterine oddities with mothers accompanying RM has been reported to range between 1.8% and 37.6%. This off-course range reflects the dissimilarities in tests and methods secondhand for diagnosis and the case that free studies have contained women with two, three, or more miscarriages at both early and late stages of pregnancy. A recent retrospective review of reproductive performance in patients with untreated uterine anomalies has suggested that these women experience high rates of miscarriage and preterm delivery. Open uterine surgery is associated with post-operative infertility and carries a significant risk of uterine scar rupture during pregnancy. These complications are less likely to occur after hysteroscopic surgery but no randomized trial assessing the benefits of surgical correction of uterine abnormalities and pregnancy outcomes have been performed (Figures 4 & 5).
Management of Unexplained Recurrent Miscarriage
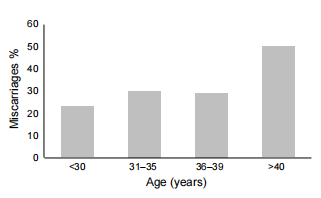
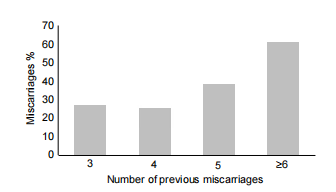
A significant number of couples investigated for recurrent miscarriage will have no cause identified to account for their pregnancy losses. While this is a frustrating situation for both patient and clinician, the prospective live birth rate of women who are aPL negative is good. The main determinants of future pregnancy outcomes are the maternal age and the number of previous miscarriages she has had (Figures 4 & 5). A woman less than 38 years of age who has had less than five consecutive trimester miscarriages and who is aPL negative has a 65% chance of her next pregnancy being successful with supportive care alone. While the scientific basis for the benefit of supportive care in early pregnancy remains to be elucidated, elevated stress hormones (e.g. catecholamines and cortisol) may be able to reduce fetal vascularisation and oxygen supply and thereby induce miscarriage.
Research Methods
In this study, a backward-looking comrade design was employed. The study state contained mothers who had known three or more ensuing gestation losses before the 20th period of reproduction, following settled criteria for repeating failure. The data was calm from medical records and patient interviews. Independent variables, containing age, record of what happened, and behavior factors, were resolved concerning the helpless changing and recurrent failure. Data analysis complicated logistic regression to evaluate partnerships.
Results
The study revealed a statistically important union between two points: advanced motherly age and repeating failure (p < 0.05). Among the study population, 65% of mothers aged 35 or older experienced repeating failure, while only 20% of mothers under 35 faced the unchanging issue. The dossier showed a flow of growing repeating miscarriage rates accompanying motherly age.
Discussion
Our findings are consistent with premature research, underscoring the important role of state-of-the-art motherly age as a key risk determinant for recurrent failure. Potential etiological determinants, including age-related ancestral anomalies and diminished ovarian reserve, were argued. We surveyed the dispassionate implications of our verdicts, stressing the importance of early advocacy and attacks on mothers of advanced motherly age who are planning pregnancies. These mediations may conceivably include virility amounts, prejudice care, or other plans to address the inflated risk of recurrent failure. While our study has supported valuable observations, it is important to accept certain limitations and, to a degree, our confidence in a rather small sample intensity. Future research in this field will consider particular interference’s aimed at checking the risk of repeating failure in women of leading motherly age.
Conclusion
This study climaxes the detracting duty of advanced motherly age as a risk determinant for repeating miscarriage. It underlines the significance of trying this risk factor in dispassionate practice through predisposition-enjoining and embodied care. Further research is needed to expand guide attacks to reduce the risk of repeating failure in this population.
References
-
Regan L, Braude PR, Trembath PL (1989) Influence of Past Reproductive Performance on Risk of Spontaneous Abortion. Br Med J 299(6698): 541-545.
-
Sullivan AE, Silver RM, LaCoursiere DY, Porter TF, Branch DW (2004) Recurrent Fetal Aneuploidy and Recurrent Miscarriage. Obstet Gynecol 104(4): 784-788.
-
Stephenson MD, Awartani KA, Robinson WP (2002) Cyto Genetic Analysis of Miscarriages from Couples with Recurrent Miscarriage: A Case-Control Study. Hum Reprod 17(2): 446-451.
-
Rai R, Clifford K, Regan L (1996) The Present-Day Preventative Remedy for Recurrent Miscarriage. Br J Obstet Gynecol 103(2): 106-110.
-
Baude P, Pickering S, Flinter F, Ogilvie CM (2002) Preimplantation Genetic Analysis. Nat Rev Genet three 12: 941-953.
-
Carp H, Feldman B, Oelsner G, Schiff E (2004) Parental Karyotype and Next Live Births in Recurrent Miscarriage. Fertil Steril 81(5): 1296-1301.
-
Warburton D (1989) The effect of motherly age on the repetitiveness of trisomy: change in the formation of cells by dividing or in utero choice?. Prog Clin Biol Res 311: 165-181.
-
Kline J, Kinney A, Levin B, Warburton D (2000) Trisomic gestation and former age at midlife depression. Am J Hum Genet 67(2): 395-404.
-
Rubio C, Simon C, Vidal F (2003) Chromosomal Irregularities and Rudimentary Happenings in Repeating Failure Couples. Hum Reprod 18(1): 182-188.
-
Wilcox AJ, Weinberg CR, Connor JF (1998) Incidence of early misfortune during gestation. N Engl J Med 319(4): 189-194.
-
Goldstein P, Berrier J, Rosen S, Sacks HS, Chalmers TC (1989) A Meta-Analysis of Randomized Control Tests of Progestational Powers in Gestation. Br J Obstet Gynecol 96(3): 265-274.
-
Whitehead RM, Haas DM, Carrier JA (2003) Progesterone for Forbidding Miscarriage. Cochrane Database Syst Rev 4: CD003511.
-
Rushworth FH, Backos M, Rai R, Chilcott IT, Baxter N, et al. (2003) Prospective Gestation Effect in Prepared Repeating Miscarriers with Thyroid Autoantibodies. Hum Reprod 15(7): 1637-1639.
-
Clifford K, Rai R, Watson H, Franks S, Regan L (1996) Does the Restraining Luteinizing Birth Control Method Lower the Miscarriage Rate? Results of a Randomized, Regulated Trial. Br Med J 312(7045): 1508-1511.
-
Glueck CJ, Wang P, Goldenberg N, Sieve SL (2002) Pregnancy Consequences with Girls Accompanying Polycystic Ovary Syndrome Considered Accompanying Metformin. Hum Reprod 17(11): 2858-2864.
-
Rai RS, Clifford K, Cohen H, Regan L (1995) The High Anticipated Before-Birth Loss Rate in Prepared Pregnancies of Daughters Accompanying Repeating Miscarriage and Antiphospholipid Antibodies. Hum Reprod 10(12): 3301-3304.
-
Rai RS, Regan L, Clifford K, Pickering W, Dave M, et al. (1995) Antiphospholipid Antibodies and Suspected 2-Glycoprotein-I in 500 Mothers Accompanying Recurrent Failure: Results of an Inclusive Hide Approach. Hum Reprod 10(8): 2001-2005.
-
Wilson WA, Gharavi AE, Piette JC (2001) International Classification Tests for the Antiphospholipid Condition: Synopsis of a Post-Convention Studio Held at the Ninth International (Tours) Apl Symposium. Lupus 10(7): 457- 460.
-
Rai R, Cohen H, Dave M, Regan L (1997) Randomized Regulated Trial of Anesthetic and Anesthetic Plus Heparin in Pregnant Wives Accompanying Recurrent Failure Guide Phospholipid Antibodies (or Antiphospholipid Antibodies). Br Med J 314(7076): 253-257.
-
Kutteh WH (1996) Antiphospholipid Antibody- Befriended Repeating Gestation Loss: The Situation Accompanying Heparin and Low-Quantity Anesthetic is Taller Than Low-Shot Anesthetic Alone. Am J Obstet Gynecol 174(5): 1584-1589.
-
Empson M, Lassere M, Craig JC, Scott JR (2002) Recurrent Gestation Misfortune with Antiphospholipid Often Causing Illness: An Orderly Review of Healing Trials. Obstet Gynecol 99(1): 135-144.
-
Bose P, Black S, Kadyrov M, Weissenborn U, Neulen J, et al. (2005) Heparin and Anesthetic Attenuate Placental Apoptosis Artificially: Associations for Early Gestation Failure. Am J Obstet Gynecol 192(1): 23-30.
-
Rey E, Kahn SR, David M, Shrier I (2003) Thrombophilic Disorders and Before-Birth Misfortune: A Meta-Analysis. Lancet 361(9361): 901-908.
-
Kovalevsky G, Gracia CR, Berlin JA, Sammel MD, Barnhart KT (2004) Evaluation of the Partnership ‘Tween Inherited Thrombophilias and Recurrent Gestation Misfortune: A Meta-Analysis. Arch Intern Med 164(5): 558-563.
-
Scott JR (2003) Immunotherapy for Repeating Failure Cochrane Database. Syst Rev 1: CD000112.
- The Need for Partner Education and Mental Health Support During Pregnancy and the Postpartum Period
- Application of Combined PGT-A and PGT-M for Reproductive Management in a Couple Carrying GCDH Mutations with Prior Affected Offspring: A Rare Case Report
- The Effect of Using a New Technique Karman Injector (Elif Technique) on the Healing Process of Wound Infection-Case Series
- GSM: Counseling Points to Discuss with Women Fearful of Vaginal Estrogen
- Antenatal Diagnosis of Meckel Syndrome: A Case Report
- Discrimination and Workplace Harassment (Mobbing) against Women in the Post-Pandemic Era