Therapeutic Clinical Implications of Insulin Resistance (IR) in Polycystic Ovary Syndrome (PCOS) in Lean/Obese PCOS Patients- Development of Non-alcoholic Fatty Liver Disease (NAFLD)-A Narrative Review
Polycystic ovary syndrome (PCOS) portrays a common which impacts the reproductive capacity as well as causes irregular menstrual cycles. Apart from criteria set at the time of Rotterdam syndrome ESHRE/ASRM-sponsored PCOS consensus, in the last decade, a newer problem insulin resistance (IR) has been observed more commonly along with subjects having PCOS greater IR in view of different for instance overweight in addition to obesity, however clarification is lacking in patients with PCOS who are of normal weight, thereby validating the posit that IR takes place independent of weight. It has been confirmed by proof that there is existence of the complicated pathophysiological conditions taking place resulting in dysfunctional post insulin receptor signalling particularly in PCOS patients having familial diabetes. Furthermore PCOS patients documented a greater incidence of non-alcoholic fatty liver disease (NAFLD) associated with hyperinsulinemia, which was observed to be greater in obese subjects having PCOS. Here in this narrative review we have concentrated on how as a further corollary to the in-depth work of the group of Genazzani AD; applications might be made with regards to utilization of very low-calorie ketogenic diet (VLCKD) along with Mediterranean diet (MD) for the treatment of PCOS apart from part of the glycaemic index in addition to glycaemic load in the generation of PCOS as well as prevention of its complications as well as trans generational transmission to the progeny.
Introduction
Polycystic ovary syndrome (PCOS) represents a disease which is substantially frequent, having an incidence of 5-21% in women at the time of their fertile duration (18- 45 year age) world over [1]. Clinical diagnosis of PCOS gets made with the utilization of Rotterdam’s criteria [2] (any two of the following three criteria after similar exclusion,
- Clinical (for instance acne, hirsutism) as well as /or biochemical androgen excess
- Chronic anovulation conditions (oligoovulation or anovulation till amenorrhea, and
- Micro polycystic morphology on ultrasonology transducer having a frequency bandwidth 8MHZ (≥20 follicles/ ovary, or an ovarian volume ≥10ml on any ovary [2, 3, 4].
Combination of these 3 criteria emphasizes 4 unique phenotypes of which maximum robust are where all 3 criteria are present [5]. Despite full prevalence of PCOS is akin over all countries, significant variations have been observed in view of ethnic factors impacting the phenotypic presentation of the syndrome for instance the prevalence of PCOS in case of Caucasian women varies from 4.7-6.8% [6]. Moreover, it has been displayed that once groups shift from one region to other regions, they have sustenance of susceptibility of their ethnicity to the generation of the PCOS in addition to the dysfunctional metabolism whose sustenance takes place secondary to hyperinsulinemia as well as/or diabetes mellitus (DM) as found for instance in women now based in Britain but are basically from Indian subcontinent Asian origin, who have greater prevalence of PCOS in addition to T2DM [6]. From these outcomes obtained manifestation it might be deduced that there exists an environmental as well as genetic constituent to PCOS in view of diet, exercise in addition to lifestyle possess broader ethnic differences.
Insulin resistance (IR) portrays a particular biological adaptation which stimulates a compensatory hyperinsulinemia in about 15-30% lean women having a diagnosis of PCOS established [3, 7]. IR is commonly observed in subjects having PCOS irrespective of their body mass index (BMI), taking into account that as much as 50% subjects having PCOS are overweight/ obese. Noticeably, overweight as well as obesity are commonly found in patients of PCOS with phenotype A, the maximum robust of the 4 phenotypes [5].
Sequentially these metabolic properties (for instance plasma insulin quantities assessment, body weight or BMI computation) need to be taken into account at the time of assessment of patients of PCOS. Actually, 2 alternate kinds of PCOS have been posited
- Canonical reproductive phenotype of PCOS in addition to a newer
- Having metabolic risk along with dysfunction known as ‘’metabolic reproductive syndrome’’ [8].
Earlier we had reviewed on the aetiopathogenesis of PCOS, part in perimenarchal girls, trans generational transmission of PCOS, advances in BAT physiology for PCOS treatment, role of flutamide identification of PCOS women at risk for generation of metabolic disease in normal weight PCOS as a predisposing factor for the generation of non- alcoholic fatty liver disease(NAFLD) [9, 10, 11, 12, 13, 14, 15]. In view of the germanises of the metabolic impact of PCOS here we have further concentrated on the newer aspects which have been recently elucidated.
Insulin Effects along with Insulin Resistance (IR)
The part of the insulin in case of mammals is of considerable significance in case of humans, insulin being the major controller of the glucose homeostasis resulting in induction of the glucose uptake in all the tissues inclusive of specifically adipose tissue (AT), muscle, heart, as well as liver. Insulin further leads to reduction of lipolysis, thus diminishing the quantities of the free fatty acids (FFA) in the blood that partially leads to modulation of the actions of the insulin on the generation of the glucose by the liver [16]. Apart from these metabolic actions, insulin possesses the part in the form of the cogonadotropin. In particular it results in the modulation of the ovarian working by augmentation of the effects of the luteinizing hormone (LH) on theca cells thereby taking part in the androgen liberation of androstenedione from the ovaries [17]. These cogonadotropin actions are partially direct in addition to partially indirect in view of insulin promotes the expression of its own receptor on the granulosa cells, however further on LH in addition to Insulin like growth factor 1 (IGF1 ) receptors. Once IR takes place, the escalated plasma quantities of the insulin lead to enhanced stimulation of the ovaries, causing over stimulation of the formation of the androgens [16, 17]. Clarification is present with regards to enhanced insulin apart from resulting in dysfunctional ovarian working, however further on the central neuroendocrine regulation of the reproductive axis (Figure 1) [18].
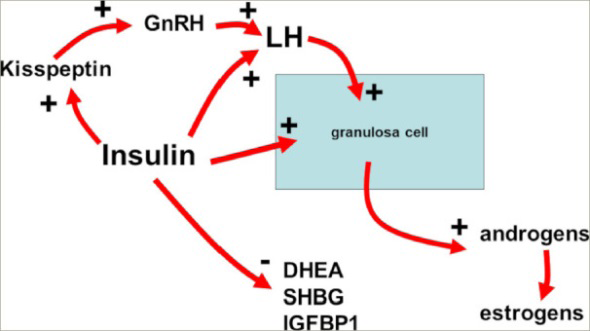
Insulin plays specific roles centrally on gonadotropin- releasing hormone through a positive action on kisspeptin release thus inducing luteinizing hormone secretion. At the ovarian level, insulin amplifies luteinizing hormone signalling and improves androgen production. Insulin also plays a role in sexual hormone-binding globulin production and in dehydroepiandrosterone release from the adrenal gland.
DHEA = Dehydroepiandrosterone; GnRH = Gonadotropin- releasing Hormone; IGFBP1 = Insulin-like Growth Factor Binding Protein 1; LH = Luteinizing Hormone; SHBG = Sex Hormone-binding Globulin.
Actually recent studies have displayed the association amongst Kisspeptin (Kp) in addition to gonadotropin releasing hormone (GnRH) stimulated liberation of LH ,the manner observed by the concurrent liberation of the pulsatile peaks of both the hormones [19]. Furthermore, KP as well as LH have been observed to be coliberated in case of eumenorrheic PCOS however not in the case of oligomenorrheic PCOS [20]. Additionally, plasma quantities of the insulin were observed to be significantly correlated with plasma quantities of LH as well as Kp in case of patients with PCOS along with functional hypothalamic amenorrhea (FHA) [1, 21]. In total ,these outcomes validate the posit that insulin possesses the germane part in the regulation of the reproduction in healthy situations as well as pathophysiological conditions for instance FHA [22], in addition to PCOS patients who are overweight as well as obese [21, 22]. Escalated insulin possesses the capacity of disrupting GnRH liberation at the hypothalamic level, via increased KP thereby resulting in escalated stimulation of gonadotropin liberation in addition to associated LH over liberation [2]. The converse takes place in FHA subjects [21]. Actually, FHA subjects display minimal quantities of insulin which are associated with the minimal quantities of LH. Thereby plasma insulin quantities are desirably not to be escalated in the blood along with any sort of escalation might be resulting in particular metabolic actions apart from the ones on the reproductive aspects. The part of the insulin is to keep the glucose quantities regulated; nevertheless for achieving this a significantly intricate network of hormones as well as peptides secreted basically from the pancreas (namely insulin) however further from the brain, liver, as well as from the adipose along with the muscle tissue. Amongst this network the pancreas possess a crucial part in release of blood glucose diminishing hormone insulin in addition to its antagonist glucagon [23]. In case of imbalanced insulin in addition to glucagon equilibrium with plasma insulin escalating in the existence of the normal plasma glucose quantities, IR occurs; that greater insulin quantities are needed for the sustenance of the normal glucose quantities in the blood flow for the sustenance of the glucose homeostasis (Figure 2) [23, 24].
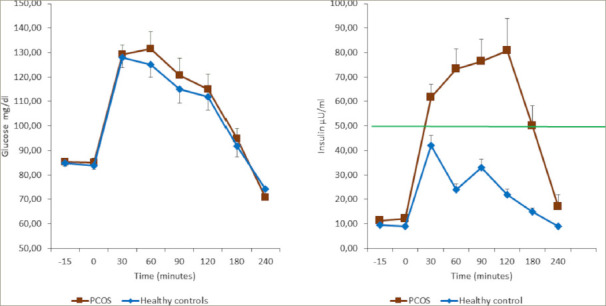
Though the glucose response was similar in both groups, the insulin response was higher in subjects with polycystic ovary syndrome. This observation suggests that, in patients who are obese with polycystic ovary syndrome, higher levels of insulin are needed to maintain normal glycaemic control. It cannot be excluded that such hyperinsulinemia response might be due to a reduced insulin clearance. The green line represents the actual maximal insulin response under oral glucose tolerance test considered within normality [19]. PCOS = polycystic ovary syndrome.
IR takes place once the capacity of insulin for the induction of its particular effects is diminished along with the metabolic uptake as well as generation of glucose along with dysfunctional lipolysis. Sequentially, a compensatory mode of liberating greater quantities of insulin occurs, in addition to greater quantities of insulin are liberated both at base line as well as subsequent to glucose load [7, 16].
IR possesses particular negative actions on certain organs in addition to tissues. In case of liver, as well as skeletal muscle, IR escalates lipolysis by the accrual of the non-esterified fatty acids (NEFA). Subsequent to accrual of lipids amongst the hepatocytes they cause activation of the diacyl glycerol (DAG)/ protein kinase C in addition to hampering of the insulin receptor [15, 16]. Within the skeletal muscle IR plausibly results in the induction of the hampering of the phosphatidyl inositol 3- kinase(PI3K) as well as phosphorylation of the insulin receptor substrate-1(IRS-1), thereby altering the expression of the glucose transporter 4 (GLUT4) vesicles as well as diminishing glucose upload [25].
Noticeably, IR takes place more commonly in PCOS subjects who are overweight as well as obese, specifically those having central obesity [4], nevertheless an exhaustive search illustrated that IR is further feasible in normal weight PCOS subjects irrespective of the BMI [7, 25].The corroboration that IR takes place in lean PCOS subjects pointing to the posit of the existence of the post receptor defect might be impacting the glucose upload [26, 27] instead of serine phosphorylation of the insulin receptor [8, 25]. Overweight/obese remains central for the initiation of the canonical PCOS symptoms, the manner it got illustrated recently by the meta-analysis performed by Behboudi- Gandevani et al. [28]. Noticeably, aberrant glucose regulation as well as /or type 2 diabetes (T2D) have further been found to be generated at a greater pace in contrast to control patients [28].This validation underpins the posit of the requirement of an oral glucose tolerance test (OGTT) [29], an approach for the determination of body’s reaction to glucose lasting for minimal 2 hours for determination of the insulin reaction under situations of metabolic stress. OGTT displays the patients hyperinsulinemia situation, once insulin reaction is greater than 50μU/ml within 30-90’ of glucose load [24, 30].
Insulin Signalling along with Insulin Resistance(IR): Part of Inositols
It is usually found that a greater proportion of the PCOS subjects having treatment with the utilization of insulin sensitizers (for instance metformin) find considerable enhancement apart from in metabolic along with hormonal paradigm, basically that of the hyperinsulinemia state, however further in the hyper androgenic signs with the return of the practically normal menstrual cycle along with working of the ovaries [31]. To our misfortune the dose of metformin is based on obesity grade in addition to their hyperinsulinemia situation, further greater the doses greater the gastrointestinal inimical sequelae [32]. Any deficiency in the inositol phosphoglycan (IPG) second messenger pathway might reason out hyperinsulinemia appearing through the dysfunction of post receptor insulin stimulated signal-this finding is the reason of posit of the innovative therapeutic approaches for the tackling of the hyperinsulinemia in case of PCOS subjects [33]. Actually, IPG portrays a necessary biological step in the transport of a particular metabolic along with hormonal signals formed subsequent to insulin gets associated with the membrane receptor. Generation of the IPG takes place at the level of the cellular membrane subsequent to hydrolysis of the glycerol phosphatidyl inositol lipids with placement on the internal of the cell membrane [34], followed by which IPGs become an integral part of the post receptor intracellular mode which is parallel to the second messenger .This insulin stimulated intracellular mode regulates the oxidative as well as non-oxidative metabolism in addition to glucose uptake by GLUT4 from the extracellular milieu [8, 35]. In view of this utilization of Inositols have been done in the form of an integral approach for the improvement of the cellular reactions to the metabolic stepwise patterns whose activation takes place subsequent to insulin binding to its receptor .Nevertheless, apart from insulin, other peptide hormones, for instance thyroid stimulating hormone (TSH), follicle stimulating hormone (FSH) further utilize them in the form of the second messengers [34, 36]. Inositols are part of a family comprised of 9 isomers, of which just 2 are germane for the modes detailed earlier namely
- My inositol (Myo)
- D chiroinositol (DCI) Inositols are existent in plants, vegetables for instance beans as well as fruits. Despite belonging to the vitamin group it possesses a chemical formula which is akin to glucose in addition to possesses the capacity of being generated by human biology, however maximum production of the inositols takes place from food [7, 37]. On gaining entry into the cells its conversion takes place into phosphatidyl-myo- inositol followed by to inositol triphosphate that constitutes the actual second messenger of peptide hormones (for instance insulin ,FSH, TSH) [34, 38]. As per Larner et al. [39], a particular balance is the requirement amongst 2/9 isomers of inositol that implies amongst Myo as well as DCI. Just one variation is present at the position of one hydroxyl group along with DCI gets obtained from Myo by the actions of epimerase [39].
The manner cited previously a particular balance is the requirement exists amongst Myo as well as DCI [39, 40]. Particularly both Myo as well as DCI are germane for regulation the right transportation of the metabolic signals of insulin subsequent to its binding with the membrane receptor. Insulin binding with its receptor causes activation of particular kinase stepwise patterns that in turn results in activation of phosphorylation of protein kinase B (AKT) which leads to translocation of the GLUT 4 vesicles on the cell membrane to upload glucose [39]. Additionally, insulin binding initiates one more stepwise pattern of processes which results in transformation of the Myo into DCI via the activation of enzymes phospholipase as well as epimerase [35]. DCI stimulates induction of glycogen synthase in the cytoplasm for the transformation of glucose into glycogen in addition to simultaneously activating mitochondrial pyruvate dehydrogenase phosphatase that stimulates the oxidation of glucose in the mitochondria [7, 35]. It is well acknowledged that the part of Myo as well as DCI is germane biologically. Sustenance of an appropriate equilibrium amongst these 2 aids in an appropriate upload of sugar from the outer aspect of the cell ;via glucose oxidation within the mitochondria in addition to conversion of glucose into glycogen; a gradient of content is attained- aiding in extra glucose upload from the outer aspect of the cell via GLUT 4 vesicles [8]. The manner it can be thought vividly, what results in the alteration of the equilibrium amongst Myo as well as DCI influences glucose upload in addition to its conversion to glycogen or oxidation in the mitochondria. Particularly processes which possess the capacity of negatively influencing epimerases diminish DCI generation along with cause dysfunctional glucose upload, diminishing rate of glucose upload thereby insulin (hyperinsulinemia) for indemnity for dysfunctional Myo into DCI transformation.
Actually, studies performed on animals as well as humans having diabetes displayed existence of greater quantities of Myo urinary excretion whereas DCI was diminished [33, 40]. This observation is thought to be reasoned out by diminished expression along with/or biological action of the epimerases [41]. Sequentially, these outcomes corroborate the posit that IR takes place in view of an aberrant expression of the enzymes instead of other acknowledged causes [7]. In the form of an illustration of aberrant expression of the enzymes, different studies have concentrated on the part possessed by inositols on insulin sensitivity [7]. Despite Myo efficaciously diminished IR at the time of OGTT in case of normal weight patients with PCOS [25], a differential IR was found in overweight /obese PCOS patients [24]. This observation evoked the probability that particular factors (for instance the dysfunctional epimerase expression) might be the reason behind the differential actions of epimerase enzyme. Taking into account the earlier illustration with regards to changed DCI formation as well as urinary excretion [33, 41], clarification of biological importance of DCI was found on DCI delivered to overweight /obese PCOS patients [42]. All the patients illustrated reduction in insulinemia on utilization of an incorporated treatment in addition to improvement of IR the manner illustrated by OGTT; nevertheless, the individuals who documented the existence of familial diabetes in 1st degree relatives (parents/grandparents) illustrated a greater IR on utilization of OGTT as well as greater enhancement with treatment [43]. These events confirmed theposit that once DCI was incorporated positively, it rectified a reduction in endogenous DCI generation in case of familial diabetes.
Taking into account that diabetes might portray a robust factor which escalates the susceptibility for the diminished insulin sensitivity escalating IR along with hyperinsulinemia, it has been pointed that delivery of inositols might be based on the capacity of epimerise in the transformation of the Myo into DCI in enough quantities [42, 44]. In case of no such familial susceptibility, delivery of lone Myo appears feasible [45], or on Myo as well as DCI [46]; that once DCI was incorporated, possesses a key part in case of existence of familial diabetes [7, 42, 43, 44].
Alpha Lipoid Acid Modulation of Insulin Sensitivity Silently
Taking into account the complicated nature of human biology it is not feasible that just the inositols are implicated in the regulation of the cellular glucose uptake as well as thereby in regulating glycaemia in the biological fluids. Actually one more substance has been recently believed to be germane for the treatment of IR, namely alpha lipoid acid (ALA). In case of animal models ALA has been observed to modulate the utilization of glucose by escalating adenosine mono phosphate (AMP)-activated protein kinase (AMPK) in skeletal muscles, thereby escalating GLUT4 [45].
ALA has been further believed to be thioctic acid which is imperative for the working of different enzymes responsible for oxidative metabolism [46]. The Initial utilization of ALA was detailed in 1959 for the treatment of the mushrooms poisoning, particularly Amanita phyllodes poisoning [47]. ALA is frequently observed in the vegetables for instance spinach as well as broccoli in addition to tomatoes along with meats in case of mammals. Generation of ALA takes place in mitochondria by the enzyme, lipoid acid synthase (LASY): that possesses the capacity of getting down regulated in the variable situations for instance diabetes [48]. ALA as well as its reduced kind dihydro lipoid acid, possess a myriad of biochemical function
- working in the form of antioxidants (for instance metal chelators) that reduce the oxidized kinds of antioxidants (for instance Vitamin C,E as well as glutathione) in addition to modulation the signalling transduction of various pathways (for instance insulin along with nuclear factor κB (NFκB)) [45] of the plethora of functions
- ALA causes improvement of endothelial dysfunction
- Decreases OS subsequent to exercise training [49],
- Conferring protection against generation of atherosclerosis [49].
In view of these effects ALA might be a putative substance for the treatment of numerous chronic diseases having a considerable epidemiological, cost in addition to social influence ; for instance hypertension [50], Alzheimer’s disease [51], cognitive impairment as well as diabetes mellitus(DM) along with its complications [48].
Sequentially, ALA has been hypothesized in the form of a substance for numerous diseases, particularly DM along with PCOS in view of the existence of the aberrant dysmetabolic profile [52]. Recently, various studies have illustrated the remarkable effectiveness of ALA in regulating insulin sensitivity. Actually, recently it was observed that delivery of ALA at a dosage of 400 mg daily was efficacious in decreasing IR in addition to enhancement of insulin sensitivity in subjects having PCOS as illustrated by significant decrease in homeostatic model assessment index particularly in subjects having PCOS with familial diabetes [53]. These outcomes validate the point that delivery of ALA possesses the capacity of getting over the dysfunction canonically existence in case of familial diabetes which down regulates the expression of the LASY with in the mitochondria of mammals as well as in humans [48, 54]. Actually, decreased endogenous ALA generation, stimulates a lesser glucose uptake in skeletal muscle, on which is dependent the generation of insulin resistance (IR) [48].This deficient effect reduces AMPK quantities in skeletal muscles [55], thereby diminishing GLUT4 induction [46]. Nevertheless, apart from this advantage just subjects having familial diabetes illustrated plasma transaminase quantities intricate to the upper quantities of normality in addition to greater in contrast to patients not having familial diabetes [56, 57]. ALA delivery in case of subjects having familial diabetes significantly reduced LASY plasma transaminase quantities to normal plasma quantities. These observations are in agreement with the posit that the incorporation of the ALA delivery (simulating endogenous ALA) deplete maximum of the metabolic dysfunctions in subjects having PCOS particularly in familial diabetes.
The utilization of ALA for the treatment possesses considerable importance .As per a recent review non- alcoholic fatty liver disease (NAFLD) is observed in a remarkable proportion (40-70%) of PCOS patients [58], along with the combination of PCOS with obesity as well as IR is inimical as apart from stimulating NAFLD plausibly it further stimulates the generation of T2D [58]. The capacity of ALA delivery in diminishing transaminase quantities in subjects having familial diabetes validates the capacity of liver protection as detailed previously [47], along with pointing that ALA positively impacts liver working in subjects having PCOS by diminishing the risk of generation of liver dysfunction for instance NAFLD as well as subsequently T2D [53]. This counters one more illustration not in agreement with this posit or displaying these actions [59].
In view of these, in addition to taking into account the advantages of Myo as well as DCI, ALA has been incorporated with Myo/ DCI for the enhancement of advantageous actions over insulin sensitivity. Different studies have illustrated the advantageous actions of LASY the combination of ALA with Myo/ DCI significantly resulted in enhancement of the reproductive as well as metabolic results in subjects having PCOS with and without familial diabetes [56, 57]. Actually, in view of subjects having PCOS with familial diabetes exhibited diminished expression of the LASY in addition to that of epimerase, rectification of insulin sensitivity in addition to reproductive working apparently illustrates substantial enhancement on combination of ALA with DCI [56], that is considerably efficacious further once there is no familial diabetes [56]. The combination of ALA with Myo further causes improvement of the reproductive axis in addition to metabolic dysfunction; nevertheless, in familial diabetes it is not efficacious in overtaking the decreased expression / working of epimerise [59].
Hepatic Insulin Extraction-an Index of Hepatic Implication in Insulin Resistance(IR) in PCOS
A canonically silent in addition to asymptomatic hepatic disease is NAFLD. NAFLD is more commonly found however not possessing the properties of escalated transaminase quantities (for instance alanine amino transferase (ALT) as well as aspartate amino transferees (AST)) [58], which are believed to be germane pointers of the existence of NAFLD in view of usually intricate to the upper quantities of normality [42, 60]. Accumulating proof is escalating with regards to the sharing of akin stimulating factors [61], along with NAFLD has greater association with IR instead of liver fat levels [62]. The incidence of NAFLD in case of fertile women having PCOS has been correlated with IR, changed lipid quantities along with plasma androgen quantities [63]. Despite, androgen quantities might not vary amongst subjects having PCOS in addition to female subjects having NAFLD without PCOS [64], lesser quantities of Sex hormone binding globulin (SHBG) have been posited in the form of an acknowledged modulator amongst IR as well as NAFLD- SHBG portrays a steroid transporter in addition to pointer of the metabolic along with the nutritional status, whose hepatic generation is controlled by insulin [15, 58, 65].
Thereby clarification is there with regards to existence of an intricate association amongst IR as well as hyperinsulinemia along with the probable existence of hepatic dysfunctional state for instance NAFLD, which is plausibly correlated with escalated transaminase quantities. Sequentially, different studies have illustrated the existence of the dysfunctional insulin clearance in overweight /obese patients [66], akin to the overweight /obese PCOS patients [67]. Recently Genazzani AD, group conducted hepatic insulin extraction (HIE) index in PCOS patients who were either overweight or obese in addition to observed that HIE index suggested dysfunction particularly in subjects having PCOS with familial diabetes in a minimum in one 1st degree relatives(parents/grandparents) [67].
Utilization of different algorithms [64, 68] can be done for computation of HIE, where computation of the ratio amongst insulin as well as C peptide plasma quantities is substantially simple [68], Recent studies displayed that diminished liver working as well as the capacity of taking part in insulin clearance results in improvement of IR [64, 68]. From the physiological angle HIE portrays insulin kinetics meant in the form of balance amongst generation from the pancreas in addition to clearance imparted by liver. In view of clearance of C peptide is practically nil, C peptide might be meant to portray the insulin generation by the pancreas [69]. Actually, at the level of the pancreas, from the cleavage of pro- insulin, a molecule of insulin along with a molecule of C peptide is formed. Despite, at the level of the pancreas generation ratio amongst insulin along with C peptide is 1; computation of this ratio is feasible by the utilization of circulating quantities of the 2 peptides. In this manner the ratio substantially portrays the balance amongst insulin hepatic clearance kinetics as well as insulin release from the pancreatic βcells which is parallel to the quantities of C peptide, in view of in its practically negligible hepatic clearance [70]. Generally working of the liver performs around 50% of the extraction of the insulin that has been administered to it by the pancreas, 30% extraction is performed by kidney, 15-30% by muscles of whatever quantities are still there subsequent to the 1st pass in the liver (Figure 3) [71, 72].
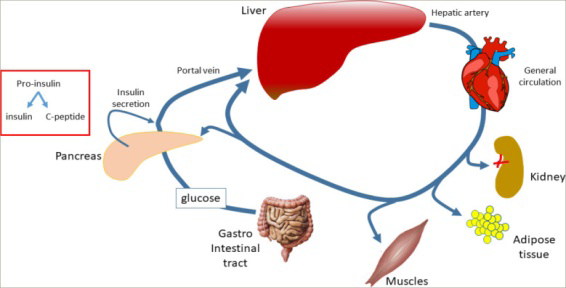
Insulin secretion from β cells of Langherhans islets of the pancreas derives from cleavage of pro-insulin into insulin and C-peptide, and the products are secreted into the portal vein. The blood passes through the liver, which extracts about 50% of the newly secreted insulin. The remaining insulin exits from liver and enters into the systemic arterial circulation via the hepatic veins. The remaining amount of insulin is removed while passing through the kidneys and the muscles. Whenever liver clearance ability is impaired, a lower amount of insulin is degraded.
HIE is based on the appropriate expression/generation of the insulin breakdown enzymes [69, 73]. Assessment of HIE has been performed in PCOS patients that are overweight /obese while taking into account if there was existence of familial diabetes in 1st degree relatives(parents/ grandparents) [74]. A study observed that apart from PCOS patients having familial diabetes possessed the greater plasma quantities of insulin in baseline situations, subsequent to overnight fasting, they further illustrated greater HIE in contrast to subjects not having PCOS with familial diabetes [61]. Additionally, PCOS patients having familial diabetes further illustrated ALT as well as AST plasma quantities the upper quantities of normality in addition to greater in contrast to patients not having familial diabetes [74]. These outcomes stimulate the deduction that a particular dysfunction might be stimulated bya familial susceptibility to diabetes impacting hepatocyte working. Actually, PCOS patients having familial diabetes illustrated greater IR in contrast to PCOS patients not having familial diabetes at the time of OGTT [61]. In view of C peptide reactions did not vary amongst the 2 groups HIE outcomes were greater in PCOS patients having familial diabetes practically all through the time of OGTT, in view of diminished hepatic insulin clearance [61]. Recently the incorporative strategy in PCOS utilization of lone ALA [53], or the combination of ALA with Myo [56], or DCI [57] illustrated greater effectiveness in PCOS patients having familial susceptibility to diabetes [58].
These outcomes validated the posit that the susceptibility to familial diabetes in certain manner apart from causing dysfunctional peripheral insulin sensitivity via lesser/ deficient expression/ generation, of both LASY in addition to epimerises however further the capacity of the hepatic insulin clearance when there is no familial diabetes, just overweight /obesity are implicated in the peripheral deficiency in insulin sensitivity , thereby stimulating a corrective greater insulin (in addition to generation); however in the existence of the familial diabetes the dysfunctional working/ generation of the LASY in addition to epimerase is extra to the deficiency in hepatic insulin clearance in view of deficiency in insulin breakdown enzymes working/their expression. The combination of these processes estimates greater circulating insulin (in view of over generation in addition to lesser clearance) in case of PCOS patients with familial diabetes in contrast to patients without familial diabetes. The more common existence of the escalated (despite not pathological) ALT as well as AST quantities have to be taken care of, it being a pointer of hepatic dysfunction. The combination of hyperinsulinemia in addition to escalated transaminases have been taken into account in the form of a stimulator of NAFLD which takes place more commonly in case of PCOS
patients in contrast to normal population [59].
How Utilization of Mitochondrial Dysfunction Might be Conducted to Unravel PCOS Pathophysiology
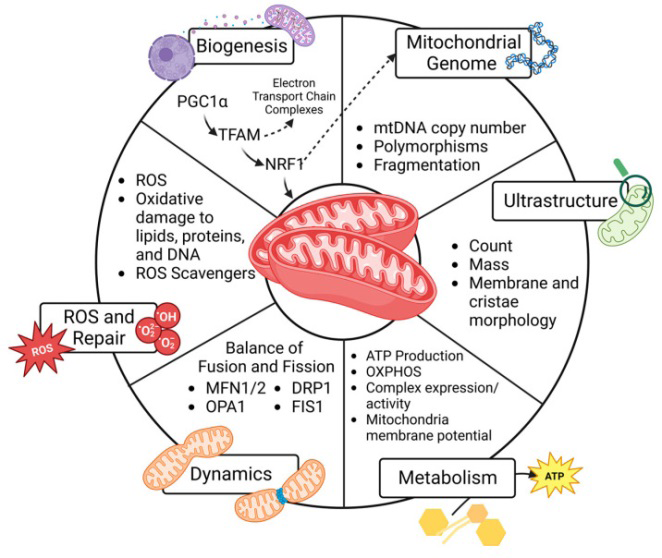
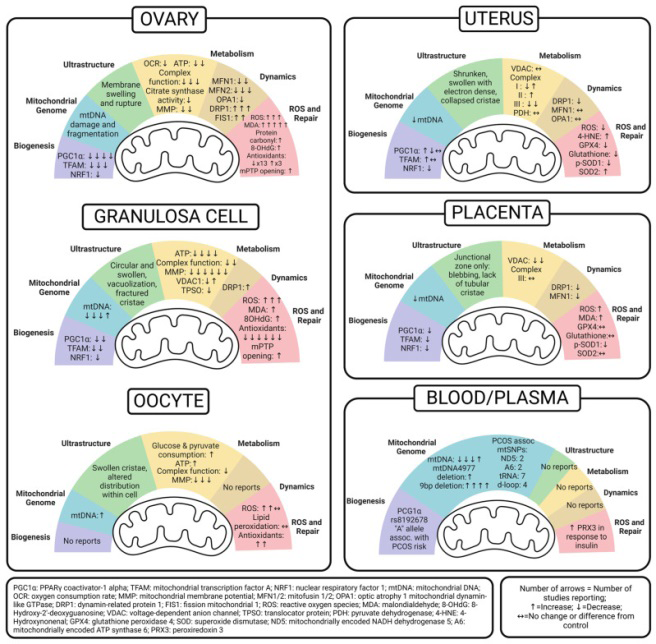
Having reviewed earlier the part of the mitochondrial unfolding protein response in reproduction and aging with use of autologous mitochondrial injections in mitochondrial diseases along with in aging oocytes here we further describe how it might be utilized in unravelling PCOS pathophysiology [75]. Recently Siemens, et al. [76], detailed six predefined mitochondrial functions, as illustrated in (Figure 4), as well as then summarize PCOS-correlated observations findings in the ovary (granulosa cells in addition to oocytes), uterus, placenta, along with peripheral circulation. The emerging designs are demonstrated in (Figure 5). Hopefully this work of theirs would lay the groundwork which is the requirement for generating of innovative diagnostic along with therapeutic strategies for people with PCOS in addition to ameliorate the trans generational sequelae for their progeny.
Summarizing their work in the whole ovary they documented that they observed that mitochondrial biogenesis as well as downstream mitochondrial quantity along with quality assessment have been performed in a wide variation of PCOS models. Even with separate models of PCOS induction, rodent models assessing biogenesis in whole ovary uniformly demonstrate decreased quantities of Peroxisome Proliferator Activated Receptor γ captivator -1α (PGC-1α), nuclear respiratory factor-1 (NRF-1), NRF-1, in addition to transcription factor A (TFAM) [75]. Metformin treatment escalated PGC-1α, as well as TFAM expression, the manner a traditional Chinese medicine, cangfudaotan decoction [75], neurokinin-B antagonist [75], two separate carnitine formulations [75], along with the overexpression of SIRT3; an NAD- based deacetylase did [75].
Just one study directly assessed mtDNA in ovarian tissue [77]. Jiang, et al. [77], documented greater injured in addition to fragmented mtDNA in the ovaries of a letrozole- induced rat model of PCOS that was further administered a high-fat diet, however the delivery of neither cangfudaotan or metformin significantly diminished mtDNA injury as well as fragmentation [77].
There was minimal documenting of mitochondria ultrastructure amongst the ovary as a whole, along with most studies examined this amongst particular cell kinds like the GCs in addition to oocytes. Jiang et al. [77], illustrated mitochondrial membrane swelling as well as rupture in ovarian tissue in addition to observed that cangfudaotan or metformin reduced the total percentage of injured mitochondria, despite not as little as in the control groups [77]. On the whole, Jiang’s [77], observations point that mtDNA injury further impacts ultrastructure, respiration, as well as downstream energy generation.
Numerous other studies assessed ATP quantities, complicated proteins, along with citrate synthase for getting insight with regards to the functional role of ovarian mitochondria in PCOS. Generally, ATP quantities were lesser in PCOS-exposed ovaries [75, 76], which might be explained by reduced bio generation as well as mitochondrial injury. Intriguingly, studies of neonatal ovaries exposed to PCOS in utero had ATP quantities akin to the controls [56]. Uniformly, all other rodent PCOS studies, excluding the in utero-exposed models, further documented lesser Complexes I, III, and IV, as well as total complex enzyme activity [76, 77]. Although the in utero exposed model did not exhibit complex enzymatic activity, the authors documented a lower expression of a particular subunit within Complex IV in contrast to the controls [76]. Dysfunctional complex activity in PCOS ovaries was rescued by cangfudaotan, Bushen Huatan Granules, or selenium delivered by nanoparticles [76, 77]. One study observed that that PCOS was correlated with lower citrate synthase activity however this escalated with the delivery of metformin or sodium selenite [76]. Furthermore, two akin studies uniformly documented that PCOS decreased the mitochondria membrane potential (MMP), which formed ATP-driving gradients in rat ovaries [76, 77]. In both cases, cangfudaotan along with selenium nanoparticles, in addition to metformin alone, caused improvement of MMP.
Just 2 studies determined real-time cellular bioenergetics to assess mitochondrial respiration. One study observed that PCOS led to a lower oxygen consumption rate (OCR) as well as respiratory control rate (RCR) in isolated mitochondria [77]. The other study examined bioenergetics via extracellular flux analyses in whole neonatal ovaries from an in utero PCOS-exposed rat model. PCOS-exposed neonatal ovaries had escalation of basal, maximal, along with ATP- correlated linked OCR, in addition to an escalated proton leak [77]. Together, these observations point that PCOS results in dysfunctional mitochondrial respiration in the adult ovary, however exposing the generating ovary to PCOS in utero causes a responsive increase in mitochondrial oxygen consumption that could be correlated with oxidative stress across a lifespan.
In studies evaluating the mitochondrial dynamics in the whole ovary, a common theme of imbalance was observed, specifically with dysfunctional fusion as well as escalated fission, a state that escalates mitophagy in addition to oxidative stress whereas impairing important networking with other organelles. For fusion, rodent studies observed lesser quantities of mitofusins 1 as well as 2(MFN1 as well as MFN2), optic atrophy 1 mitochondrial dynamin-like GTPase
(OPA1), however their expression quantities escalated with interventions of cangfudaotan, sodium selenite, or metformin [76, 77]. The fission genes DRP1 as well as FIS1 were greater in rat PCOS models however reduced with cangfudaotan, sodium selenite, or metformin [76, 77]. Many studies assessed oxidative stress (OS) in PCOS ovaries. Overall, PCOS escalated mitochondrial superoxide [76], lipid peroxidation (malondialdehyde (MDA)), and protein oxidation, along with DNA oxidation [77]. Cangfudaotan reverted increased ROS production [77]. Selenium, sodium selenite, metformin, in addition to genistein all successfully decreased MDA levels [76, 77], as well as metformin along with sodium selenite reduced protein carbonyls [76, 77]. Genistein treatment reversed DNA oxidation in DHEA-induced PCOS [76].
In addition to oxidative damage, some studies evaluated if PCOS possessed the capacity of changing the antioxidant capacity in the ovary, which would significantly influence its capacity to react to oxidative stress. Overall, the studies suggest that PCOS lowers antioxidant capacity, particularly SOD1 mRNA expression and SOD activity, in ovary tissue [76]. In contrast, two other studies observed increased quantities of SOD2 protein [76], which might be a cellular reaction to oxidative stress (OS). Others reported impaired GSH, glutathione peroxidase (GPx), GR, and GSH: GSSG ratio, whereas one study opposed this with reports of increased GSH-Px [76]. Three different studies observed decreased CAT activity, which got rescued with both genistein along with neurokinin-B antagonists [76]. Studying both ROS generation in addition to antioxidant capacity is significant in view of when once ROS exceeds antioxidant capacity, oxidative damage and cell death take place. This is highlighted by two studies that further did assessment of mitochondrial permeability transition pore (mPTP) opening as well as quantities of cytochrome C in the cytosol, both of which are primary controllers cell death. PCOS increased these markers in rat ovaries, but they were significantly reduced with cangfudaotan along with metformin, or Bushen Huatan Granules, respectively [76, 77]. They suggested that differences in antioxidant capacity within these studies are related to both the methods of PCOS induction and the timing of tissue collection, as antioxidant capacity might to start with be “overawed” by ROS however escalate over time in reaction to on-going OS.
Conclusions and Future Directions
Here the significance of the utilization of an appropriate strategy in the treatment of PCOS is emphasized apart from gynecolologic aspects; however from the aspect of the internal medicine specialists as well. The proof pointed that a greater existence of the dysmetabolic diseases for instance diabetes as well as dyslipidemia in addition to NAFLD along with non-alcoholic steatohepatitis (NASH) in case of PCOS patients particularly in the ones having familial diabetes; thereby particular assessment is warranted. In the case of their referral to a gynecolologist for any specific reproductive or simply irregular menstrual cycle in the form of the oligomenorrheic/amenorrhea, anovulation need a detailed metabolic assessment. Furthermore, Wang, et al. [78], illustrated that the PCOS patients with obesity possessed a significantly greater higher prevalence of NAFLD on performance of alteration in addition to impacting factors of liver controlled attenuation parameter (CAP). Additionally, in PCOS patients with obesity, liver CAP was correlated with abnormalities of lipid metabolism, insulin resistance, as well as hyperandrogenemia, with elevated testosterone quantities being an independent risk factor for NAFLD in PCOS patients with obesity. Moreover, as illustrated by us earlier these facts have made the application of very low-calorie ketogenic diet (VLCKD) along with Mediterranean diet (MD) in the treatment of PCOS as recently corroborated by Calcaterra, et al. [79], in adolescents with PCOS [79].
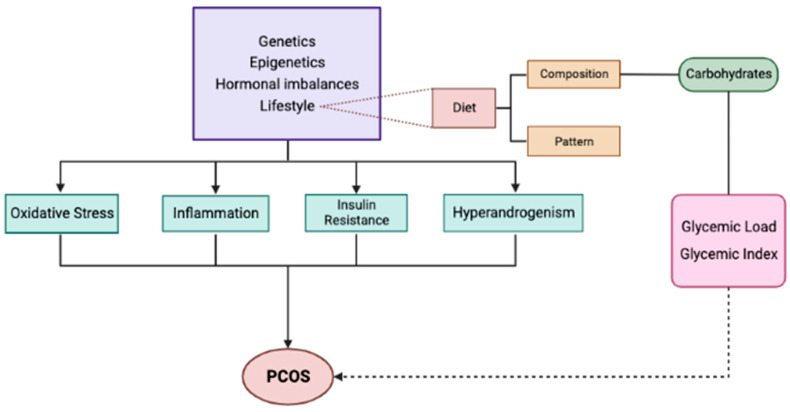
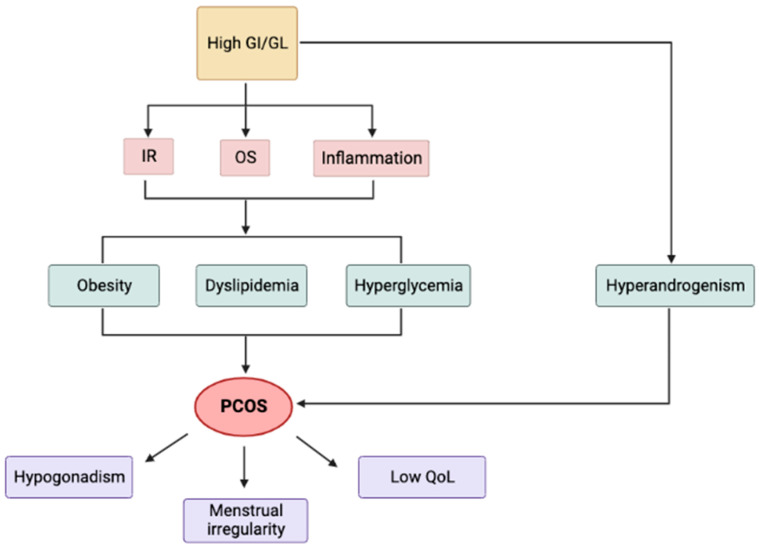
As a further corollary nutrition, with regards to nutrient constitution, dietary, endocrine-disrupting chemicals (EDC), as well as food processing along with preparation, that has acquired considerable interest in the pathogenesis in addition to the therapeutic strategy of PCOS. Manta, et al.
[80] emphasized on how carbohydrate ingestion is a key point in the diet recommendations. Glycaemic index as well as glycaemic load compose the indexes of the influence of dietary carbohydrates on postprandial glucose quantities. Numerous studies have indicated that a greater glycaemic index in addition to the glycaemic load diet might exaggerate insulin resistance, a critical characteristic of the syndrome, as well as a risk for its generation along with complications. On the other hand, low-glycaemic index in addition to low- glycaemic load diets apparently cause improvement of insulin sensitivity, menstrual cycles, and control as well as ameliorate the risk of comorbidities with PCOS, for instance obesity, changes in body constitution, type2 diabetes (T2D), cardiovascular disease, along with quality of life (QOL). The objective of this exhaustive review by Manta, et al. [80], was the exploration of the germanises of nutrition along with more particularly, the correlation of glycaemic index in addition to glycaemic load with the different perspectives of PCOS, in addition to evaluate the plausible advantages of manipulating those indexes in the dietary approach for the syndrome (Figures 6 & 7).
References
-
Azziz R, Woods KA, Reyna R, Key TJ, Yildiz OB, et al. (2004) The Prevalence and Features of the Polycystic Ovary Syndrome in an Unselected Population. J Clin Endocrinol Metab 89(6): 2745-2749.
-
Rotterdam ESHRE/ASRM- Sponsored PCOS consensus workshop group (2004) Revised 2003 Consensus on Diagnostic Criteria and Long Termrisks Related to Polycystic Ovary Syndrome (PCOS). Hum Reprod 19(1): 41-47.
-
Fauser BC, Tarlatzis BC, Rehar RW, Legro SR, Balen HA, et al. (2012) Consensus on Womens Health Aspects of Polycystic Ovary Syndrome(PCOS): The Amsterdam’s ESHRE/ASRM-Sponsored 3rd PCOS Consensus Workshop Group. Fertil Steril 97(1): 28-38.
-
Teede HJ, Misso ML, Costello MF, Dokras A, Laven J, et al. (2018) Recommendations from the International Evidence Based Guidelines for Assessment and of Polycystic Ovary Syndrome. Fertil Steril 110(3): 364- 379.
-
Walters KA, Gilchrist RB, Ledger WL, Teede HJ, Handelsman DJ, et al. (2018) New Perspectives on the Pathogenesis of PCOS: Neuroendocrine Origins. Trends Endocrinol Metab 29(12): 841-852.
-
Escobar-Morreale HF, Botella-Caretero JL, Alvarez- Blasco F, Sancho J, San Millan JL (2005) The Polycystic Ovary Syndrome Associated with Morbid Obesity May Resolve After Weight Loss Resolve Induced by Bariatric Surgery. J Clin Endocrinol Metab 90(12): 6364-6369.
-
Genazzani A (2020) Inositols: Reflections on How to Choose the Appropriate One for PCOS. Gynecol Endocrinol 36(12): 1045-1046.
-
Dunaif A, Fauser BC (2013) Renaming PCOS: A Two State Solution. J Clin Endocrinol Metab 98(11): 4325- 4328.
-
Kulvinder KK, Allahbadia GN, Singh M (2019) Role of Antimullerian Hormone as an Early Predictor of PCOS in Perimenarchal Girls-Role in Preventing Associated Comorbidities. J Gynecol 4(1): 000175.
-
Kulvinder KK, Allahbadia GN, Singh M (2023) Advancements in the Etiopathogenesis, Pathophysiology and Treatment of Polycystic Ovary Syndrome (PCOS)? - A Short Communication. EC Gynaecology 12(7): 20-23.
-
Kulvinder KK, Allahbadia GN, Singh M (2023) An update on Mechanistic Modes in AGEs Stimulated & ER and Inflammatory Stress- Modulated Control of the GLUT4 Expression (SLC2A4 promoted) and Thermogenesis in Diabetes mellitus - A Narrative Review. Mathews J Cytol Histol 6(1): 1-25.
-
Kulvinder KK, Allahbadia GN, Singh M (2018) Advances in BAT Physiology for Understanding and Translating into Pharmacotherapies for Obesity and Comorbidities. MOJ Drug Des Develop Ther 2(5): 166-176.
-
Kulvinder KK, Allahbadia GN, Singh M (2023) Role of Flutamide Identification of Women of Polycystic Ovary Syndrome (PCOS) At Risk for Generation of Metabolic Disease in Normal Weight PCOS: Is There a Role of Flutamide?- A Short Communication. CPQ Medicine 14(2): 1-6.
-
Kulvinder KK, Allahbadia GN, Singh M (2023) Will Exploration for Role of Kisspeptins Answer the Modes by Which Transgenerational Transmission of Polycystic Ovary Syndrome (PCOS) Occursto Find A Way of Avoidance of Inheritance of PCOS?- A Short Communication. MAR Case Reports 7(1): 1-17.
-
Kulvinder KK, Allahbadia GN, Singh M (2023) An Update on the Etiopathogenesis of Non-Alcoholic Fatty Liver Disease (NAFLD) Including Organokines for Early Diagnosis & Improvement of Management & Preventing Early HCC Development- A Narrative Review. Liver Res Open J 4(1): 18-41.
-
Armanini D, Boscaro M, Bordin L, SabbadinC (2022) Controversies in the Pathogenesis, Diagnosis and Treatment Of PCOS: Focus on Insulin Resistance, Inflammation and Hyperandrogenism. Int J Mol Sci 23(8): 4110.
-
Diamanti Kandrakis E, Dunaif A (2012) Insulin Resistance and the Polycystic Ovary Syndrome revisited : An Update on the Mechanisms and Implications. Endocrin Rev 33(6): 981-1030.
-
Genazzani AD, Genazzani AR (2023) Polycystic Ovary Syndrome as Metabolic Disease: New Insights on Insulin Resistance. Touch REV Endocrinol 19(1): 71-77.
-
Podfigurna A, Meczekalski-Jeske M, Meczekalski B, Genazzani AD (2020) Kisspeptin and LH Pulsatility in Patients with Functional Hypothalamic Amenorrhea. Endocrine 70(3): 635-643.
-
Katulski K, Podfigurna A, Cryzyk A, Meczekalski B, Genazzani AD (2018) Kisspeptin and LH Pulsatile Temporal Coupling In PCOS Patients. Endocrine 61(1): 149-157.
-
Genazzani AD, Podfigurna A, SzeligaA, Meczekalski B (2021) Kisspeptins in Female Reproduction: Fromphysiology to Pathophysiology. Gynec Reprod Endocrin Metab 2(3): 148-155.
-
Roder PV, WuB, LiuY, HanW (2016) Pancreatic Regulation of Glucose Homeostasis. Exp Mol Med 48(3): e219.
-
Genazzani AD, Prati A, Santagni S, Ricchieri F, Chierchia E, et al. (2012) Differential Insulin Response to Myoinositol Administration in Obese Polycystic Ovary Syndrome Patients. Gynecol Endocrinol 28(12): 969- 973.
-
Petersen MC, Schulman GI (2018) Mechanism of Insulin Actions and Insulin Resistance. Physiol Rev 98(4): 2133-2223.
-
Genazzani AD, Chierchia E, Ricchieri F, Campedelli A, Rattighieri E, et al. (2014) Myoinositol Modulates Insulin and Luteinizing Hormone Normal Weight Patients with Polycystic Ovary Syndrome PCOS. J Obstet Gynaecol Res 40(5): 1353-1360.
-
Baillargeon JP, Diamanti Kandrakis E, Ostlund RE, Nestler JE, Luorno JM, et al. (2006) Altered D Chiroinositol Clearance in Women with Polycystic Ovary Syndrome. Diabetes Care 29(2): 300-305.
-
Vrbikova J, Hainer V (2009) Obesity and Polycystic Ovary Syndrome. Obes Facts 2: 26-35.
-
Behboudi-Gandevani S, Ramezani TF, Rostani DM, Farahmand M, Khomami BM, et al. (2016) Insulin Resistance in Obesity and Polycystic Ovary Syndrome: Systematic Review and Meta**-**analysis of Observational Studies. Gynecol Endocrinol 32(5): 343-353.
-
Celik C, Tasdemir N, Abail R, Bastu E, Yilmaz M (2014) Progression to Impaired Glucose Tolerance Test or Type 2 Diabetes Mellitusin Polycystic Ovary Syndrome: A Controlled Follow up Study. Fertil Steril 101(4):1123- 1128.
-
Legro RS, Arslanian SA, Ehrmann DA, Hoeger KM, Murad MH, et al. (2013) Diagnosis and Treatment of Polycystic Ovary Syndrome: An Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab 98(12): 4565-4592.
-
Legro RS, Finegood D, Dunaif A (1998) A Fasting Glucose: Insulin Ratio is a Useful Measure of Insulin Sensitivity in Women with Polycystic Ovary Syndrome. J Clin Endocrinol Metab 83(8): 2694-2698.
-
Genazzani AD, Lanzoni C, Ricchieri F, Baraldi E, Casarosa E, et al. (2007) Metformin Administration is More Effective When Non-obese Patients with Polycystic Ovary Syndrome Show Hyperandrogenism and Hyperinsulinemia. Gynecol Endocrinol 23(3): 146- 152.
-
Kennington AS, Hill CR, Craig J, Bogardus C, Raz I, et al. (1990) Low Urinary Chiroinositol Excretion in Non- Insulin Dependent Receptor Diabetes Mellitus. N Engl J Med 323(6): 373-378.
-
Porcaro G, Gullo G, Carlomagno G, Bizzarri M, Unfer V, et al. (2014) Polycystic Ovary Syndrome: Features, Diagnostic Criteria and Treatments. Endocrinol Metab Syndr 3(3): 1000136.
-
Croze ML, Soulage CO (2013) P**o**tential and Therapeutic Interests of Myoinositol in Metabolic Diseases. Biochimie 95(10): 1811-1827.
-
Wild RA, Carmina E, Diamanti Kandrakis E, Dokras A, Talbott E, et al. (2010) Asssessment of Cardiovascular Risk and Prevention of Cardiovascular Disease in Women with Polycystic Ovary Syndrome (AE- PCOS). J Clin Endocrinol Metab 95(5): 2038-2049.
-
Bizzarri M, Carlomagno G (2014) Inositol: History of an Effective Therapy for Polycystic Ovary Syndrome. Eur Rev Med Pharmacol Sci 18(13): 1896-1903.
-
Thomas RM, Nechamen CA, Mazurkiewicz JE, Dias AJ, Ulloa-Aguirre A (2011) The Adapter Proteinappl1 Links FSH Receptor to Inositol 1, 4, 5 Trisphosphate Production and is Implicated Intracellular Ca2+ Mobilization. Endocrinology 152(4): 1691-1701.
-
Larner J, Brautigan DL, Thorner MD (2010) D Chiro- inositol glycans in Insulin Signalling and Insulin Resistance. Mol Med 16(11-12): 543-552.
-
Ortmeyer HK, Bodkin NL, Lilley K, et al. (1993) Chiroinositol Deficiency and Insulin Resistance. I. Urinary Excretion Rate of Chiroinositol is Directly Associated with Insulin Resistance in Spontaneously Diabetic Rhesus Monkeys. Endocrinology 132(2): 642- 645.
-
Sun T, Heimark DB, Nguyen T, Nadler LJ, Larner J (2002) Both Myoinositol to Chiroinositol Epimerase Activities and Chiroinositol to Myoinositol Ratios are Decreased in Tissues of GK Type 2 Diabetic Rats. Biochim Biophys Res Commun 293(3): 1092-1098.
-
Chalasani N, Younossi ZM, Lavine AE, Charlton M, Cusi K, et al. (2018) The Diagnosis and Management of Non- alcoholic Fatty Liver Disease: Practice Guidance from the American Association for the Study of Liver disease. Hepatology 67(1): 328-357.
-
Genazzani AD, Santagni S, Ratighieri E, Chierchia E, Despini G, et al. (2014) Modulatory Role of D Chiroinositol (DCI) on LH and Insulin Secretion in PCOS Patients. Gynecol Endocrinol 30(6): 438-443.
-
Genazzani AD (2016) Inositol as a Putative Integral Treatmentfor PCOS. Reprod Biomed Online 33(6): 770- 780.
-
Gomes MB, Negrato CA (2014) Alpha Lipoic Acid as a Pleiotropic Compound with Potential Therapeutic use in Diabetes and in other Chronic Diseases. Diabetes Metab Syndr 6: 80.
-
Golbidi S, Badran M, Laher I (2011) Diabetes and Alpha Lipoic Acid. Front Pharmacol 2: 69.
-
Bock E, Schneeweiss J (1959) Ein Beitrag Zur Therapie Der Neuropathia Diabetic. Munch Med Wochenschrift 43: 1911-1912.
-
Padmalayam I, Hasham S, Saxena U, Pillarisetti S (2009) Lipoic Acid Synthase (LASY): A Novel Role in Inflammation, Mitochondrial Function and Insulin Resistance. Diabetes 58(3): 600-608.
-
Mc Neilly AM, Davison GW, Murphy MH, Needam N, Trinick T, et al. (2011) Effect of α- Lipoic Acid and Put on Cardiovascular Disease Risk in Obesity with Impaired Glucose Tolerance Test. Lipids Health Dis 10: 217-222.
-
Vasdev S, Ford CA, Parai S, Longerich L, Gadag V (2000) Dietary Alpha Lipoic Acid Supplementation Lowers Blood Pressure in Spontaneously Hypertensive Rats. J Hypertens 18(5): 567-573.
-
Moreira PI, Harris PLR, Zhu X, Santos SM, Oliveira RC, et al. (2007) Lipoic Acid and N-Acetyl Cysteine Decrease Mitochondrial Related Oxidative Stress in Alzheimer’s Disease Patient Fibroblasts. J Alzheimer’ Dis 12(2): 195-206.
-
Scaramuzza A, Giani E, Redaelli F, Ungheri S, Macedoni M, et al. (2015) Alpha Lipoic Acid and Antioxidant Diet Help to Improve Endothelial Dysfunction in Adolescents with Type 1 Diabetes: A Pilot Trial. J Diabetes Res 2015: 474561.
-
Genazzani AD, Shefer K, Della Casa D, Prati A, Manzo A, et al. (2018) Modulatory Effects of Alpha Lipoic Acid (Ala) on Insulin Sensitivity in Obese PCOS Patients. J Endocrinol Invest 41(5): 583-590.
-
Morikawa T, Yasuno R, Wada H (2001) Do Mammalian Cells Synthesize Lipoic Acid? Identification of a Mouse C DNA Encoding a Lipoic Acid Synthase Located in Mitochondria. FEBS Lett 498(1): 16-21.
-
Genazzani AD, Prati A, Marchini F, Petrillo T, Simoncini T et al. (2019) Differential Insulin Response to Oral Glucose Tolerance Test (OGTT) in Overweight /Obese Polycystic Ovary Syndrome Patients Undergoing to Myoinositol (myo), Alpha Lipoic Acid(Ala) or Combination of Both. Gynecol Endocrinol 35(12): 1088-1093.
-
Genazzani AD, Drespini G, Santagni S, Prati A, Rattighieri E, et al. (2014) Effects of a Combination of Alpha Lipoic Acid and Myoinositol on Insulin Dynamics in Overweight/ Obese Patients with PCOS. Endocrinol Metab Synd 3(3): 1000140.
-
Genazzani AD, Prati A, Simonocini T, Napolitano A (2019) Modulatory Role of D Chiroinositol and Alpha Lipoic Acid Combinationon Hormonal and Metabolic Parameters of Overweight /Obese PCOS Patients. Eur Gynaecol Obstet 1(1): 29-33.
-
Genazzani AD (2020) Expert’s Opinion: Integrative Treatment with in Ositos and Lipoic Acid for Insulin Resistance of PCOS. Gynec Reprod Endocrinol Metab 1: 146-157.
-
Macut D, Bozic Antic I, Bjekic Macutj, Tziomatos K (2017) Polycystic Ovary Syndrome and Non-alcoholic Fatty Liver Disease. Eur J Endocrinol 177: R145-R158.
-
Bae JC, Rhee EJ, Lee WY, Park ES, Young C, et al. (2011) Combined Effects of Non-alcoholic Fatty Liver Disease and Impaired Fasting Glucose on the Development of Type 2 Diabetes. Diabetes Care 34(3): 727-729.
-
Genazzani AD, Battipaglia C, Petrillo T, Alberti C, Patrizi B, et al. HIE (Hepatic Insulin Extraction) Index in Overweight/ Obese PCOS Patients with or without Familial Diabetes. Gynecol Reprod Endocrinol Metab 3(1): 57-68.
-
Legana AS, Monti N, Fedeli V, Gullo G, Bizzarri M (2014) Does Alpha Lipoic Acid Improve Effects on Polycystic Ovary Syndrome. Eur Rev Med Pharmacol Sci 26(4): 1241-1247.
-
Loria P, Adinolfi LE, Bellentani S, Grieco A, Gasbarrini A, et al. (2010) Practice Guidelines for the Diagnosis and Management of Non-alcoholic Fatty Liver Disease. A Decalogue from the Italian Association for the Study of Liver (AISF) Expert Committee. Dig Liver Dis 42(4): 272-282.
-
Ulzschneider KM, Kahn SE, Polidori DE (2019) Hepatic Insulin Extraction in NAFLD Related to Insulin Resistance Rather than Liver Fat Content. J Clin Endocrinol Metab 104(5): 1855-1865.
-
Anstee QM, Targher G, Day CP (2013) Progression of NAFLD to Diabetes Mellitus, Cardiovascular Disease or Cirrhosis. Nat Rev Gastroenterol Hepatol 10(6): 330- 344.
-
Dawson AJ, Sathyapalan T, Smithson JAI, et al. (2014) A Comparison of Cardiovascular Risk Indices in Patients with Polycystic Ovary Syndrome with and Without Non-alcoholic Fatty Liver Disease. Clin Endocrinol 80(6): 843-849.
-
Pascal N, Amouzou EKS, Sanni A, et al. Serum Concentration of Sex Hormone Binding Globulin Are Elevated in Kwashiorkor and Anorexia Nervosa but not in Marasmus. Am J Clin Nutr 76(1): 239-244.
-
Genazzani AD, Prati A, Genazzani AR, Battipaglia C (2020) Synergistic Effects of the Integrative Administration of Acetyl L-Carnitine, L-Carnitine, L- Arginine and N-Acetyl Cysteine on Metabolic Dynamics and on Hepatic Insulin Extraction in Overweight/Obese Patients with PCOS. Gynecol Reprod Endocrinol Metab 1(1): 56-63.
-
Fosam A, Sikder S, Abel BS, et al. (2020) Reduced Insulin Clearance and Insulin-Degrading Enzyme Activity Contribute to Hyperinsulinemia in African Americans. J Clin Endocrinol Metab 105(4): e1835-e1846.
-
Tura A, Ludvik B, Nolan JJ, Pacini G, Thompaseth K (2001) Insulin and C peptide Secretion and Kinetics in Humans: Direct and Model based Measurements During OGTT. Am J Physiol Endocrinol Metab 281(5): E966-E974.
-
Koh HC, Cao C, Mittendorfer B (2022) Insulin Clearance in Obesity and Type 2 Diabetes. Int J Mol Sci 23(2): 596.
-
Eggleson EM, Jahn LA, Barrett EJ (2007) Hyperinsulinemia Rapidly Increases Human Muscle Micro vascular perfusion but Fails to Increase Insulin Clearance: Evidence that Saturable Process Mediate Muscle Insulin Uptake . Diabetes 56(12): 2958-2963.
-
Leissring MA, Gonzalez Cassimirio CM, Merrino B, Suire NC, Perdomo G, et al. (2021) Targeting Insulin Degrading Enzymes in Insulin Clearance. Int J Mol Sci 22(5): 2235.
-
Genazzani AD, Battipaglia C, Semprini E, Arnesano M, Ambrosetti F, et al. (2022) Familial Diabetes in Obese PCOS Predisposes Individuals to Compensatory Hyperinsulinemia and Insulin Resistance (IR) Also for Reduced Hepatic Insulin Extraction(HIE). Endocrine 3(2): 296-302.
-
Kulvinder KK, Allahbadia GN, Singh M (2020) Role of Mitochondrial Unfolding Protein Response in Reproduction and Aging with Utilization of Autologous Mitochondrial Injections in Mitochondrial Diseases along with in Aging Oocytes. J Gynecol 5(1): 1-14.
-
Siemens KM, Klein AK, Baack ML (2023) Mitochondrial Dysfunction in PCOS: Insightsinto Reproductive Organ Pathophysiology. Int J Mol Sci 24(17): 13123.
-
Jiang XL, Tai H, Xiao XS, Zhang SY, Cui SC, et al. (2022) Cangfudaotan Decoction Inhibits Mitochondria- Dependent Apoptosis of Granulosa Cells in Rats with Polycystic Ovarian Syndrome. Front Endocrinol 13: 962154.
-
Wang D, Nan N, Bing H, He B (2023) Controlled Attenuation Parameters to Assess Liversteatosis in Obese Patients with Polycystic Ovary Syndrome. Front Endocrinol 14: 1241734.
-
Calcaterra V, Cena H, Sottotetti F, Hruby C, Madini N, et al. (2023) Low-Calorie Ketogenic Diet: Application in the Treatment of Polycystic Ovary Syndrome in Adolescents. Nutrients 15(16): 3582.
-
Manta A, Paschou SA, Isari G, Mavroiedi I, Kalantaridou S, et al. (2023) Glycemic Index and Glycemic Load Dietary Estimatesin the Approach of Polycystic Ovary Syndrome. Nutrients 15(15): 3483.
- The Need for Partner Education and Mental Health Support During Pregnancy and the Postpartum Period
- Application of Combined PGT-A and PGT-M for Reproductive Management in a Couple Carrying GCDH Mutations with Prior Affected Offspring: A Rare Case Report
- The Effect of Using a New Technique Karman Injector (Elif Technique) on the Healing Process of Wound Infection-Case Series
- GSM: Counseling Points to Discuss with Women Fearful of Vaginal Estrogen
- Antenatal Diagnosis of Meckel Syndrome: A Case Report
- Discrimination and Workplace Harassment (Mobbing) against Women in the Post-Pandemic Era