Lateral Cervical Epidermal Inclusion Cyst in a Paediatric Patient: A Rare Case Report
Epidermal inclusion cysts (EICs) are benign lesions that are widely encountered in adults but less common in children. This article describes the case of a thirteen-month-old child who developed a rapidly increasing cystic swelling on his left side of the neck, which was diagnosed as an epidermal inclusion cyst. The patient recovered without incident following a complete surgical resection. This example highlights the need of early detection, precise diagnosis, and surgical intervention in avoiding complications.
Goyal P¹*, Kumawat K¹ and Roy S²
¹Consultant ENT and Head & Neck surgeon, Apollo ENT hospital, India ²Pathologist at Sterling Accurris, India
Abbreviations
EICs: Epidermal Inclusion Cysts; MRI: Magnetic Resonance Imaging; CT: Computed Tomography; FNAC: Fine Needle Aspiration Cytology; CECT: Contrast Enhanced Computed Tomography.
Introduction
Epidermal inclusion cysts are typically seen superficially in the subcutaneous space and originate solely from ectodermal tissue. According to histology, they have squamous epithelial and frequently include keratinaceous debris. Since it is thought that acquired cysts arise from the traumatic implantation of a part of the skin into the underlying layers, they are frequently referred to as inclusion cysts [1, 2]. This can lead to the ectopic creation of a dermal cyst lined with squamous epithelium in any related area. Preoperative imaging using magnetic resonance imaging (MRI), computed tomography (CT), or ultrasonography may be necessary for diagnosis and surgical planning, depending on the extent and depth of these lesions [1, 3]. Direct surgical excision is an option for the majority, and every attempt should be taken to remove the cysts without rupturing them and causing contents to flow. Unlike dermoid cysts, epidermoid cysts of the neck are rare and typically seen in the midline and submental area. In this report, we describe a unique example of a neck epidermoid cyst that started in the left lateral cervical region.
At the Apollo ENT hospital in Jodhpur, Rajasthan, a thirteen-month-old boy arrived with a four-month history of a painless, steadily growing swelling on the left side of his neck. There was no history of trauma, infection, or previous procedures in the area for the patient. His parents stated that although the tumor had progressively grown in size, there was no pain or noticeable impairment in his ability to function.
Physical Examination
A well-defined, non-tender, movable, subcutaneous lump that measured roughly 2 × 2 cm was palpable on the left lateral part of the neck (level II and III neck area) during the physical examination (Figure 1). There were no indications of infection or irritation on the skin above. No anomalies, including regional lymphadenopathy, were seen.

Investigations
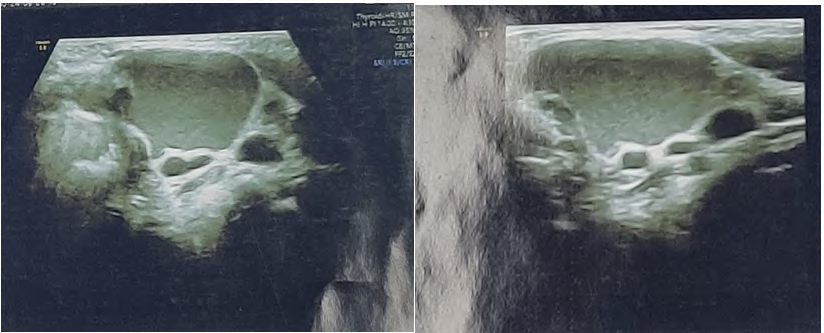
A well-defined, hypoechoic lesion without any vascularity or solid components was seen during a neck ultrasound, which suggested the presence of a benign cystic mass Figure 2. The results of the fine needle aspiration cytology (FNAC) test supported the presence of a benign cyst.
Surgical Management
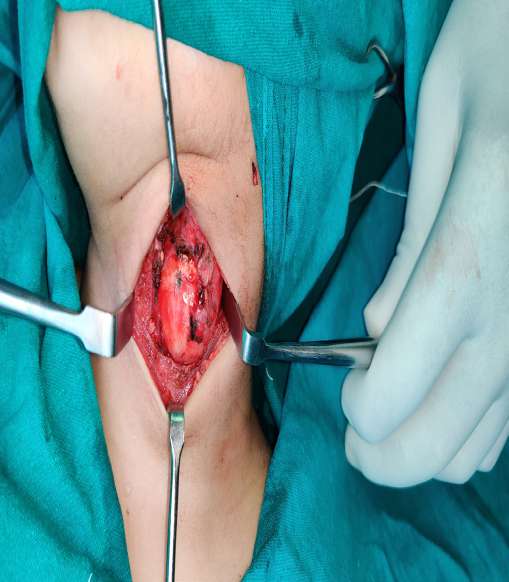
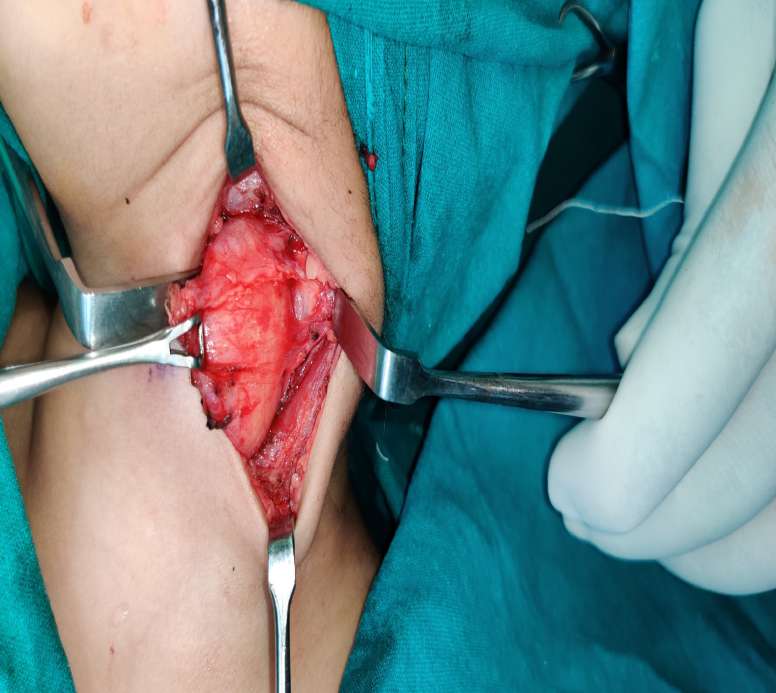
The decision was taken to proceed with surgical excision due to the size and the possibility of future consequences, such as infection or discomfort. A transverse incision was made along the neck crease while under general anesthesia, and the cyst was carefully dissected to reveal it (Figure 3). To avoid recurrence, the entire cyst—including its capsule—was removed (Figures 4-7). After the specimen was submitted for histological analysis, the diagnosis of an epidermal inclusion cyst was verified. The sections show a cyst lined partly by stratified squamous epithelium with a prominent granular cell layer and partly by granulation tissue with keratin flakes embedded within (Figures 8a-d).


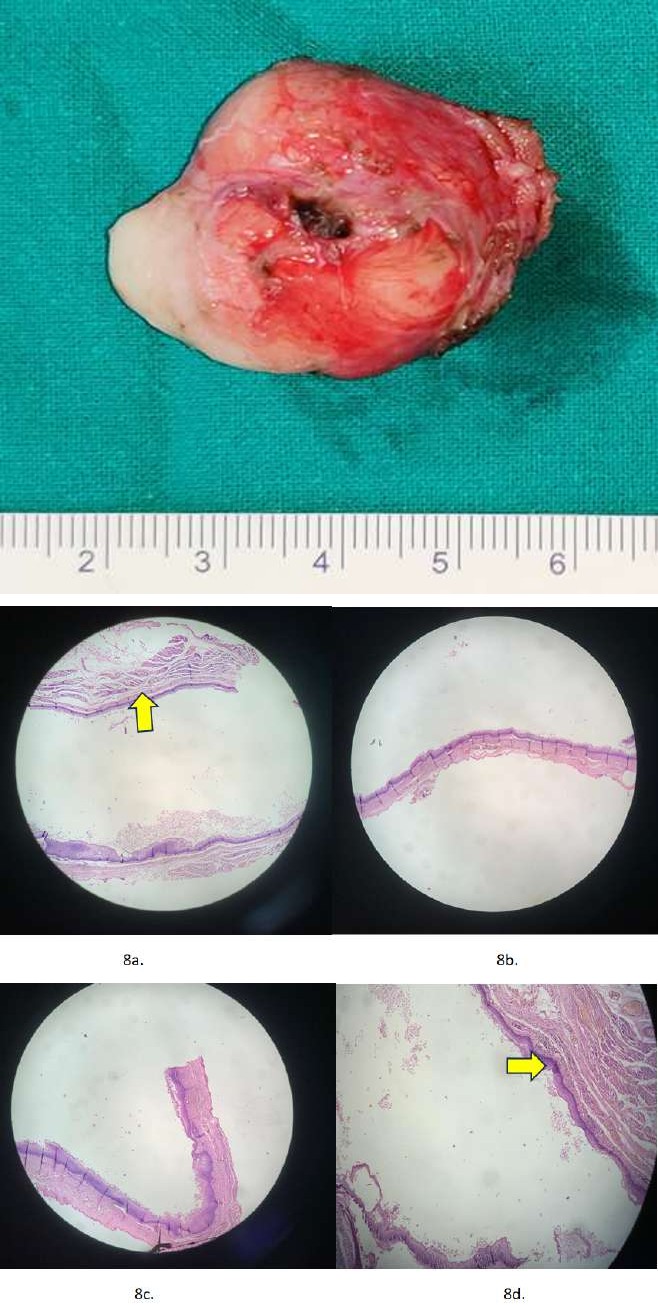
Figures 8a-d: Histopathological slides show a cyst surrounded by stratified squamous epithelium with a significant granular cell layer and granulation tissue with embedded keratin flakes (marked with arrow).
Postoperative Course
Following surgery, the patient made a full recovery without any issues. A follow-up at one month revealed a well-healed scar with no indications of recurrence, and the incision healed without any infection symptoms. The cosmetic result pleased the patient and their family.
Discussion
Children’s neck masses may create a diagnostic conundrum. It is believed that cellular failure during embryogenesis leads to an abnormal migration of ectodermal cells, resulting in congenital tumors called epidermoid cysts [4]. However, an acquired implantation theory contends that trauma or surgical procedures may cause germinal descendants to be implanted into deeper tissues, potentially resulting in epidermoid cysts [5]. Additionally, although the precise process of inheritance is yet understood, epidermoid cysts are a feature of many hereditary illnesses [6, 7]. With a preponderance of adult males, these cysts are the most common kinds of cutaneous cysts [8, 9, 10]. We have a fairly young male patient in our instance. Generally slow-growing, asymptomatic, and typically discovered until they reach adulthood, they are comparatively uncommon in children, as we found out [9, 10, 11].
We think that the condition in our case was a congenital epidermal cyst. Unusual and characterized by gradual growth, epidermoid cysts typically do not cause any symptoms [4]. In a few occasions, the cyst wall may burst and cause an inflammatory response in the dermis, and when they do develop, they are typically significant upon presentation. A history and physical examination of the cyst are sufficient to diagnose this condition. The diagnosis will be aided by radiological modalities. Imaging aids in identifying the type and extent of the lesion, and the interaction between the lesion and the neck muscles aids in choosing the best surgical strategy [6]. For the majority of cases, the diagnosis can be made with ultrasonography alone. In dubious individuals with uncommon presenting sites, magnetic resonance imaging and contrast enhanced computed tomography (CECT) play an additional role [11]. Histopathological analysis is the only way to arrive at a conclusive diagnosis. The majority of epidermoid cyst cases are seen in the midline of the neck and the submental region [12]. The cyst in our patient was located anteriorly in the lateral cervical area. This presentation is extremely uncommon. Histologically, the epidermoid cyst in our instance lacked skin appendages inside its wall, which is a characteristic that distinguishes it from a dermoid cyst. In the differential diagnosis, benign neoplasm or malignancy, infection and disruption of developmental processes should be taken into account. A cyst that grows quickly could be a sign of infection or malignancy.
Whether the objective is to correct a cosmetic defect or prevent future infection and malignant degeneration, we believe that total surgical excision is the greatest option for a successful course of therapy with a good prognosis and no recurrence. The recurrence rate of this cyst is low (<3%), and the prognosis is good [13, 14].
Conclusion
This instance emphasizes how crucial it is to identify pediatric patients’ epidermal inclusion cysts, especially in unusual places like the neck. Infection and recurrence can be avoided with early detection and total surgical excision. For the best results, surgeons should use the proper surgical management and take epidermal inclusion cysts into account when making a differential diagnosis for children’s neck tumors.
Compliance with Ethical Standards
The procedure performed in this case report was in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Funding
This study is not funded by any resources.
Conflict of Interest
The author (s) declares no potential conflicts of interest with respect to the research, authorship, and/or publication of this paper.
Ethical Approval
For the purpose of publishing this case report, the patient’s written informed consent was obtained.
References
-
Pryor SG, Lewis JE, Weaver AL, Orvidas LJ (2005) Pediatric Dermoid Cysts of the Head and Neck. Otolaryngol Head Neck Surg 132(6): 938-942.
-
Thomson HG (1990) Common Benign Pediatric Cutaneous Tumors: Timing and Treatment. Clin Plast Surg 17(1): 49-64.
-
Ahuja R, Azar NF (2006) Orbital Dermoids in Children. Semin Ophthalmol 21(3): 207-211.
-
Ozan F, Polat HB, Ay S, Goze F (2007) Epidermoid Cyst of the Buccal Mucosa: A Case Report. J Contemp Dent Pract 8(3): 90-96.
-
Hewitt DK, Kinney WC (2006) Two Cases of Incidental Epidermoid Cysts: Sphenoid Sinus and Temporal Bone. Ear Nose Throat J 85(12): 825-828.
-
Gorur K, Talas DU, Ozcan C (2004) An Unusual Presentation of Neck Dermoid Cyst. Eur Arch Otorhinolaryngol 262(4): 353-355.
-
Becker AK, Thomas I (2006) Epidermal Inclusion Cyst. eMedicine.
-
Al-Khateeb TH, Al-Masri NM, Al-Zoubi F (2009) Cutaneous Cysts of the Head and Neck. J Oral Maxillofac Surg 67(1): 52-57.
-
Dutta M, Saha J, Biswas G, Chattopadhyay S, Sen I, et al. (2013) Epidermoid Cysts in Head and Neck: Our Experiences, with Review of Literature. Indian J Otolaryngol Head Neck Surg 65(Suppl 1): 14-21.
-
Kim CS, Na YC, Yun CS, Huh WH, Lim BR (2020) Epidermoid Cyst: A Single Center Review of 432 Cases. Arch Craniofac Surg 21(3): 171-175.
-
Aihole JS (2020) Epidermoid Cyst at a Rare Location in a Child. J Craniofac Surg 31(2): 596-97.
-
Darmstadt GL, Sidbury R (2004) Tumors of the Skin. In: Behrman ER, et al. (Eds.), Nelson Textbook of Pediatrics. 17th (Edn.), Philadelphia, PA, WB Saunders Co, USA.
-
Manie MAB, Al-Qahtani KH, Ammar AA, Islam T, Otaibi FNA (2020) Epidermoid Cyst of the Suprasternal Region: A Rare Case Report. Braz J Otorhinolaryngol 86(1): 133- 135.
-
Morgan MB, Stevens GL, Somach S, Tamenbum M (2001) Carcinoma arising in Epidermoid Cyst: A Case Series and Aetiological Investigation of Human Papilloma virus. Br J Dermatol 145(3): 505-506.
- Origin, Evolution, and Functional Impact of Short Insertion- Deletion Variants in Human Genomes: A Review
- Harnessing Molecular Glues for Next-Generation Vaccine, Cancer and Cardiovascular Disease Drug Development: A Comprehensive Review
- Malarial Plasmodium Falciparum with Hepatitis B and C Virus Infections among Blood Donors in Ife Central Local Government Area, Ile Ife, Osun State, Nigeria
- Withanolides and Withaferin A- What’s next in Ashwagandha Research
- Designing of Dual Pulse Photoacoustic Tomography for Imaging of Drug-Response and Tumor Growth
- Trend Scenarios of Mortality due to Diabetes Mellitus and its Correlation with the Economic Sector, in the State of Mexico, for the Years 2020, 2025 and 2030