Perfusion Index Derived from Pulse Oximetry, Serum actate, its Surrogates and Beta Type Natriuretic Peptide (Bnp) for Outcome Prediction in Poly-Traumatized Patients. A Prospective Observational Cohort Study
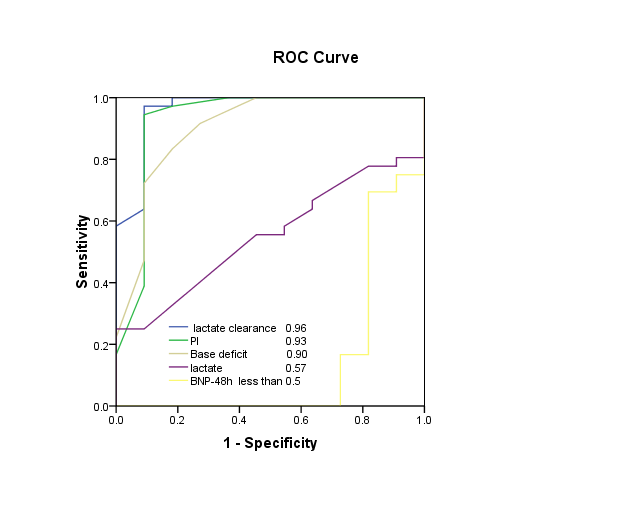
Introduction: Perfusion index (PI) is a non-invasive numeric value of peripheral perfusion; gained from pulse Oximeters. No study researched the predictive value of perfusion index in poly-traumatized patients. Patients and methods: Fifty adult poly-traumatized patients with blunt injury without head injury studied. Perfusion index compared to serum lactate lactate clearance, base deficit and beta Natriuretic peptide (BNP) in survivors and non-survivors and their predictability of mortality in a prospective observational study up to 48 hours in Assuit University tertiary hospital. Results: Perfusion index showed a significant difference between survivors and non-survivors after the first 6 hours, post resuscitation (p< 0.001). ROC analysis showed the ideal cutoff point for predicting mortality ≤ 0.75 with AUC 0.93, sensitivity 97% and specificity 82%. Non-survivors had significantly higher serum lactate than survivors (p< 0.001). ROC analysis showed the ideal cutoff point for predicting mortality ≥ 2.25 mmol/L with AUC 0.57, sensitivity 79% and specificity 69%. Survivors had significantly higher lactate clearance than non-survivors (p< 0.001). ROC analysis showed the ideal cutoff point for predicting mortality < 3.0 mmol/L/24 hours with AUC 0.97, sensitivity 97% and specificity 86%. Non-survivors had significantly higher beta Natriuretic peptide (BNP) at 48 hours than survivors (p< 0.001). ROC analysis showed the ideal cutoff point for predicting mortality ≥ 95.0 pg/ml with AUC less than 0.5, sensitivity 61% and specificity 32%. Conclusion: Perfusion index more than six hours after the injury is prognostic of mortality in adult poly-traumatized patients with blunt injury. Lactate clearance is prognostic of mortality. Serum lactate is a weak predictor of mortality in adult poly-traumatized patients with blunt injury. Beta Natriuretic peptide (BNP) has no prognostic value of mortality in adult poly-traumatized patients with blunt injury in this survey.
Key messages
- Lactate clearance is a useful prognostic factor of mortality in adult poly-traumatized patients with blunt trauma; AUC 0.96.
- The Perfusion index is a useful prognostic factor of mortality in adult poly-traumatized patients with blunt trauma; AUC 0.93.
- Serum lactate is a weak prognostic factor of mortality in adult poly-traumatized patients with blunt trauma; AUC 0.57.
- The beta Natriuretic peptide has no prognostic value of mortality in adult poly-traumatized patients with blunt trauma; AUC less than 0.5. Abbreviations: APACHE: Acute Physiology and Chronic Health Evaluation; ARF: Acute Renal Failure; ATLS: Advanced Trauma Life Support; AUC: Area Under the Curve; BD: Base Deficit; BNP: Beta Type Natriuretic Peptides; CO: Centigrade; CO2: Carbon Dioxide; CVP: Central Venous Pressure; DIC: Disseminated Intravascular Coagulopathy; EIA: Enzyme Immune Assay; ICU: Intensive Care Unit; IV: Intravenous; MAP: Mean Arterial Pressure; Mmol/l: Millimole Per Litre; NE: Nor Epinephrine; NT pro BNP: N-Terminal Pro Beta Natriuretic Peptide; OCT: Oxygen Challenge Test; PaCO2: Arterial Pressure Of Carbon Dioxide; PaO2: Arterial Partial Pressure Of Oxygen; PI: Peripheral Perfusion Index; PtcCO2: Transcutaneous Partial Pressure Of Carbon Dioxide; PtcO2: Transcutaneous Partial Pressure Of Oxygen; Pv-aCO2: Difference Between Central Venous And Arterial PCO2; RBCs: Red Blood Cells; ROC: Receiver Operating Characteristic; RTS: Revised Trauma Score; ScvO2: Central Venous Oxygen Saturation; SOFA: Sequential Organ Failure Assessment; SPSS: Statistical Package for the Social Sciences
Introduction
Major injury with severe hemorrhagic shock can progress to organ hypo-perfusion, failure and even death. Decreased perfusion because of intra-vascular volume depletion and hindered oxygen delivery results in regional hypoxia and anaerobic metabolism. The peripheral circulation first to suffer and last to regain blood flow during resuscitation; used as a target for monitoring compared to other prognostic markers of anaerobic metabolism as lactate and its surrogates. Even beta Natriuretic peptide (BNP) can predict the outcome of patients with major injuries [1]. Perfusion index (PI) is a non-invasive numeric value of peripheral perfusion; gained from pulse oximetery. Perfusion index is the ratio Alaa M Atia, et al. Perfusion Index Derived from Pulse Oximetry, Serum Lactate, its Surrogates and Beta Type Natriuretic Peptide (Bnp) for Outcome Prediction in Poly-Traumatized Patients. A Prospective Observational Cohort Study Anaesth Critic Care Med J 2016, 1(1): 000102.
of the pulsatile blood flow to the non-pulsatile static blood flow in patient’s peripheral tissue (pulsatile component / non-pulsatile component of the plethysmographic waveform × 100%) and is now displayed on some pulse Oximeters. In universal terms, PI reflects peripheral vasomotor tone. Low PI suggests peripheral vasoconstriction or severe hypovolaemia and high PI suggests vaso-dilatation. The PI’s value ranges from 0.2% for weak pulse to 20% for a strong pulse [2] It has been reported that perfusion index traced from pulse Oximeters can monitor peripheral perfusion in critically ill patients [3]. Recently, Huai-Wu and others, in a prospective observational study compared perfusion index to trans-cutaneous oxygen saturation/ carbon dioxide tension (ptcO2/ptcCO2), oxygen challenge test (OCT) in a group of septic patients. Perfusion index found similar to arterial lactate to predict mortality [4]. The value of non-invasive monitoring of peripheral perfusion to predict outcome remains to be explored in poly- traumatized patients. To the best of our knowledge, no study has addressed the sensitivity of perfusion index compared to lactate, its surrogates and serum beta Natriuretic peptide (BNP) to predict mortality in such critical poly-traumatized patients in a prospective study.
Aim of the Study
The aim of this prospective observational study was measuring the significance of perfusion index in poly- traumatized patients. The intent was to respond the following queries:
- Is perfusion index an independent predictor of death compared with serum lactate and lactate clearance within the first 48 hours post injury?
- Do serum lactate and lactate clearance predict mortality in poly-traumatized patients?
- How these two (perfusion index and serum lactate) change during the first 48 hours post injury?
- Is serum beta Natriuretic peptide (BNP) a predictor of mortality in poly-traumatized patients?
Patients and Methods
Setting: This prospective observational study conducted in the trauma emergency department and trauma ICU of Assuit University tertiary hospital in Upper Egypt, from June 2011 to December 2013. This study protocol approved by the local research ethics committee of Assuit University medical school and waived to require informed consent because the study design and intervention did not put critically ill patients at any unnecessary risk of harm or deviate from the best standard of care according Copyright© Alaa M Atia, et al.
to the state of the art. All written informed consents got from all patients’ and their respective parties. Agreeing to our institutional ethical committee policy, clinical data can be used for research without disclosing the patients' identities. Patient selection: Sixty patients admitted in the study; ten of them excluded: (Figure 1).
- Five patients taken out because of penetrating injury.
- Three patients taken out because of uncontrolled bleeding.
- Two patients excluded because of hypothermia.
This prospective trial was a non-randomized observational study of 50 adults poly-traumatized patients with blunt injury without head injury; admitted to the emergency department directly from the scene of injury; within 6 hours of the injury event and expected to stay 48 hours in the ICU; fulfilling the inclusion criteria and underwent resuscitation according to the advanced trauma life support protocol (ATLS 2008) [5]. The relevant history of all details about the accident and preexisting co-morbid illnesses adopted. I. Eligibility:
- Ages eligible for study: 16 - 60 years old.
- Genders eligible for study: Both.
Alaa M Atia, et al. Perfusion Index Derived from Pulse Oximetry, Serum Lactate, its Surrogates and Beta Type Natriuretic Peptide (Bnp) for Outcome Prediction in Poly-Traumatized Patients. A Prospective Observational Cohort Study Anaesth Critic Care Med J 2016, 1(1): 000102.
II. Inclusion criteria:
- Adults poly-traumatized patients with blunt injury without head injury.
- Mean arterial blood pressure ≤ 60 mmHg and/ or systolic arterial blood pressure ≤ 90 mm Hg. III. Exclusion criteria:
- Known pregnancy.
- Hypothermia (body core temperature < 36 CO).
- Patients admitted to the emergency department after 6 hours of injury.
- History of co-morbid cardiac disorder, uncontrolled hemorrhage, the failure of central venous catheterization, dialectic procedure expected during the survey period and liver failure. Study protocol: The study period corresponded to the outcome of the first 48 hours of trauma emergency department or ICU resuscitation. Patients immediately resuscitated on admission according to ATLS algorithm (2008) [5] and entered a prospective data set. The protocol aimed at normalizing perfusion parameters. Patients considered as successfully resuscitated if they had normal lactate levels (≤ 2 mmol/L) and stable macro hemodynamic parameters. Outcome measures defined by death during the first 48 hours of resuscitation and the patients recorded as survivors and non-survivors. Resuscitation: We used a standardized protocol for resuscitation of the patients, according to the advanced trauma life support guidelines (ATLS 2008) [5]. A careful, balanced approach with frequent reevaluation done as blood pressure and heart rate will not identify all injured patients who are in shock. Measurements: Protocol related measurements got in 0 hours (immediately after admission), 6, 12, 18, 24, 30, 36, 42 and 48 hours, post resuscitation for metabolic perfusion parameters (serum lactate, lactate clearance and base deficit). Perfusion index and Hemodynamic parameters (heart rate, central venous pressure, systolic, diastolic, and mean arterial blood pressure) got at admission and every hour after that. 1. Demographic characteristics: Age, sex and medical history reported. 2. The Revised Trauma Score (RTS) is a physiological scoring system, with high inter-rater reliability and proved accuracy in predicting death [6]. 3. Sequential Organ Failure Assessment (SOFA) [7]
collected for each patient at baseline (SOFA-0). Changes in SOFA score reported at 48 hours (SOFA-f).
Copyright© Alaa M Atia, et al.
4. Fluid and blood administration calculated and nor- adrenaline needs registered in the pre-established time points all over the whole study period (48 hours). 5. Peripheral perfusion parameters:
Peripheral perfusion index (PI): recorded on admission and every hour after that using Massimo SET Rad-5 handheld signal extraction oximetry (Massimo Corporation, USA) ®. MASIMO SET® Rad-5 is a fully featured handheld pulse oximeter with the accuracy and reliability of Massimo SET, perfect for both continuous monitoring and spot-checks applications (8). 6. Metabolic perfusion parameters:
- Serum lactate and lactate clearance: measured on admission and every six hours after that from a heparinized arterial sample using Stat Strip ® Lactate Xpress™ nova lactate point-of-care measuring system (Nova Biomedical Biosensor Technologies; USA). ®
- Base deficit: measured on admission and every six hours after that from a heparinized arterial sample by a blood gas analyser (Cobas b 221 Blood Gas system, Hoffmann-La Roche Ltd; Swiss). ©
- Serum beta Natriuretic peptide: BNP level assayed with EVOLIS BIORAD system based on RAYBio BNP. Enzyme immunoassay (EIA) kit is a (BIORAD LABORATORIES - USA) ®. In vitro quantitative assay for detecting BNP peptide based on the principle of competitive Enzyme Immunoassay.
Sensitivity: The minimum detectable concentration of BNP is 1.45 pg/ml, Concentration range: 0.1 - 1000 pg/ml. Data analysis: Receiver operating characteristic (ROC) curves used in medicine to discover a cutoff value for a clinical test; in some manner to downplay the number of false positives and false negatives. The ROC curve is a graph of sensitivity (y‐axis) versus 1- specificity (x‐axis). Minimizing the false positives and false negatives is the same as maximizing the sensitivity and specificity. Maximizing sensitivity matches to the large Y value of the ROC curve. Maximizing specificity matches to a small X value on the ROC curve, so a good first choice for a test cutoff value is the value which fits to a point on the ROC curve nearest to the upper left corner of the ROC graph. The important measure of the accuracy of clinical test is the area under the ROC curve. If this area is equal to 1.0 then the ROC curve consists of two straight lines, one Alaa M Atia, et al. Perfusion Index Derived from Pulse Oximetry, Serum Lactate, its Surrogates and Beta Type Natriuretic Peptide (Bnp) for Outcome Prediction in Poly-Traumatized Patients. A Prospective Observational Cohort Study Anaesth Critic Care Med J 2016, 1(1): 000102.
vertical from 0,0 to 0,1 and the next horizontal from 0,1 to 1,1. This test is 100% accurate because both the sensitivity and specificity are 1.0 so no false positives and no false negatives. The test that cannot discriminate between normal and abnormal corresponds to a ROC curve that is a diagonal line from 0,0 to 1,1. The ROC area for this line is 0.5. ROC curve areas are typically between 0.5 and 1.0. Two or more tests can be compared by statistically comparing the ROC areas for each test. Tests may be correlated because they occurred from multiple measurements of the same individual or they may be interrelated because they resulted from measurements of different individuals. The ROC Curves Analysis Module refers to this as Paired and Unpaired respectively, and can analyze either situation. Results for normally distributed continuous variables expressed as mean value, standard deviation and inter- quartile range. Categorical data and dichotomous variables showed as number and percentage. Comparisons of continuous variables performed using independent t. Test. The proportions compared with the chi - square test. All reported P values are 2-sided, with a significant α level of 0.05. Differences considered statistically significant if the null hypothesis could be rejected with 95% confidence (p< 0.05). Receiver operator characteristic (ROC) curve, a graph constructed to correlate true and false positive rates (sensitivity and 1 minus specificity, respectively). ROC curve can determine the ideal cutoff point for predicting mortality. Finally, we performed correlations and logistic regression to find out perfusion variables independently associated with mortality. The Area under ROC measures the ability to discriminate survivors from non-survivors. The SPSS version seventeen statistical software package (SPSS for Windows Release 17.0.0; SPSS Inc, Chicago, Ill, USA) ® package used for statistical analysis. It was practiced for all calculations, except ROC curve analysis, which performed using “medcalc 7” statistical software package available at <http://www.medcalc.org>.
Results
The study included 50 adults poly-traumatized patients with blunt trauma; fulfilling the inclusion criteria (43 men and 7 women), with a mean age (27.5± 8.0 years), of whom 36 survived (72%) and 14 non-survivors (28%) (Figure 2). The admission Revised Trauma Score (5.9236±0.3996) and the admission SOFA score (6.7±1.31), the final SOFA score (6.5±3.75). All over the 48-hour study period; patients received crystalloid volume (5700±2130.9 ml), colloid volume (1710±1030.6 Copyright© Alaa M Atia, et al.
ml), packed RBCs (4.6±1.6 units), fresh frozen plasma (3.42±2.5 units) and nor adrenaline doses (0.312±0.431 ug/kg/minute). Peripheral perfusion parameters include admission perfusion index (0.2±0.06). Hemodynamic parameters on admission showed a mean heart rate (149.3±6.1 beat/min), systolic blood pressure (60.12±11.08 mmHg), diastolic blood pressure (29.22±7.81 mmHg), mean blood pressure (39.52±8.21 mmHg) and central venous pressure (-3.98±1.64 cmH2o).
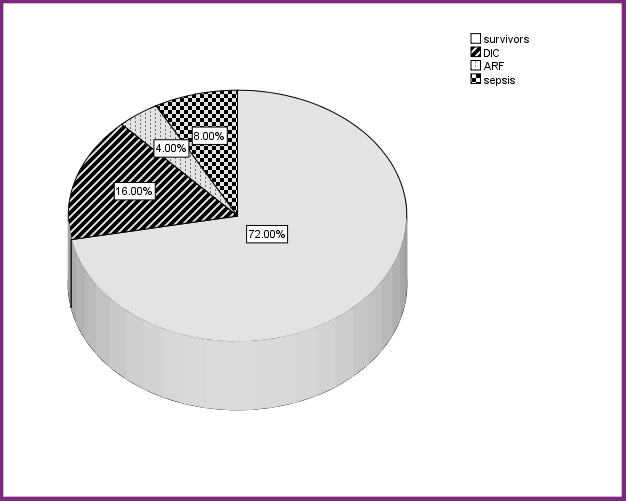
Figure 2: mortality and cause of death.
- DIC: Disseminated intravascular coagulopathy
- ARF: Acute renal failure Metabolic perfusion parameters showed a mean baseline serum lactate (6.9±1.7 mmol/L), mean base deficit (-20.3±2.8 mmol/L). The comparison between survival group and non-survival group about demographic data, revised trauma score (RTS), SOFA score, nor adrenaline dose and resuscitation by blood products and fluids. Age, sex, packed RBCs and fresh frozen plasma transfusion showed nonsignificant difference between survival and non-survival group. However, RTS, SOFA-0, SOFA-f, noradrenaline dose, The crystalloid and colloid volume used showed a statistically significant difference between survival and non-survival group (P< 0.05) and have significant correlation with mortality. Revised Trauma Score is a reliable predictor of mortality and had significant correlation with mortality (P< 0.001). Non- survivors had significantly lower RTS than survivors (P< 0.001). However, SOFA-0 and SOFA-f had significant correlation with mortality. Non-survivors had Alaa M Atia, et al. Perfusion Index Derived from Pulse Oximetry, Serum Lactate, its Surrogates and Beta Type Natriuretic Peptide (Bnp) for Outcome Prediction in Poly-Traumatized Patients. A Prospective Observational Cohort Study Anaesth Critic Care Med J 2016, 1(1): 000102.
significantly higher SOFA-0 and SOFA-f than survivors (P< 0.001). A significant correlation between nor adrenaline dose and mortality (P< 0.001) found. Nor adrenaline dose significantly higher in non-survivors (P< 0.001). Crystalloid and Colloid volume significantly correlated with mortality (P< 0.001) and significantly higher in non- survivors than survivors (P< 0.001). However, transfusion products (packed RBCs and fresh frozen plasma) had a statistically non significant correlation with mortality (P> 0.05).
Perfusion index changed significantly from baseline (PI- 0) (p< 0.001) in survivors and non-survivors. Perfusion index showed a non significant difference between survivors and non-survivors in the first six hours, post resuscitation. After the first 6 hours, post resuscitation; perfusion index showed a statistically significant difference between survivors and non-survivors (P< 0.01). Non-survivors had significantly lower PI than survivors (p< 0.001) (Figure 3).
Perfusion index changes in survivors and non survivors $$ \mathrm {E} = \frac {1}{2} \mathrm {A} ^ {2} + \mathrm {B} ^ {2} $$ $$ \diamond $$ $$ \mathrm {E} = \frac {1}{2} \mathrm {A} ^ {2} + \mathrm {B} ^ {2} $$ $$ \diamond $$ $$ \mathrm {E} = \mathrm {E} _ {1} + \mathrm {E} _ {2} + \dots + \mathrm {E} _ {n} $$ $$ \Delta $$ $$ \mathrm {E} = \frac {1}{2} \mathrm {A} ^ {2} + \mathrm {B} ^ {2} $$ $$ \Delta $$ $$ \mathrm {E} = \frac {1}{2} \mathrm {A} ^ {2} + \mathrm {B} ^ {2} $$ $$ \diamond $$ $$ \mathrm {E} = \frac {1}{2} \mathrm {A} ^ {2} + \mathrm {B} ^ {2} $$ $$ \Delta $$ $$ \diamond $$ $$ \mathrm {E} = \frac {1}{2} \mathrm {A} ^ {2} + \mathrm {B} ^ {2} $$ $$ \diamond $$ $$ \square $$ $$ \mathrm {E} = \mathrm {E} _ {1} + \mathrm {E} _ {2} + \dots + \mathrm {E} _ {n} $$ $$ \mathrm {E} = \frac {1}{2} \mathrm {A} ^ {2} + \mathrm {B} ^ {2} $$ $$ \square $$ $$ \square $$ $$ \mathrm {E} = \mathrm {E} _ {1} + \mathrm {E} _ {2} + \dots + \mathrm {E} _ {n} $$ $$ \square $$ $$ \mathrm {E} = \frac {1}{2} \mathrm {A} ^ {2} + \mathrm {B} ^ {2} $$ $$ \diamond $$ $$ \mathrm {E} = \mathrm {E} _ {1} + \mathrm {E} _ {2} + \dots + \mathrm {E} _ {n} $$ $$ \square $$ $$ \mathrm {E} = \frac {1}{2} \mathrm {A} ^ {2} + \mathrm {B} ^ {2} $$ $$ \square $$ $$ \mathrm {E} = \mathrm {E} _ {1} + \mathrm {E} _ {2} + \dots + \mathrm {E} _ {n} $$ $$ \mathrm {E} = \frac {1}{2} \mathrm {A} ^ {2} + \mathrm {B} ^ {2} $$ $$ \square $$ $$ \square $$ $$ \mathrm {E} = \mathrm {E} _ {1} + \mathrm {E} _ {2} + \dots + \mathrm {E} _ {n} $$ $$ \mathrm {E} = \mathrm {E} _ {1} + \mathrm {E} _ {2} + \dots + \mathrm {E} _ {n} $$ $$ \mathrm {E} = \mathrm {E} _ {1} + \mathrm {E} _ {2} + \dots + \mathrm {E} _ {n} $$ $$ \diamond $$ $$ \square $$ $$ \square $$ Figure 3: Perfusion index changes in survivors and non survivors. ROC curve analysis of perfusion index at 24 hours, post resuscitation; showed the ideal cutoff point for predicting mortality ≤ 0.75 with AUC 0.93, sensitivity 97% and specificity 82% (Figure 4).
Copyright© Alaa M Atia, et al.
Metabolic perfusion parameters
Serum lactate: Serum lactate changed significantly from baseline (admission lactate-0) (P< 0.001). Serum lactate showed a statistically significant difference between survivors (6.3±0.9 mmol/L) and non-survivors (8.3±2.5 mmol/L) (P< 0.01). Non-survivors had significantly higher first serum lactate levels than survivors. Serum lactate had a statistically significant positive correlation with mortality after the first 6 hours, post resuscitation (P< 0.001) (Figure 5).
serum lactate changes in survivors and non survivors
0 1 2 3 4 5 6 7 8 9
$$ \mathrm {E} = \frac {1}{2} \mathrm {A} ^ {2} + \mathrm {B} ^ {2} $$
$$ \square $$ $$ \mathrm {E} = \frac {1}{2} \mathrm {A} ^ {2} + \mathrm {B} ^ {2} $$ $$ \square $$ $$ \mathrm {E} = \mathrm {E} _ {1} + \mathrm {E} _ {2} + \dots + \mathrm {E} _ {n} $$ $$ \square $$ $$ \mathrm {E} = \frac {1}{2} \mathrm {A} ^ {2} + \mathrm {B} ^ {2} $$ $$ \mathrm {E} = \frac {1}{2} \mathrm {A} ^ {2} + \mathrm {B} ^ {2} $$ $$ \square $$ $$ \square $$ $$ \mathrm {E} = \frac {1}{2} \mathrm {A} ^ {2} + \mathrm {B} ^ {2} $$ $$ \square $$ serum lactate $$ \mathrm {E} = \frac {1}{2} \mathrm {A} ^ {2} + \mathrm {B} ^ {2} $$ $$ \diamond $$ $$ \mathrm {E} = \frac {1}{2} \mathrm {A} ^ {2} + \mathrm {B} ^ {2} $$ $$ \square $$ $$ \mathrm {E} = \mathrm {E} _ {1} + \mathrm {E} _ {2} + \dots + \mathrm {E} _ {n} $$ $$ \square $$ $$ \mathrm {E} = \frac {1}{2} \mathrm {A} ^ {2} + \mathrm {B} ^ {2} $$ $$ \diamond $$ $$ \mathrm {E} = \mathrm {E} _ {1} + \mathrm {E} _ {2} + \dots + \mathrm {E} _ {n} $$ $$ \square $$ $$ \mathrm {E} = \frac {1}{2} \mathrm {A} ^ {2} + \mathrm {B} ^ {2} $$ $$ \diamond $$ $$ \mathrm {E} = \mathrm {E} _ {1} + \mathrm {E} _ {2} + \dots + \mathrm {E} _ {n} $$ $$ \diamond $$ $$ \diamond $$ surviv $$ \mathrm {E} = \frac {1}{2} \mathrm {A} ^ {2} + \mathrm {B} ^ {2} $$ $$ \diamond $$ $$ \mathrm {E} = \frac {1}{2} \mathrm {A} ^ {2} + \mathrm {B} ^ {2} $$ $$ \diamond $$ $$ \mathrm {E} = \frac {1}{2} \mathrm {A} ^ {2} + \mathrm {B} ^ {2} $$ $$ \diamond $$ $$ \square $$ non surviv $$ \mathrm {E} = \mathrm {E} _ {1} + \mathrm {E} _ {2} + \dots + \mathrm {E} _ {n} $$ $$ \diamond $$ $$ \mathrm {E} = \frac {1}{2} \mathrm {A} ^ {2} + \mathrm {B} ^ {2} $$ $$ \diamond $$ t0 t6 t12 t18 t24 t30 t36 t42 t48 Time Figure 5: Serum lactate changes in survivors and non survivors.
Alaa M Atia, et al. Perfusion Index Derived from Pulse Oximetry, Serum Lactate, its Surrogates and Beta Type Natriuretic Peptide (Bnp) for Outcome Prediction in Poly-Traumatized Patients. A Prospective Observational Cohort Study Anaesth Critic Care Med J 2016, 1(1): 000102.
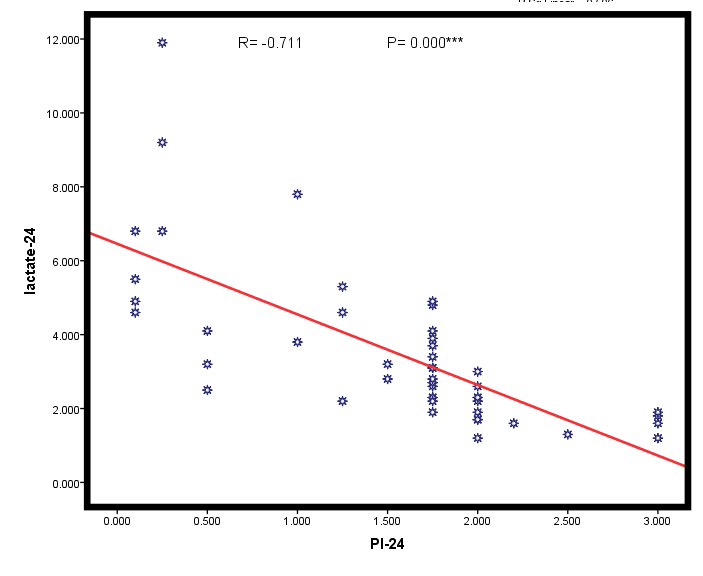
ROC analysis showed the ideal serum lactate cutoff point for predicting mortality ≥ 2.25 mmol/L with AUC 0.57, sensitivity 79% and specificity 69% (Figure 4). Examining the correlation between perfusion index and serum lactate on admission (PI-0& lactate-0) established a statistically nonsignificant correlation, but a statistically significant inverse correlation found at all times after resuscitation (r= - 0.711; P= 0.000) (Figure 6). Lactate clearance: Lactate clearance was significantly lower in non-survivors (0.72±1.89 mmol/L/24h) than survivors (5.03±1.15 mmol/L/24h) (P< 0.001). Patients failed to clear lactic acidosis within 48 hours, post resuscitation; had higher mortality. ROC analysis showed the ideal lactate clearance cutoff point for predicting mortality < 3.0 mmol/L/24 hours with AUC 0.97, sensitivity 97% and specificity 86% (Figure 4).
Base deficit: Base deficit showed statistically significant difference between survivors and non- survivors (P< 0.05) and significantly higher in non- survivors (Figure 7). ROC analysis showed the ideal base deficit cutoff point for predicting mortality > (-8.0) mmol/L with AUC 0.90, sensitivity 91% and specificity 73% (Figure 4).
Copyright© Alaa M Atia, et al.
Base deficit changes in survivors and non survivors t0 t6 t12 t18 t24 t30 t36 t42 t48 $$ \mathrm {E} = \mathrm {E} _ {1} + \mathrm {E} _ {2} + \dots + \mathrm {E} _ {n} $$ $$ \mathrm {E} = \mathrm {E} _ {1} + \mathrm {E} _ {2} + \dots + \mathrm {E} _ {n} $$ $$ \diamond $$ $$ \diamond $$ $$ \mathrm {E} = \mathrm {E} _ {1} + \mathrm {E} _ {2} + \dots + \mathrm {E} _ {n} $$ $$ \diamond $$
0 $$ \mathrm {E} = \frac {1}{2} \mathrm {A} ^ {2} + \mathrm {B} ^ {2} $$
$$ \Delta $$ $$ \mathrm {E} = \mathrm {E} _ {1} + \mathrm {E} _ {2} + \dots + \mathrm {E} _ {n} $$ $$ \diamond $$ $$ \mathrm {E} = \frac {1}{2} \mathrm {A} ^ {2} + \mathrm {B} ^ {2} $$ $$ \diamond $$ -5 Base deficit $$ \diamond $$ surviv $$ \mathrm {E} = \frac {1}{2} \mathrm {A} ^ {2} + \mathrm {B} ^ {2} $$ $$ \diamond $$ $$ \mathrm {E} = \mathrm {E} _ {1} + \mathrm {E} _ {2} + \dots + \mathrm {E} _ {n} $$ $$ \mathrm {E} = \frac {1}{2} \mathrm {A} ^ {2} + \mathrm {B} ^ {2} $$ $$ \mathrm {E} = \frac {1}{2} \mathrm {A} ^ {2} + \mathrm {B} ^ {2} $$ $$ \square $$ $$ \square $$ $$ \square $$ -10 $$ \mathrm {E} = \frac {1}{2} \mathrm {A} ^ {2} + \mathrm {B} ^ {2} $$ $$ \square $$ $$ \square $$ non surviv $$ \mathrm {E} = \mathrm {E} _ {1} + \mathrm {E} _ {2} + \dots + \mathrm {E} _ {n} $$ $$ \square $$ $$ \mathrm {E} = \frac {1}{2} \mathrm {A} ^ {2} + \mathrm {B} ^ {2} $$ $$ \square $$ $$ \mathrm {E} = \mathrm {E} _ {1} + \mathrm {E} _ {2} + \dots + \mathrm {E} _ {n} $$ $$ \diamond $$ -15 $$ \mathrm {E} = \mathrm {E} _ {1} + \mathrm {E} _ {2} + \dots + \mathrm {E} _ {n} $$ $$ \mathrm {E} = \mathrm {E} _ {1} + \mathrm {E} _ {2} + \dots + \mathrm {E} _ {n} $$ $$ \square $$ $$ \square $$ $$ \mathrm {E} = \frac {1}{2} \mathrm {A} ^ {2} + \mathrm {B} ^ {2} $$ $$ \diamond $$ -20 $$ \mathrm {E} = \frac {1}{2} \mathrm {A} ^ {2} + \mathrm {B} ^ {2} $$ $$ \square $$ -25 Time Figure 7: Base deficit changes in survival and non survival group.
BNP study: Studying BNP levels of poly-traumatized
patients with blunt trauma on admission (BNP-0)
revealed mean ±SD (93.4±31.2 pg/ml). Examining the
correlation between admission BNP and mortality
revealed a statistically non significant correlation (r= 0.01
and P= 0.951). Student t. Test revealed a statistically non
significant difference in BNP-0 between survivors and
non-survivors (P> 0.05). Studying BNP levels at 48 hours,
$$ p o s t r e s u s c i t a t i o n (B N P - 4 8) r e v e a l e d m e a n \pm S D $$
(98.5±46.7 pg/ml). Examining the correlation between
BNP-48 and mortality revealed a statistically significant
positive correlation (r= 0.637 and P = 0.000).
Alaa M Atia, et al. Perfusion Index Derived from Pulse Oximetry, Serum Lactate, its Surrogates and Beta Type Natriuretic Peptide (Bnp) for Outcome Prediction in Poly-Traumatized Patients. A Prospective Observational Cohort Study Anaesth Critic Care Med J 2016, 1(1): 000102.
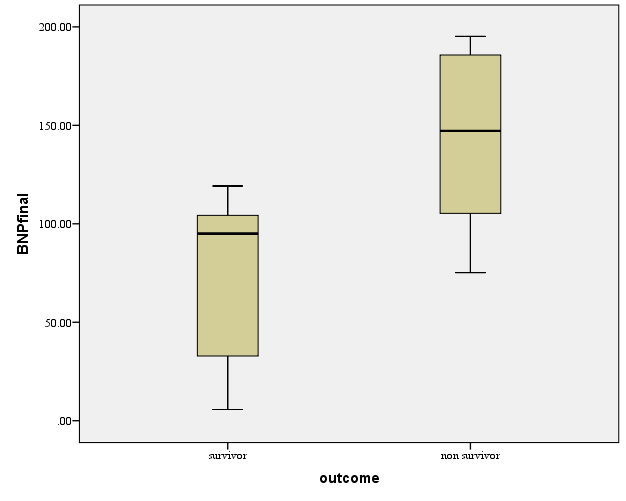
Studying BNP-48 in survivors and non-survivors revealed mean ±SD in survivors (75.7±38.7 pg/ml) and, in non- survivors (144.0±42.4 pg/ml) (Figure 8). Student t. Test revealed a statistically significant difference to study difference in BNP-48 between survivors and non- survivors. Non-survivors had significantly higher beta Natriuretic peptide (BNP) at 48 hours than survivors (p< 0.001). ROC analysis showed the ideal BNP-48 cutoff point for predicting mortality ≥ 95.0 pg/ml with AUC less than 0.5, sensitivity 61% and specificity 32% (Figure 8).
Discussion
The value of routine blood pressure and pulse rate monitoring in patients with hemorrhagic shock as markers of tissue perfusion became questionable. Other monitoring tools have been recently introduced; among them, monitoring of peripheral perfusion during the resuscitation and post resuscitation stages of shock. Peripheral perfusion can be gravely compromised during shock which has been correlated with cardiac output, hyperlactatemia, and organ dysfunction [9]. Many reports showed that traditional vital signs alone are not reliable measures of acute hemorrhage due to compensatory mechanisms. [10, 11, 12] Hernandez and others mentioned that, notwithstanding, no work has assessed the temporal profile of changes in peripheral perfusion during severe shock and resuscitation or has compared the kinetics of development of peripheral perfusion versus traditional metabolic perfusion parameters. This will offer valuable insights about perfusion monitoring in the critically ill patients and help to describe the potential role and limitations of peripheral perfusion as a target for resuscitation [13]. This prospective observational study showed that perfusion index was low on admission, which could be a valuable tool in diagnosing the severity of bleeding, monitoring resuscitation and predicting mortality. Perfusion index showed a statistical significant difference between survivors and non-survivors after 6 hours, post resuscitation. ROC analysis showed the ideal PI cutoff point for predicting mortality ≤ 0.75 with AUC 0.93, sensitivity 97% and specificity 82%. Examining the correlation between perfusion index and serum lactate on admission showed a statistically nonsignificant correlation, but showed a statistically significant inverse correlation at all times after resuscitation. Smetkin and others found PI < 1 is accompanied by other signs of hypo-perfusion in a group of critically ill patients as confirmed by increased lactate and increased Copyright© Alaa M Atia, et al.
venous-end tidal CO2 difference. So, the PI may be used for non-invasive assessment of peripheral blood flow in critical conditions. They determined that in patients who had “decreased” perfusion PI < 1, there was a tendency to inverse correlation between PI and lactate and patients with “normal” perfusion had lower blood lactate than the “decreased” perfusion group [14]. Recently; Huai-Wu and others found PI and Oxygen Challenge Test are predictive of mortality in septic shock patients after resuscitation. They reported the control group had a higher baseline PI than the septic shock group. In the sepsis group, the macro hemodynamic parameters and ScvO2 showed no differences between survivors and non-survivors. The non-survivors had significantly lower PI and higher arterial lactate levels. The PI predicted the ICU mortality with accuracy similar to arterial lactate level. A PI < 0.2 related to poor outcome after resuscitation with area under ROC curve 0.84, sensitivity 55% and specificity 73% [4]. Lima and others proposed a standardized quantitative clinical assessment of peripheral perfusion. An abnormal peripheral perfusion as explained by this approach associated with hyperlactatemia and predicted a worsening SOFA score at 48 hours [15]. In this study, serum lactate was a weak predictor of mortality. Non-survivors had a higher serum lactate level. A cutoff point as traced from the ROC analysis showed a lactate level >2.25 mmol/L in non- survivors (AUC 0.57). A statistically significant positive correlation between lactate and mortality has been also shown. In trauma patients with blood lactate level relative to their vital signs, mortality rate of 28% for patients with mean first lactate (8.33±2.59 mmol/L) or more suggests a high hazard of mortality which could be immediately on arrival to the emergency section. One study found that a cutoff value of 4 mmol/L has a prognostic significance in the emergency department [16]. Compared with our results; recently, a point of care testing depends on venous sample proved comparable to arterial measurement with good correlation in trauma patients. Jansen and others studied capillary or venous lactate levels using a handheld device on arrival at the scene and just before or on arrival at the emergency department. The main outcome tested was in-hospital mortality. They settled that non-survivors had significantly higher lactate levels than survivors. Mortality was significantly higher in patients with lactate levels of 3.5 mmol/L or higher compared with those with lactate levels below 3.5 mmol/L. Likewise, without hypotension, mortality was higher in those with higher lactate levels. Pre-hospital blood lactate levels associated with in- Alaa M Atia, et al. Perfusion Index Derived from Pulse Oximetry, Serum Lactate, its Surrogates and Beta Type Natriuretic Peptide (Bnp) for Outcome Prediction in Poly-Traumatized Patients. A Prospective Observational Cohort Study Anaesth Critic Care Med J 2016, 1(1): 000102.
hospital mortality and provided prognostic information superior to that supplied by the patient's vital signs [17]. Lactate clearance within 48 hours and survival in trauma patients also reported by pal and others in a large scaled study with 5995 trauma patients, comparing the admission lactate value to mortality. They settled that admission serum lactate levels do not predict mortality in the acutely injured patients [18]. MC Nelis and others, in a study of 96 patients reported that mortality significantly increased when lactate clearance is prolonged [19]. In our study, the mortality of patients did not clear lactate within 48 hours post resuscitation was 28%. This is similar to previously reported studies with mortality rate 14-33% [19, 20]. The early assessment of hypovolemic shock, predicting transfusion need and mortality in multi-injured patients are still among the most challenging tasks in the early management of multi-injured patients. In our study, base deficit showed a statistically significant difference between survivors and non- survivors (P< 0.01). Base deficit was significantly higher in non-survivors. ROC analysis showed the ideal base deficit cutoff point for predicting mortality > (-8.0) mmol/L with AUC 0.90. Multiple studies showed that ATLS classification system may not accurately show the degree of hemorrhage in poly-traumatized patients. This system overestimates the degree of tachycardia to hypotension and underestimates mental status. In addition, individual items of the system are poor predictors of bleeding. This contributed to re-interest in base deficit as a predictor of morbidity and mortality. A base deficit oriented classification of hemorrhagic shock has developed. Mutschler and others created a classification system based on base deficit in patients with blunt trauma. Whether this system applies to penetrating injuries is still questionable [21]. Martin and others reviewed all intensive care unit patients with simultaneously got lactate and base deficit measurements. The ability to predict mortality compared alone and in combination. Non-survivors had higher admission lactate and base deficit levels than survivors (both P<0.01), with a modest correlation (r =0. 52) between the measures. The admission lactate and base deficit levels had a similar prediction of mortality with areas under the ROC of 0.7 and 0.66, respectively (both P <0.01). There was no improvement in predictive ability using a combination of the 2 measures [22].
Copyright© Alaa M Atia, et al.
It is to be stated that all these markers (perfusion index, serum lactate, lactate clearance and base deficit) cannot be used at the point of admission to provide the prognostic information about trauma mortality but they might be clinically relevant during the continuing resuscitation. BNP proved to be a prognostic marker in cardiac disease and sepsis [23]. However the prognostic value of BNP in trauma patients remains unclear. The present study displayed elevation of admission serum BNP in all poly-traumatized patients; still high levels got in non-survivors than survivors after 48 hours post trauma. ROC curve analysis showed low sensitivity and specificity of BNP to predict the outcome. The cause of high BNP in trauma patients remains unclear. It may be due to excessive volume resuscitation as described as a marker of fluid overload in transfusion and burn patients [24]. Friese and others reported a higher BNP with resuscitation after injury and levels were higher in patients developed pulmonary edema [25]. Bouras and others settled that no statistically significant difference in BNP levels observed among previously healthy multi- trauma patients (APACHE II score 2-8) with hemorrhagic shock (class II - III) and without head injury. This may show that current IV fluid therapy, at this stage of hemorrhagic shock may be inadequate and further investigation is needed [26]. Our study showed elevated BNP levels in poly-trauma patients without a prognostic value to predict outcome. This study explains for the first time that perfusion index is a sensitive monitor for the diagnosis of the severity of hemorrhagic shock, monitoring resuscitation and a useful prognostic factor of mortality in adult poly- traumatized patients with blunt trauma compared with metabolic parameters. Lactate clearance is a useful prognostic factor and serum lactate is a weak prognostic factor of mortality. BNP has no prognostic value of mortality in this study. Limitations of the survey were the modest number of patients admitted in the study with a short study period which may necessitate a further larger study. As BNP study of this work limited to admission and 48 hours, post resuscitation, it has a limited value in predicting outcome. Serial determinations in further works can be more informative in predicting outcome with BNP in adult poly-traumatized patients with blunt injury.
Alaa M Atia, et al. Perfusion Index Derived from Pulse Oximetry, Serum Lactate, its Surrogates and Beta Type Natriuretic Peptide (Bnp) for Outcome Prediction in Poly-Traumatized Patients. A Prospective Observational Cohort Study Anaesth Critic Care Med J 2016, 1(1): 000102.
Acknowledgments
The authors thank all nurses, residents, and other personnel of the trauma emergency department and the trauma intensive Care for their generous cooperation.
References
-
Qian A, Zhang M, Zhao G (2015) Dynamic detection of N-terminal pro-B-type Natriuretic peptide helps to predict the outcome of patients with major trauma. Eur J Trauma Emerg Surg 41(1): 57-64.
-
Hager H, Reddy D, Kurz A (2003) Perfusion Index - A Valuable Tool to Assess Changes in Peripheral Perfusion Caused by Sevoflurane? Anesthesiology 99: A 593.
-
Lima AP, Beelen P, Bakker J (2002) Use of peripheral perfusion index derived from the pulse oximetry signal as a noninvasive indicator of perfusion. Crit Care Med 30(6): 1210-1213.
-
Huai-Wu He, Da-Wei Liu, Yun Long, Xiao-ting Wang (2013) The peripheral perfusion index and transcutaneous oxygen challenge test are predictive of mortality in septic patients after resuscitation. Crit Care 17(3): R116.
-
American College of Surgeons Committee on Trauma: Advanced Trauma Life Support for Doctors: Instructor Course Manual (2008) 8th edn Chicago, Ill: American College of Surgeons.
-
Champion HR, Sacco WJ, Copes WS, Gann DS, Gennarelli TA, et al. (1989) "A revision of the Trauma Score". J Trauma 29(5): 623–629.
-
Vincent JL, de Mendonça A, Cantraine F, Moreno R, Takala J, et al. (1998) Use of the SOFA score to assess the incidence of organ dysfunction/failure in intensive care units: results of a multicenter, prospective study. Working group on "sepsis-related problems" of the European Society of Intensive Care Medicine. Crit Care Med 26 (11): 1793-1800.
-
SpO2 Monitors with OXISMART® Advanced Signal Processing and Alarm Management Technology: (2008) Pulse Oximetry Note Number 9. Masimo signal extraction technology. Copyright© Alaa M Atia, et al.
-
Howell M, Donnino M, Clardy P, Talmor D, Shapiro N (2007) Occult hypo-perfusion and mortality in patients with suspected infection. Intensive Care Med 33(11): 1892-1899.
-
Wilson M, Davis D, Coimbra R (2003) Diagnosis and monitoring of haemorrhagic shock during the initial resuscitation of multiple trauma patients: a review. J Emerg Med 24(4): 413-422.
-
Vandromme M, Griffin R, Weinberg J, Rue L, Kerby J (2010) Lactate is a better predictor than systolic blood pressure in determining blood requirement and mortality: called pre hospital measures improve trauma triage? J Am Coll Surg 210: 861-869.
-
Guly H, Bouamra O, Spiers M, Dark P, Coats T, Lecky F, et al. (2011) Vital signs and estimated blood loss in patients with major trauma: testing the validity of the ATLS classification of hypovolaemic shock. Resuscitation 82(5): 556-559.
-
Hernandez G, Peña H, Cornejo R, Rovegno M, Retamal J, Navarro J, et al. (2009) Impact of emergency intubation on central venous oxygen saturation in critically ill patients: a multicenter observational study. Critical Care 13(3): R63.
-
Smetkin A, Gaidukov K, Kuzkov V, Kirov M, Bjertnaes L (2010) Assessment of tissue blood flow using peripheral perfusion index. European of Anaesthesiology 27: 47- 55.
-
Lima A, Jansen T, van Bommel J, Ince C, Bakker J (2009) The prognostic value of the subjective assessment of peripheral perfusion in critically ill patients. Crit Care Med 37(3): 934-938.
-
Krishna U, Joshi S, Modh M (2009) An evaluation of serial blood lactate measurement as an early predictor of shock and its outcome in patients of trauma or sepsis. Indian J Crit Care Med 13(2): 66-73.
-
Jansen T, van Bommel J, Baker J (2009) Blood lactate monitoring in critically ill patients: a systematic health technology assessment. Crit Care Med 37(10): 2827-2839.
-
Pal J, Victorino P, Twomey P, Liu T, Bullard K, et al (2006) Admission serum lactate levels do not predict mortality in the acutely injured patient. J Trauma 60(3): 583–587. Alaa M Atia, et al. Perfusion Index Derived from Pulse Oximetry, Serum Lactate, its Surrogates and Beta Type Natriuretic Peptide (Bnp) for Outcome Prediction in Poly-Traumatized Patients. A Prospective Observational Cohort Study Anaesth Critic Care Med J 2016, 1(1): 000102.
-
Mc Nelis J, Marini C, Jurkiewicz A, Szomstein S, Simms H, et al. (2001) Prolonged lactate clearance is associated with increased mortality in the surgical intensive care unit. Am J Surg 182(5): 481–485.
-
Abramson D, Scalea T, Hitchcock R, Trooskin S, Henry S, et al. (1993) Lactate clearance and survival following injury. J Trauma 35 (4): 584–588.
-
Mutschler M, Nienaber U, Brockamp T, Wafaisade A, Fabian T, Paffrath T, et al. (2013) Renaissance of base deficit for the initial assessment of trauma patients: a base deficit-based classification for hypovolemic shock developed on data from16, 305 patients derived from the Trauma Register DGU®. Critical Care 17(2): R42.
-
Martin M, Fitz Sullivan E, Salim A, Brown C, Demetriades D, Long W (2006) Discordance between lactate and base deficit in the surgical intensive care unit: which one do you trust? Am J Surg 191 (5): 625- 630.
-
Rudiger A, Gasser S, Fischler M (2006) Comparable increase of B-type Natriuretic peptide and amino- terminal pro-B-type Natriuretic peptide levels in patients with severe sepsis, septic shock, and acute heart failure. Crit Care Med 34(80): 2140–2144.
-
Tobian A, Sokoll L, Tisch D, Ness P and Shan H (2008) N-terminal pro-brain Natriuretic peptide is a useful diagnostic marker for transfusion-associated circulatory overload. Transfusion 48(6): 1143-1150.
-
Friese R, Dineen S, Jennings A, Pruitt J, McBride R, Shafi S, et al. (2007) Serum B-Type Natriuretic Peptide: a Marker of Fluid Resuscitation After Injury? J Trauma 62(6): 1346-1351.
-
Bouras P, Rogdakis A, El-Fellach N, Karampas B, Liakos G, (2011) Plasma B-Type Natriuretic Peptide (BNP) Variation in Multi-Trauma Patients: Prospective Clinical Study. Hellenic Journal of Surgery 83: 4. Copyright© Alaa M Atia, et al.
- Editorial on Multimodal Analgesia
- Surgical Incision Site Local Anaesthetic Infiltration and Superior Hypogastric Plexus Block in Total Abdominal Hysterectomy Under General Anaesthesia- A Placebo-Controlled, Randomized Clinical Trial
- Supraglottic Airway Insertion in Semi Fowler Position Due to Severe Thoracic Hyperkyphosis: A Case Report
- Anaesthetic Management of Cardiac Myxoma Patient with Systemic Involvement: A Case Report
- Current Problems in Pulmonary Respiratory Distress Syndrome (Literature Review)
- Evolution of Perioperative Hemodynamic Monitoring from the Hand on Pulse to Hypotension Prediction Index