Utility of Advanced Airway Assessment in the Awake Patient: Case Series
The assessment and management of the difficult airway represents one of the primary topics addressed in anesthesiology. A number of recommendations regarding airway management have been issued by various associations. Awake intubation has been described as a viable option among patients with a predicted difficult airway, with possibilities for its achievement that include the use of fiber optics, for which experience is required. The use of the videolaryngoscope is another reported technique, which similarly requires a learning curve. In reported studies, the probability of failure is similar between both devices, despite the causes of failure differing from each other. Airway evaluation includes both clinical assessment and the support of imaging studies, such as tomography, magnetic resonance or ultrasound. Successful awake intubation is highly dependent on patient communication and adequate upper airway preparation. The following article describes four case reports outlining the management of awake intubation and emphasizing the importance of teaching tools for the improvement of the awake intubation technique.
Introduction
Airway assessment and management represents one of the major implications among patients undergoing any anesthetic or emergency procedure, due to the consequences on patient’s morbidity and mortality.
These complications derive both from the difficulty in maintaining patency of the airway, as well as from its instrumentation (intubation), reason for which an appropriate and safe evaluation is by means of adequate preparation and topicalization of the airway, therefore enabling a proper review of the patient during spontaneous ventilation, which in turn facilitates crucial decision-making without risking the patient’s life.
Awake intubation or awake airway assessment is a recommended technique for airway management in patients with a known difficult airway, or in those in whom intubation is indicated prior to anesthetic induction [1]. A strategy for difficult airway management is necessary when facemask ventilation or placement of an advanced airway device is expected or is likely to be compromised by the patient’s condition [2].
Patients presenting with neck pathology caused by tumors, previous surgery, obstructive lesions or radiotherapy are at increased risk of failed facemask ventilation, direct laryngoscopy, videolaryngoscopy and a higher possibility of undergoing surgical airway [3]. Indications for awake intubation include: anticipated or known difficult airway, cervical spine conditions, lesions occupying space in the mouth or neck, body mass index (BMI) > 35 kg/m2, poor dental status, polyarthritis, avoidance of neuromuscular blocking drugs, induction in patients with high cardiac risk, bowel obstruction with high risk of bronchoaspiration, and training purposes [4]. Considering the nature of the pathology in these patients, ensuring that asleep airway management is safe prior to induction of anesthesia and, otherwise, choosing awake tracheal intubation, appears advisable [3].
The challenges encountered by most physicians when learning the technique of awake fibreoptic intubation (AFOI) should be fully recognized [5, 6]. The introduction of awake videolaryngoscopy could further reduce exposure to AFOI [7]. The 4th National Audit Project (NAP4) reported on the low utilization of awake fiberoptic intubation (AFOI) in the management of difficult airways, with possible contributing factors that include lack of experience and familiarity [8]. To date, both techniques show a fairly similar success rate, though consideration on the operator’s ability remains of the utmost importance [9]. While flexible bronchoscopy (FB) and video laryngoscopy (VL) with a brief mention of awake tracheal intubation via a supraglottic or lighted stylet-guided airway are the two main available techniques for performing awake tracheal intubation, it’s important to consider all known and available intubation techniques that can be performed in an awake patient [3].
Availability and use of VLs is increasing. Studies involving both inexperienced and experienced anesthesiologists have suggested that becoming proficient with a particular VL requires approximately 20 uses [10]. In a comparative study on awake fiberoptic-guided nasotracheal intubation and video laryngoscopy, Kramer and colleagues observed that both techniques had a 4% failure rate, although the underlying reasons varied between each approach. Failure in the videolaryngoscope group was attributed to the persistence of the gag reflex, even after topicalization with a local anesthetic agent [11]. Not to be forgotten are the guidelines set by the Difficult Airway Society for the management of the unexpected difficult airway and the American Society of Anesthesiologists’ algorithm on difficult airway, suggesting intubation through a supraglottic device in the event of failed tracheal intubation. Insertion of a supraglottic device in the awake patient under topical anesthesia, followed by tracheal intubation after induction of general anesthesia, has been previously reported [12, 13].
Imaging Assessment of the Airway
Airway assessment and the prediction of a difficult airway is the most important step in emergency airway management. Failure to recognize a difficult airway can lead to life-threatening complications, such as brain damage and death [14]. Three-dimensional reconstruction technique using computed tomography provides orientation in difficult tracheal intubation, as it enables the identification of deviations, such as adjacent structures, that could hinder tracheal intubation [15, 16]. Ultrasound provides high- resolution images of the upper airway anatomy, comparable to those obtained through computed tomography and magnetic resonance imaging. It can be a useful adjunct for predicting a difficult laryngoscopy [14]. The use of ultrasound imaging has been successfully employed for the identification of difficult airway predictors, which include temporomandibular joint mobility and tongue thickness, among others. Nevertheless, a difficult airway correlates with the entire anatomy of the upper airway structure, in which case a single indicator results insufficient in reflecting the functionality of the upper airway and fails to accurately predict the difficult airway. The more predictors that are studied, the lower the risk of encountering a difficult airway [17].
Topicalization
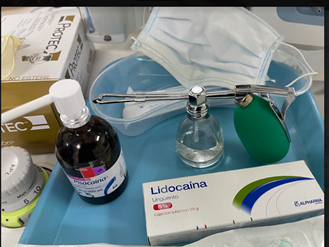
A successful awake intubation relies heavily on adequate upper airway preparation, emphasizing topicalization and appropriate analgesia. Lidocaine provides a more favorable systemic and cardiovascular toxicity risk profile, thereby becoming a preferable choice over bupivacaine or ropivacaine. Clinical levels of toxicity have been demonstrated with lidocaine doses greater than 6.0-9.3 mg/kg of lean body weight. The total dose of local anesthetics, including regional anesthesia and surgical infiltration, should be considered [18]. Traditional devices for topical pharyngeal anesthesia, such as the laryngotracheal topical anesthesia kit (Figure 1), are widely available, but their effectiveness is not necessarily ideal. Additional methods, such as nebulization and spray- as-you-go techniques, provide satisfactory conditions for awake intubation [19].
Sedation Levels
The American Society of Anesthesiologists has defined the different levels of sedation/analgesia as a continuum, ranging from “minimal (anxiolysis)” to “moderate/analgesia” (conscious sedation) and “deep sedation/analgesia”. The deepest level of this continuum is general anesthesia [1]. AFOI typically requires adequate sedation, patient cooperation and preserved spontaneous breathing. Drugs suitable for AFOI sedation include opioids, benzodiazepines (midazolam), propofol and dexmedetomidine [20]. The use of either remifentanil or dexmedetomidine is recommended, as both have been proven to have a higher level of patient satisfaction and a lower risk of excessive sedation and airway obstruction as compared to other drugs [21, 22]. Although Remifentanil is an extremely potent opioid, it is not considered a sedative as it acts as a poor hypnotic in clinically relevant concentrations, with a minimal effect on cognitive function. Therefore, caution when using this medication is advised [23].
Clinical Case 1
59-year-old male patient presenting with a 2-year clinical picture of dysphonia, with increasing dysphonia over the last few weeks, denying dyspnea or other respiratory symptoms. It should be noted that he has a diagnosis of moderately differentiated squamous cell carcinoma with tumoral ulceration in the right hemilarynx, undergoing 35 sessions of radiotherapy. Previous medical history includes appendectomy, vasectomy, and uncomplicated pulmonary thromboembolism in treatment with Rivaroxaban (suspended 2 days before the current procedure). On this occasion, the patient was admitted for laryngosuspension with biopsy. Upon airway examination, no presence of Mallampati II, thyromental distance I, interincisor distance I, with no evidence of total airway obstruction. Vital signs were SpO2: 88%, BP: 110/70mmhg, HR: 79 beats per minute, RR: 20 breaths per minute, weight: 87kg, height: 1.78mts. Balanced general anesthesia with awake airway assessment was selected as anesthetic management. Patient was admitted to the preoperative area, where airway topicalization began. It’s decided to administer micronebulization with lidocaine 60mg in 10ml, aerosolization of the oral cavity with 2% lidocaine 60mg (Figure 2), along with the use of lidocaine 5% ointment in the nasal cavity. Stimulation tests with tongue depressors were performed after 5 minutes of topicalization. The patient was considered tolerant and was taken into the operating room. Intravenous ketamine (10mg) and fentanyl (50mcg) were administered under non-invasive monitoring. Ultrasonographic tracing of the cricothyroid membrane was performed and labeled for emergency management in case of airway collapse. Prior to introducing the C-MAC hyper-curved blade videolaryngoscope, the patient received information regarding the procedure. The videolaryngoscopy was then gently performed. Upon observing 100% POGO (percentage of glottic opening) (Figure 4), videolaryngoscopy was withdrawn as a safety measure, and a standard anesthetic induction was performed, providing a higher range of safety for patient intubation, which was carried out without incident.

Months later, the patient was admitted to the hospital emergency room presenting with dyspnea on minimal exertion, as well as signs of respiratory distress. An awake nasofibroscopy was performed, showing reduced mobility of both vocal cords (Figure 3). Thus, it’s decided to enter the operating room to perform an awake tracheostomy, considering regulations and the risk of collapse during induction. The risks were discussed with the patient, deciding to proceed with an awake tracheostomy. The patient was brought into the operating room, receiving micronebulized lidocaine 80mg, intravenous ketamine 5mg, and intravenous fentanyl 50mcg, with facemask at 6 liters per minute and spontaneous ventilation. Lidocaine with epinephrine was applied over the surgical site before tracheal incision, followed by transtracheal administration of 40 mg of 2% lidocaine. Tracheostomy tube was then successfully placed without incident.

Clinical Case 2
59-year-old female patient with diagnosis of moderately differentiated infiltrating squamous cell carcinoma on the right mandible, scheduled for right mandibulectomy plus radical neck dissection. She presented with clinical picture one year ago, subsequently undergoing a resection of a lesion on the right mandible. She later presented an increase in size, resulting in a lesion measuring 2.9 cm x 1.5 cm with the addition of 5 right cervical lymph nodes and bone infiltration. Previous medical history includes rhinoplasty and an uncomplicated right shoulder arthroscopy, allergy to diclofenac, and absence of dyspnea or ventilatory mechanics alterations. Upon physical examination, the patient appeared to be older than her chronological age; airway examination revealed Mallampati class II airway, thyromental distance class I, interincisor distance class III, Bell House score class I, no other apparent clinical alterations. The patient was informed on the risks of airway management, and the decision to perform awake airway exploration was made. Upon admission to the preoperative area, airway topicalization began, administering micronebulization with lidocaine 50mg in 10ml, aerosolization of the oral cavity with 2% lidocaine 60mg, and the use of lidocaine 5% ointment in the nasal cavity. Stimulation tests with tongue depressors were performed after 5 minutes of topicalization. The patient was considered tolerant and was taken into the operating room. 15 mg of intravenous ketamine and 50 mcg of fentanyl were administered under non-invasive monitoring. Ultrasonographic tracing of the cricothyroid membrane was performed and labeled for emergency management in case of airway collapse. Prior to introducing the C-MAC hyper-curved blade videolaryngoscope, the patient received information regarding the procedure. The videolaryngoscopy was then gently performed. Upon observing 90% POGO (Figure 4), videolaryngoscopy was withdrawn as a safety measure, and a standard anesthetic induction was performed, providing a higher range of safety for patient intubation. Nasotracheal intubation assisted by videolaryngoscopy was performed without any incidents.

Clinical Case 3
40-year-old female patient with diagnosis of bilateral peritonsillar abscess, presenting with increased volume in the oropharynx, fever and general malaise 7 days after dental intervention, in addition to dyspnea on exertion one day before admission. Antibiotic treatment was initiated, and a CT scan was performed revealing 2 peritonsillar abscesses, the left one measuring 2.1x1.5cm and the right one 2x1.8cm, for which reasons the patient was admitted for surgical drainage of the abscesses under anesthesia. Patient denied any chronic degenerative diseases or allergies. Past medical history includes a closed reduction of the left wrist under anesthesia, referring having experienced nausea and vomiting postoperatively with poor tolerance to opioid usage. Upon physical examination, the patient appeared to be younger than her chronological age, with a weight of 130kg and a height of 1.69 meters. Vital signs were HR: 90 beats per minute, RR: 18 breaths per minute, BP: 135/75mmHg, and SpO2:90%. Airway examination showed Mallampati grade III, thyromental distance grade II, interincisor distance grade II, and Bell House score grade II. Given the airway risks, the decision to perform awake airway assessment with possible awake intubation was made, after explaining the risks of said procedure to the patient. Topicalization of the airway was initiated using nebulized lidocaine 80mg in 10ml, (Figure 3) aerosolization of the oral cavity with 2% lidocaine 100mg, and lidocaine 5% spray in the nasal cavity. Stimulation tests with tongue depressors were performed after 5 minutes of topicalization. The patient was considered tolerant and was taken into the operating room, receiving both a dexmedetomidine infusion at a rate of 0.2mcg/kg/ hr and a remifentanil infusion at a rate of 0.06mcg/kg/ min under non-invasive monitoring. Ultrasonographic tracing of the cricothyroid membrane was performed and labeled for emergency management in case of airway collapse. Prior to introducing the Onfocus hyper-curved blade videolaryngoscope, the patient received information regarding the procedure. The videolaryngoscopy was then gently performed. Upon observing 90% POGO with a slight difficulty when introducing the videolaryngoscope, the airway was secured through endotracheal intubation (Figure 4). Thereafter, the anesthetic induction was completed with propofol 120mg and rocuronium 50mg, achieving a successful intubation with no risk to the patient.
Clinical Case 4
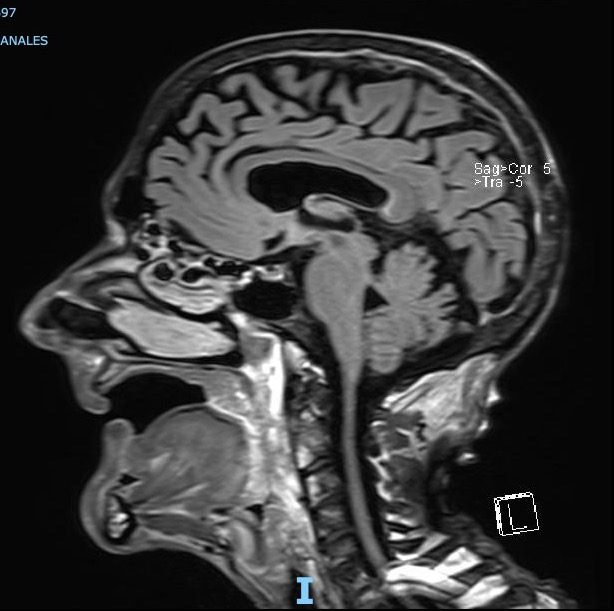
64-year-old male patient with a 1 year and 6-month history of laryngeal carcinoma, in treatment with chemotherapy and radiotherapy. For the past 9 months, he’s presented a 14 kg weight loss, in addition to dysphagia and cyanotic dyspnea. Upon physical examination, the patient appeared older than his chronological age, cachectic, with evident weight loss, tachypneic (27rpm), cyanotic, tachycardic (115lpm), with conventional nasal cannulas at 3lt/min reaching a baseline saturation of 84%, dyspnea on minimal exertion; upon airway-directed examination, findings included Mallampati score of 1, Patil-Aldrete score of 1, cylindrical neck with increased volume on the right side, measuring approximately 3x2cm upon palpation with associated displacement of trachea (further confirmed on magnetic resonance imaging – (Figure 5), intercostal retractions observed on the chest and evident signs of increased ventilatory effort. Given the patient’s clinical condition and the risk of airway obstruction, a decision was made to perform an awake tracheostomy. Once the patient was admitted into the operating room with non-invasive monitoring, 10mg of ketamine and 25mcg of fentanyl were administered, along with facemask ventilation at 10 lt/min achieving a saturation of 96%. The surgical site, previously marked using ultrasound assistance, was then infiltrated with local anesthetic (lidocaine with epinephrine). 2ml of simple transtracheal lidocaine was administered, the trachea was incised, and a #6.5 non-fenestrated tracheostomy tube was inserted after the first attempt without incident. The cuff was inflated and connected to mechanical ventilation, obtaining ETCO2: 65mmHg; arterial blood gas revealed pH: 7.09, pCO2: 89.2mmHg, pO2: 101, p50: 34.7, Lac: 0.7, glucose: 152. Based on the results shown, an evident respiratory acidosis was identified, for which reason the patient was transferred to the intensive care unit for further mechanical ventilation management and assessment of ventilatory parameters, achieving improvement in the 24 hours following management.
Discussion
Ensuring a patent airway remains a fundamental focus within clinical anesthesia, as failure to secure an airway in anesthetized patients can result in serious outcomes in a matter of minutes [24]. According to the American Society of Anesthesiologists’ analysis regarding closed claims, one of the leading causes of anesthesia-related patient injury is the failure to intubate the trachea and secure the airway. Consequently, 85% of said injuries result in death or brain damage [24].
Awake intubation remains an acceptable experience for most patients, although others find it to be painful and frightening. The application of local anesthetic can cause discomfort, coughing and a sense of suffocation, thus making communication with the patient an essential component for the successful performance of this procedure [25].
Teaching tools available nowadays can undoubtedly improve awake intubation techniques, thereby making them both more efficient and more precise [26].
Conclusion
Day by day, we encounter situations that endanger the patient’s integrity, which makes our work as anesthesiologists extremely valuable when making the best decision for the patient. Choosing awake intubation or assessment of the airway should be seen in a positive light, without fear of talking to the patient and explaining the procedure to be performed, as well as the benefits of taking such an approach. Advanced airway assessment should constitute a standard part of our practice, as it allows for the identification of risks in our procedures. However, we should never forget that the combination of assessments and studies performed will provide a better understanding of the situation we are facing. We should always make use of devices or images that provide a better overview, such as airway ultrasound, computed tomography or magnetic resonance imaging.
Difficult airways will invariably represent a challenge for any anesthesiologist; however, we are preparing ourselves every day to approach them in safer ways.
References
-
Heidegger TM (2017) “Awake” or “Sedated”: Safe Flexible Bronchoscopic Intubation of the Difficult Airway. Anesthesia Analgesia 124(3): 996-997.
-
Ahmad I, El-Boghdadly K, Bhagrath R, Hodzovic I, McNarry AF, et al. (2020) Difficult Airway Society guidelines for awake tracheal intubation (ATI) in adults. Anaesthesia 75(4): 509-528.
-
Kristensen MS, Aziz MF (2020) From variance to guidance for awake tracheal intubation. Anaesthesia 75(4): 442-446.
-
Wong P, Lim WY (2019) Awake supraglottic airway guided flexible bronchoscopic intubation in patients with anticipated difficult airways: a case series and narrative review. Korean J Anesthesiol 72(6): 548-557.
-
Ince M, Jackson M, Plummer N, Simmons H, Talbot L, et al. (2016) Awake fibreoptic intubation, videolaryngoscopy and training. Anaesthesia 71(11): 1369-1381.
-
Murphy T, Howes B (2017) Current practice for awake fibreoptic intubation - some unanswered questions. Anaesthesia 72(6): 675-685.
-
Mendonca C, Mesbah A, Velayudhan A, Danha R (2016) A randomised clinical trial comparing the flexible fibrescope and the Pentax Airway Scope (AWS) for awake oral tracheal intubation. Anaesthesia 71(8): 908-1014.
-
Chong MSF, Oti C (2018) Experience in awake fibreoptic intubation. Anaesthesia 73(12): 1568-1579.
-
Alhomary M, Ramadan E, Curran E, Walsh SR (2018) Videolaryngoscopy vs. fibreoptic bronchoscopy for awake tracheal intubation: a systematic review and meta-analysis. Anaesthesia 73(9): 1151-1161.
-
Ahmad I, Bailey CR (2016) Time to abandon awake fibreoptic intubation. Anaesthesia 71(1): 12-16.
-
Kramer A, Müller D, Pförtner R, Mohr C, Groeben H, et al. (2015) Fibreoptic vs videolaryngoscopic (C-MAC- D-BLADE) nasal awake intubation under local anaesthesia. Anaesthesia 70(4): 400-406.
-
Bhalotra AR (2020) Awake supraglottic airway guided flexible bronchoscopic intubation. Korean J Anesthesiol 73(2): 173-174.
-
Sahay N, Kumer R, Naaz S, anand V (2020) Awake supraglottic airway guided intubation: for the patient, by the patient. Korean J Anesthesiol 73(3): 262-263.
-
Adi O, Fong CP, Sum KM, Ahmad AH (2021) Usage of airway ultrasound as an assessment and prediction tool of a difficult airway management. Am J Emerg Med 42: 263e1-263e4.
-
Hong H, Qian YT, Fu L, Wang W, Li CH, et al. (2019) Study on the use of CT three-dimensional reconstruction technique for guiding tracheal intubation with rigid fiber bronchoscope in difficult airway. Beijing Da Xue Xue Bao Yi Xue Ban 51(5): 870-874.
-
Ingelmo PM, Parini R, Grimaldi M, Mauri F, Romagnoli M, et al. (2011) Multidetector computed tomography (MDCT) for preoperative airway assessment in children with mucopolysaccharidoses. Minerva Anestesiol 77(8): 774-780.
-
Wang B, Yao W, Xue Q, Wang M, Xu J, et al. (2022) Nomograms for predicting difcult airway based on ultrasound assessment. BMC Anesthesiology 22: 23.
-
Kostyk P, Francois K, Salik I (2021) Airway Anesthesia for Awake Tracheal Intubation: A Review of the Literature. Cureus 13(7): e16315.
-
Xue Li, Hai-yang Yu, Xiao Hu (2022) A converted spray device for topical pharyngeal anesthesia in awake intubation. Braz J Anesthesiol 72(2): 309-310.
-
Ma Y, Cao X, Zhang H, Ge S (2020) Awake fiberoptic orotracheal intubation: a protocol feasibility study. J Int Med Res 49(1): 1-10.
-
El-Boghdadly K, Ahmad I (2020) Sedation strategies in awake tracheal intubation: a reply. Anaesthesia 75(5): 689-690.
-
Johnston KD, Rai MR (2013) Conscious sedation for awake fibreoptic intubation: a review of the literatura. J Can Anesth 60(6): 584-599.
-
Irwin MG (2020) Difficult Airway Society guidelines for awake tracheal intubation in adults. Anaesthesia 75(5): 686-698.
-
Xue FS, Liu QJ (2018) Tracheal Intubation Awake or Under Anesthesia for Potential Difficult Airway: Look Before You Leap. Chin Med J 131(6): 753-756.
-
Knudsen K, Nilsson U, Högman M, Pöder U (2016) Awake intubation creates feelings of being in a vulnerable situation but cared for in safe hands: a qualitative study. BMC Anesthesiology 16: 71.
-
Weigel WA, Lyons AB, Liberman JS, Blackmore C (2021) Using Lean tools to improve the efficiency of awake fibreoptic intubation setup. BMJ Open Quality 10(4): e001432.
- Editorial on Multimodal Analgesia
- Surgical Incision Site Local Anaesthetic Infiltration and Superior Hypogastric Plexus Block in Total Abdominal Hysterectomy Under General Anaesthesia- A Placebo-Controlled, Randomized Clinical Trial
- Supraglottic Airway Insertion in Semi Fowler Position Due to Severe Thoracic Hyperkyphosis: A Case Report
- Anaesthetic Management of Cardiac Myxoma Patient with Systemic Involvement: A Case Report
- Current Problems in Pulmonary Respiratory Distress Syndrome (Literature Review)
- Evolution of Perioperative Hemodynamic Monitoring from the Hand on Pulse to Hypotension Prediction Index