SGLT2 Inhibitors and Perioperative Euglycemic Diabetic Ketoacidosis
Sodium-glucose cotransporter 2 (SGLT2) inhibitors are a new class of diabetes medications that act at the level of the kidney to increase renal glucose clearance. The resultant hypoglycemia suppresses insulin secretion and stimulates glucagon, lipolysis, and ketogenesis, which creates a state of starvation. Since SGLT2 inhibitors also decrease sodium reabsorption, patients are at risk for dehydration. An unusual side effect of this drug class is the development of euglycemic diabetic ketoacidosis (eDKA). A case report describes a patient taking Synjardy® (empagliflozin/metformin) who underwent laparoscopic cholecystectomy and developed perioperative eDKA. It is critical to maintain a high index of suspicion to recognize eDKA and institute immediate therapy tenants of intravenous fluid hydration, insulin infusion, and aggressive electrolyte repletion.
Introduction
Sodium-glucose cotransporter 2 (SGLT2) inhibitors are a new class of drugs approved by the U.S. Food and Drug Administration (FDA) for use in type two diabetes (T2DM). SGLT2 inhibitors work via several mechanisms: decreasing glucose reabsorption in the proximal convoluted tubules, thus increasing glycosuria with reduced plasma glucose; improving insulin sensitivity; and promoting pancreatic β-cell function1. These drugs are favored in some patients because of their lower hypoglycemic risk compared to other alternatives; however, the drug class’s side effect profile includes euglycemic diabetic ketoacidosis (eDKA), which is precipitated by states of starvation, hypovolemia, illness, or stress. Perioperative patients taking SGLT2 inhibitors often encounter periods of starvation, nil per os, and dehydration. Thus, careful perioperative management of patients on SGLT2 inhibitors is crucial to prevent life-threatening consequences. Herein, we describe a case of a patient on empagliflozin/ metformin (Synjardy®) with post-operative eDKA and multiorgan dysfunction after a laparoscopic cholecystectomy and endoscopic retrograde cholangiopancreatography (ERCP). Subsequent discussion includes evaluation of the class of SGLT2 inhibitors, pathophysiology of diabetic ketoacidosis (DKA), identification and management of eDKA.
Case Presentation
Our patient is a sixty-nine-year-old female with a past medical history of dementia, overactive bladder, and non-insulin-dependent T2DM managed with Synjardy® (empagliflozin/metformin). She was admitted with choledocholithiasis associated with mild pancreatitis. Initial medical management included fluid resuscitation, bowel rest followed by advancement to clear liquid diet, glycemic control with sliding scale insulin, and intravenous antibiotic Zosyn® (piperacillin tazobactam). On hospital day #2, she underwent a laparoscopic cholecystectomy with a positive intraoperative cholangiogram. The following day, ERCP with biliary sphincterotomy was performed, and her common bile duct was successfully cleared of retained gallstones. Post- procedure, she was advanced to a regular diet, which she tolerated but experienced a mild post-operative ileus.
On post-operative day (POD) #3, the patient was seen early in the morning, had no complaints, and her mental status was noted to be at baseline in the setting of mild dementia. A review of vital signs found her to be afebrile, mildly tachycardic, and hypertensive. Labs revealed increasing leukocytosis of 20 x10^3/µL, acute hypernatremia of 153 mmol/L, hyperchloremia of 121 mmol/L, hypokalemia 3.1 mmol/L, low bicarbonate of 6 mmol/L, and blood glucose within normal range from 137- 186 mg/dL. Later that morning, her clinical status acutely decompensated. On reassessment, she was found to be confused, diaphoretic, tachypneic, and she was reporting angina. She was immediately transferred to the intensive care unit (ICU) with additional labs revealing a high anion gap metabolic acidosis with pH of 6.9 and base deficit of 28 mEq/L, β-hydroxybutyrate >9 mmol/L, high plasma osmolality 342 mOsm/kg, and an elevated troponin of 2.2 ng/mL.
The patient was diagnosed with high anion-gap eDKA. She was started on an insulin infusion with fluid hydration, aggressive potassium repletion, and bicarbonate boluses to help correct the acidosis. Additional diagnoses included the following: metabolic encephalopathy; mixed shock requiring norepinephrine support; type II myocardial infarction requiring initiation of acute coronary syndrome protocol with heparin infusion; acute systolic heart failure with reduced ejection fraction to 30-35%; compensatory acute respiratory failure requiring emergent intubation; and pre- renal acute kidney injury. Empiric antibiotics of vancomycin and meropenem were started as the differential diagnosis for decompensation included cholangitis with recent biliary tree instrumentation; however, her blood cultures remained negative. Her clinical status improved over the next few days, and she was transitioned from an insulin drip to long-acting insulin. On POD #5, her ileus resolved, and she was started on Glucerna tube feeds. She was discharged to home on POD #8 with a regimen of metformin 1000 mg twice daily.
SGLT2 Inhibitors
SGLT is a transmembrane protein that co-transports sodium and glucose across the cell membrane for reabsorption. Specifically, SGLT2 is the isoform that is located on the apical cells of the proximal convoluted tubules (PCTs) in the kidneys [1]. The SGLT2 is responsible for 90% of glucose reabsorption in normoglycemic conditions [2]. In diabetic patients, hyperglycemia induces glomerular hyperfiltration, which results in the overall growth and hypertrophy of the PCTs with increased expression of SGLT2 [3, 4].
The drug class’s mechanism of action inhibits the SGLT2, thereby decreasing glucose reabsorption in the PCTs and increasing glucose excretion in the urine (Figure 1). Glycosuria induces osmotic diuresis, decreasing extracellular volume and thus diastolic blood pressure [5]. Furthermore, the decreased plasma glucose concentration results in increased insulin sensitivity and β-cell function [1]. The insulin-independent mechanism of SGLT2 inhibitors is favorable with a lower risk of hypoglycemia. The drug class also has cardiorenal protective effects. Pharmacokinetics of the SGLT2 inhibitors include rapid oral absorption, extensive hepatic metabolism, and long half-lives [2]. The average half- life ranges from 11-13 hours, with peak effect at 1.5 hours after administration [2]. Primary distribution is within the kidneys, with smaller amounts found in hepatic, gastric, and enteric tissues [2].
SGLT2 inhibitors can be identified by their suffix of “-gliflozin”. Currently, the FDA has approved four types of SGLT2 inhibitors for use in T2DM: canagliflozin, dapagliflozin, empagliflozin, and ertugliflozin [6]. In 2018, the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD) provided recommendations regarding the use of SGLT2 inhibitors in the management of T2DM. SGLT2 inhibitors are recommended as a second-line therapy for T2DM patients at high risk for cardiovascular disorders including coronary artery atherosclerosis and heart failure, those with a risk of chronic kidney disease, and cases where weight loss is necessary [7].
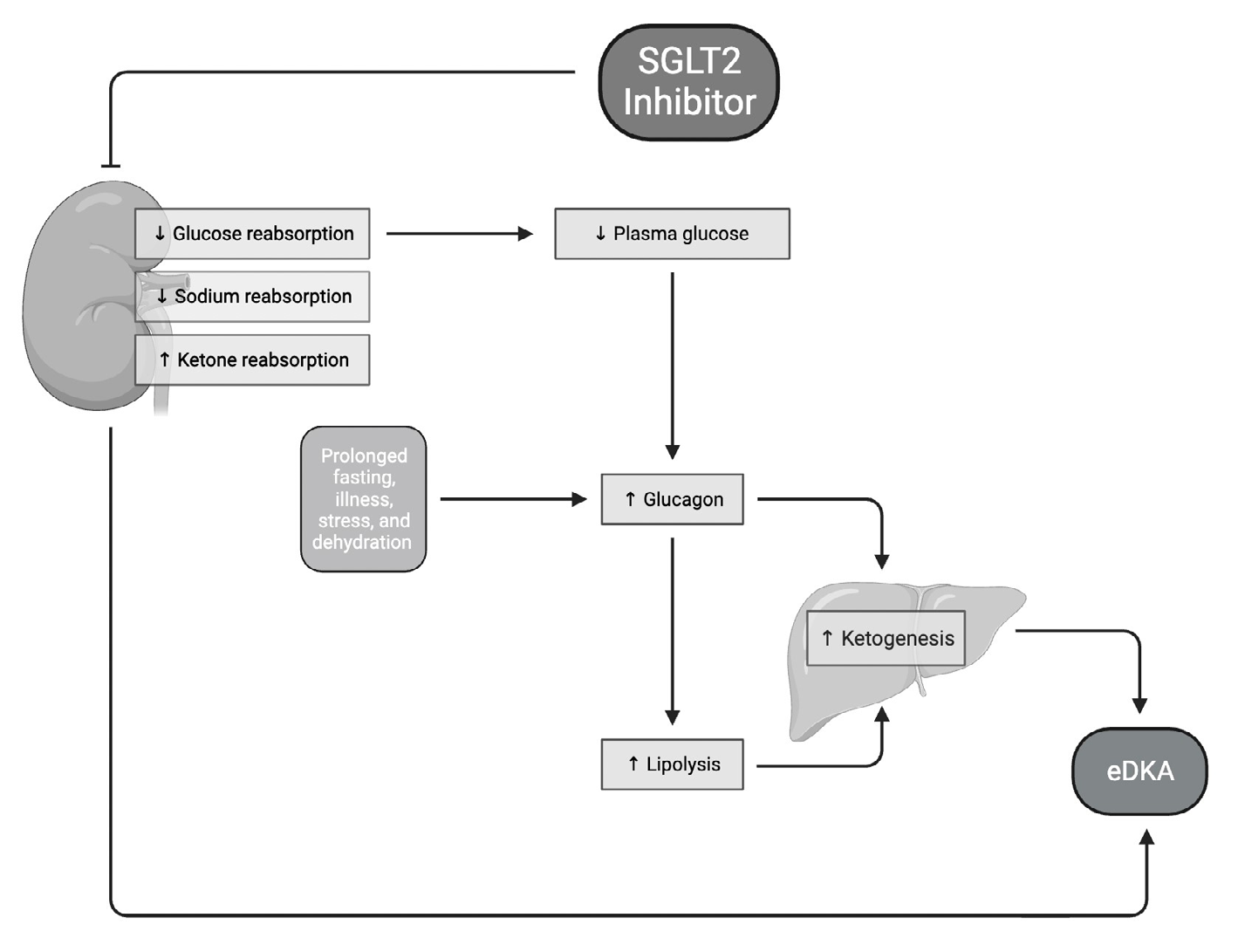
SGLT2 sodium-glucose cotransporter 2; eDKA euglycemic diabetic ketoacidosis. Figure 1: Mechanism of SLGT2 Inhibitor.
One of the most concerning adverse effects of SGLT2 inhibitors is eDKA; however, there is limited research available to explain why eDKA occurs [8]. Increased renal clearance of glucose results in reduced insulin, increased counter-regulatory hormone glucagon, and insulin sensitivity [9]. Hepatic lipolysis and ketogenesis are up regulated. β-oxidation of fatty acids generates acetyl-CoA that is converted to ketone bodies via ketogenesis. Also, renal reabsorption of ketones is increased, which worsens ketonemia and metabolic acidosis through indirect bicarbonate losses [10]. Fluid loss is inherent to the mechanism of SGLT2 inhibitors since water follows sodium that is lost in the urine, worsening the hypovolemic state of DKA [8]. Thus, SGLT2 inhibitors create favorable conditions for the development of eDKA.
Diabetic Ketoacidosis (DKA)
DKA is a life-threatening diabetic complication that is more prevalent among type I diabetics than type II [11]. The National Institutes of Health (NIH) defines DKA as a state of relative or absolute insulin deficiency worsened by hyperglycemia, dehydration, and acidosis brought on by the onset of diabetes, lack of medication compliance, infection, or trauma [11]. In non-diabetics, increased serum glucose stimulates pancreatic β-cells to produce and secrete insulin while inhibiting hepatic gluconeogenesis and glycogenolysis. In patients with low to absent serum insulin, these pathways are upregulated secondary to insulin resistance.
Insulin deficiency leads to a state of energy starvation in cells. Counter-regulatory hormones such as glucagon are released, further elevating serum glucose by activating gluconeogenesis, glycogenolysis, and lipolysis to meet the body’s metabolic demands. This results in increased levels of serum free fatty acids that are oxidized via β-oxidation in hepatocytes, producing β-hydroxybutyrate and acetoacetate [11]. Patients in DKA have ketonemia, high anion gap metabolic acidosis (pH <7.35) with compensatory low bicarbonate levels, and hyperglycemia (> 250 mg/dL) [12, 13].
Euglycemic Diabetic Ketoacidosis (eDKA)
eDKA is present in patients with ketonemia, metabolic acidosis, but normal serum glucose (<250 mg/dL) [9]. Like DKA, eDKA is a life-threatening condition and more prevalent in type I diabetics with mortality rates ranging from 0.65% to 3.3% [8]. eDKA is brought on by a starvation state where the body shifts energy substrate from carbohydrates to lipid and ketone metabolism. Therefore, conditions that result in starvation and dehydration predispose individuals to develop eDKA. Common risk factors for eDKA include decreased caloric intake, low-carbohydrate diet, pregnancy, acute/chronic alcohol use, surgery, and infection [9]. Women who are pregnant are at increased risk for developing eDKA because pregnancy is a state of accelerated starvation with increased insulin resistance, especially during the second and third trimesters [8]. Acute alcohol use causes anion gap acidosis which elevates the risk of developing eDKA [8]. Chronic alcohol abuse shifts caloric dependence to alcohol’s metabolites, creating a state of chronic carbohydrate deficiency and starvation [8]. Additionally, diabetic patients undergoing bariatric surgery are at an increased risk for developing eDKA and should be monitored closely [8]. Other risk factors for eDKA include insulin pump use, anorexia, ketogenic diet, glycogen storage disorders, gastroparesis, and cirrhosis [2, 9].
Multiple studies indicate that there is an association between SGLT2 inhibitor drug use and eDKA [8]. Patients on SGLT2 inhibitors who have low to normal body mass index or have type 1 diabetes are more susceptible to developing eDKA [8]. However, literature suggests that there is no association between the duration of SGLT2 inhibitor use and eDKA onset [8]. The timeframe between SGLT2 inhibitor exposure and eDKA onset is highly variable, spanning from 0.3 - 420 days [8]. Therefore, all patients on SGLT2 inhibitors that develop vomiting, nausea, malaise, or metabolic acidosis should be screened for ketones in the blood and urine [14].
Management of SGLT2 Inhibitor eDKA
To diagnose eDKA perioperatively, attention should be paid to complete a thorough home medication reconciliation. The index of suspicion of eDKA should be high as the symptoms are nonspecific and normal glucose levels create a false sense of security [2]. Symptoms include malaise, anorexia, and tachypnea in response to ketoacidosis. However, in the setting of surgical procedures and their preceding pathologies, these symptoms may be concealed by post-operative symptomatology. To establish a case of eDKA, laboratory evaluation and diagnostic criteria include venous or arterial blood gas (VBG or ABG) to obtain pH (pH < 7.3), serum bicarbonate (≤ 18 mmol/L), serum and urine ketones (urine ketones > 20 mg/dL), B-hydroxybutyrate (> 3.0mmol/L), anion gap (>12 mEq/L), and electrolytes with particular attention to potassium levels [15].
If eDKA is diagnosed, the treatment mirrors that of hyperglycemic DKA in that it is focused on correction of metabolic acidosis and closure of the anion gap, which is performed with implementation of an insulin drip, dextrose infusion and correction of dehydration with volume resuscitation using crystalloids, and repletion of electrolytes [15]. Our institution’s algorithmic management of post-operative eDKA involves the following: admission to an intermediate or intensive care unit; endocrinology consultation; high volume intravenous infusion of 5% dextrose (starting rate of 200 mL/h) with titration based off of volume status; insulin drip which is initiated at 0.05–0.1 µ/kg/h with hourly rate titration by point of care glucose testing for a goal of 150-200 mg/dL; and serial labs with particular attention to hypokalemia correction which is monitored by basic metabolic panels (BMPs) [16].
Resolution of eDKA occurs when pH > 7.3, bicarbonate > 15 mmol/L, and anion gap closes or is ≤ 12 mEq/L [17]. If the patient is ready to resume oral intake, she or he is converted to a subcutaneous sliding scale insulin regimen, serial blood glucose checks and BMPs are continued to monitor for eDKA recurrence, and a carbohydrate-containing diet is prescribed [16]. The SGLT-2 inhibitor is resumed the next day. If the patient is unable to resume oral intake, dextrose- containing fluids are continued until tolerance of diet per os [16]. Thus, intake of carbohydrates is an important factor in management of eDKA resolution.
Due to the morbidity of eDKA, methods of prevention are of definite interest. The consensus at our institution thus far includes holding SGLT2 inhibitors three to four days before surgery. Preoperative patients have a BMP and B-hydroxybutyrate drawn to identify patients with eDKA. Patients who meet diagnostic criteria for eDKA are admitted, treated per the algorithm outlined, and the procedure delayed until resolution of eDKA. Patients who do not meet diagnostic criteria for eDKA are started on dextrose-containing fluids at a rate of 75-80 mL/h if their blood glucose ˂200 mg/dL and their volume status permits. They proceed with surgery, and intraoperative steroids are avoided unless hemodynamics or suppression of the hypothalamus-pituitary-adrenal (HPA) axis necessitate utilizaiton [16]. Post-procedure, patients are given a carbohydrate-containing snack, instructed to eat a meal upon return to home, restart diabetic medications, and resume their SGLT-2 inhibitor the following day. In summary, procedures can be safely performed on patients prescribed SGLT-2 inhibitors by withholding the drug three to four days prior to surgery, screening for eDKA pre-op, whilst minimizing peri-operative dehydration and time of starvation.
Conclusion
SGLT2 inhibitors are a new class of diabetic drugs that block renal glucose reabsorption and induce a metabolic state of starvation, which can lead to the development of eDKA. Medical professionals must have a high index of suspicion to recognize STGLT2 inhibitors’ potential side effects in perioperative patients and initiate the three major tenants of therapy consisting of insulin infusion, hydration, and electrolyte repletion if eDKA does develop.
Conflicts of Interest
There are no conflicts of interests by any of the authors.
Acknowledgements
None.
Funding
This research received no external funding.
References
-
Patel K, Nair A (2022) A Literature Review of the Therapeutic Perspectives of Sodium-Glucose Cotransporter-2 (SGLT2) Inhibitor-Induced Euglycemic Diabetic Ketoacidosis. Cureus 14(9): e29652.
-
Brown E, Wilding JPH, Alam U, Barber TM, Karalliedde J, et al. (2021) The expanding role of SGLT2 inhibitors beyond glucose-lowering to cardiorenal protection. Ann Med 53(1): 2072-2089.
-
Vallon V, Thomson SC (2020) The Tubular Hypothesis of Nephron Filtration and Diabetic Kidney Disease. Nat Rev Nephrol 16(6): 317-336.
-
Vallon V, Verma S (2021) Effects of SGLT2 Inhibitors on Kidney and Cardiovascular Function. Annual Review of Physiology 83: 503-528.
-
Bonora BM, Avogaro A, Fadini GP (2020) Extraglycemic Effects of SGLT2 Inhibitors: A Review of the Evidence. Diabetes Metabolic Syndrome and Obesity 13: 161-174.
-
Padda IS, Mahtani AU, Parmar M (2023) Sodium-Glucose Transport Protein 2 (SGLT2) Inhibitors. StatPearls Publishing, Treasure Island, Florida, USA.
-
Davies MJ, D’Alessio DA, Fradkin J, Kernan WN, Mathieu C, et al. (2018) Management of Hyperglycemia in Type 2 Diabetes, 2018. A Consensus Report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care 41(12): 2669-2701.
-
Erica C, Clement S, Garg R (2023) Euglycemic Diabetic Ketoacidosis in the Era of SGLT-2 Inhibitors. BMJ Open Diabetes Research & Care 11(5): e003666.
-
Michael CP, Bryant M, King-Thiele R (2023) Euglycemic Diabetic Ketoacidosis. StatPearls Publishing, Treasure Island, Florida, USA.
-
Palmer BF, Clegg DJ (2021) Euglycemic Ketoacidosis as a Complication of SGLT2 Inhibitor Therapy. Clin J Am Soc Nephrol 16(8): 1284-1291.
-
Lizzo JM, Goyal A, Gupta V (2023) Adult Diabetic Ketoacidosis. StatPearls Publishing, Treasure Island, Florida, USA.
-
Burger MK, Schaller DJ (2023) Metabolic Acidosis. StatPearls Publishing, Treasure Island, Florida, USA.
-
Fateen A, Yousaf Z, Khan AA, Razok A, Akram J, et al. (2021) SGLT-2 Inhibitors Associated Euglycemic and Hyperglycemic DKA in a Multicentric Cohort. Scientific Reports 11(1): 10293.
-
Peters, Anne L, et al. (2015) Euglycemic Diabetic Ketoacidosis: A Potential Complication of Treatment with Sodium–Glucose Cotransporter 2 Inhibition. Diabetes Care 38(9): 1687-1693.
-
Nasa P, Chaudhary S, Shrivastava PK, Singh A (2021) Euglycemic diabetic ketoacidosis: A missed diagnosis. World J Diabetes 12(5): 514-523.
-
Shah N, Belalcazar M, Shabot S (2023) Recommendations on SGLT-2 inhibitor use when scheduling elective procedures under anesthesiology care protocol. Division of Endocrinology and Metabolism with Department of Anesthesiology, University of Texas Medical Branch.
-
Kitabchi AE, Umpierrez GE, Miles JM, Fisher JN (2009) Hyperglycemic crises in adult patients with diabetes. Diabetes Care 32(7): 1335-1343.
- Editorial on Multimodal Analgesia
- Surgical Incision Site Local Anaesthetic Infiltration and Superior Hypogastric Plexus Block in Total Abdominal Hysterectomy Under General Anaesthesia- A Placebo-Controlled, Randomized Clinical Trial
- Supraglottic Airway Insertion in Semi Fowler Position Due to Severe Thoracic Hyperkyphosis: A Case Report
- Anaesthetic Management of Cardiac Myxoma Patient with Systemic Involvement: A Case Report
- Current Problems in Pulmonary Respiratory Distress Syndrome (Literature Review)
- Evolution of Perioperative Hemodynamic Monitoring from the Hand on Pulse to Hypotension Prediction Index