Cytologic Surveillance Versus Immediate Referral to Colposcopy for Women with a Cervical Cytology Diagnosis of ASC-US and LSIL in the Absence of HPV DNA Test
Background and Objectives: Cytology screening programmes decrease the risk of cervical cancer by detecting the precancerous changes. Treating these reduce the likelihood of developing invasive disease in future. The management strategies for severe precancerous changes are well established, however, this is not the case with minor cytological abnormalities like ASCUS or LSIL especially when a triage strategy like HPV testing is not easily available. This study aims to assess whether immediate referral to colposcopy is better than cytologic surveillance for women with a cervical smear diagnosis of ASC-US and LSIL in a context where HPV test is either unavailable or not affordable. Methods: A prospective study was conducted at a tertiary care hospital between January 2021 and November 2022. Total 126 women with a Pap smear report of ASC-US or LSIL were recruited to receive either cytologic surveillance (Group A) or immediate colposcopy (Group B), with 63 women in each group. Adherence to follow up and eventual histologic diagnosis of HSIL on colposcopically directed biopsy (CDB) and/or Loop electrical excision procedure (LEEP) were considered as the main study end-point. Results: Significantly more women defaulted from the cytologic surveillance group than the immediate colposcopy group (p=0.00001). In group B, using CDB and LEEP, 5 additional high-grade lesions were detected. However, the p value was not significant when compared with the cytologic surveillance group (p=0.360). Interpretation and Conclusions: Cytologic surveillance is fraught with a poor compliance rate. In the absence of HPV DNA test, minor cytologic abnormalities should undergo immediate colposcopy if follow up cannot be ensured. The high persistence rates of ASC-US and LSIL (41.18% and 35.71%), as well as the high progression rate of LSIL in the cytologic surveillance group, also underscore the necessity for these women to undergo immediate referral to colposcopy.
Introduction
In India, the age standardised incidence rate of cervical cancer is 10.9 to 18.3 per 100,000 women and the age standardised mortality rate is 9.1 to 12.4 per 100,000 women per year [1]. Through the use of Pap smear, which aims to detect precancerous changes which might progress in some women and put them at risk of developing an invasive disease in the future, cytology screening programmes lower the risk of cervical cancer. To prevent the latter, screen detected severe precancerous changes require treatment, preferably after a thorough colposcopic evaluation. However, a significant number of women are diagnosed with borderline cytological abnormalities i.e., Atypical Squamous Cells of Undetermined Significance (ASC-US) & Low Grade Squamous Intraepithelial Lesion (LSIL) and yet there are differing opinions on how to manage women with these minor cytologic changes i.e., ASC- US or LSIL, especially in resource-limited settings.
A significant number of LSILs undergo spontaneous regression. Spontaneous regression of these lesions (ASC- US & LSIL) is known in 70-80 % women [2]. Therefore, the surveillance strategy for women with minor cytologic changes is currently with a repeat Pap smear (cytologic surveillance) at 6 & 12 months [3]. However, cytologic surveillance is fraught with poor compliance rate thereby putting women at risk to developing invasive disease [4].
With the advent of Liquid Based Cytology (LBC), reflex HPV DNA testing has proven to be an effective triage means for follow up and further management of women with minor cervical abnormalities [5]. However, there is no affordable global standard for the HPV DNA test currently [6]. Because of non-availability of HPV DNA test, immediate colposcopy may be a viable alternative. Immediate colposcopy has the disadvantage of over diagnosis and over treatment [7, 8] but the chances of detecting precancerous lesions are higher than with cytological surveillance [9].
This study is undertaken with the hypothesis that immediate referral to colposcopy is a better management option for minor cervical abnormalities detected by Pap smear, as compared to cytologic surveillance.
The main objective of this study was to assess whether immediate referral to colposcopy is better than cytologic surveillance in detecting CIN 2+ lesions in women with a cervical smear diagnosis of ASC-US and LSIL in the absence of HPV DNA test. Our secondary objective was to correlate cytologic findings and colposcopy diagnosis with histopathology (CDB - Colposcopically Directed Biopsy and LEEP - Loop Electrosurgical Excision Procedure) when available.
Materials and Methods
The current study was conducted as a prospective study from January 2021 to November 2022 at a tertiary care hospital after the approval from the Institutional Ethics committee. All females, symptomatic or asymptomatic undergoing Pap smear in the Gynaecology OPD and with a cytological diagnosis of ASC-US & LSIL were included in the study. Pregnant women and women with vaginal bleeding because of any cause or those who refuse to give consent were excluded.
All women who were eligible and consenting and had a Pap smear diagnosis of ASC-US and LSIL were sequentially enrolled in one of the two groups i.e., group A or group B (63 women in each group). For cytologic surveillance, all women with odd serial numbers were assigned group A, while those with even serial numbers were assigned group B for immediate colposcopy. Six months after their initial Pap smear cytology, group A women were advised to undertake a repeat Pap smear. Colposcopic evaluation of the cervix and, if necessary, colposcopically guided cervical biopsies were performed on group A women who had persistent ASC-US and LSIL or worse at 6 months. Group B women underwent immediate colposcopy (on the same day when she came to collect the report or within 3 weeks from recruitment) and colposcopically directed cervical biopsy (CDB) as appropriate. LEEP was performed in women when the follow up cytologic smear report was HSIL or when clinically indicated (even when the Pap smear report was less than HSIL). Pap smears were reported according to The Bethesda System- 2014 and colposcopic findings were graded according to the SWEDE score grading system [10].
Follow-up Procedures
The women included in the study were followed up using their telephone numbers, address and Aadhar card numbers /addresses. With the above details, these women were reminded about their appointment dates.
Statistical Analysis
STATA software was used to code and analyse the data (version 10.1, 2011 by Stata Corp, Texas, USA). Drop-out rates in 2 groups were compared with Binomial test for proportions and risk ratio for estimating risk of drop out were calculated along with 95% Confidence Interval.
For all comparisons, a p value of 0.05 or lower was regarded as statistically significant.
Observations and Results
The study included 126 women in total who fulfilled the inclusion criteria. Each study group was assigned 63 women i.e., Group A- cytologic surveillance and Group B- immediate colposcopy group (Flow chart 1 & 2). Regarding the sociodemographic traits, there was no statistically significant difference between the two participant groups (Table 1). In group A, out of 63 women, 32 were lost to follow up. Whereas, in group B, out of 63 women 9 women were lost to follow up. Out of the 31 women who underwent repeat Pap smear after 6 months, 15 women (ASCUS- 2, LSIL- 5, HSIL- 1) were subjected to colposcopy and CDB. In group B, 54 women were subjected to immediate colposcopy whereas, CDB was taken only in 37 women. Only a single case of HSIL was detected in Group A while the number was 6 in Group B on histopathology (Flow chart 1, 2). The primary objectives were evaluated in the form of p value and risk ratio in between the two groups (Table 2). Results of Pap smear and colposcopy scoring system- SWEDE score was correlated with colposcopically directed biopsy (CDB) (Tables 3 & 4). The correlation of colposcopically directed biopsy and LEEP tissue in our study showed that Cohen’s kappa statistic ĸ was 0.4286 indicating moderate level of agreement between the two.
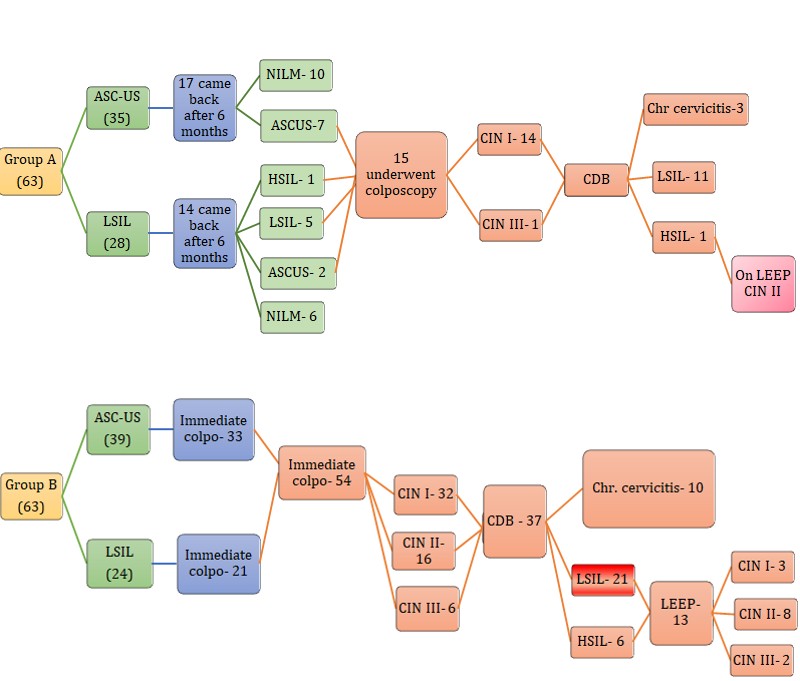
Flow Chart 1: Study flowchart of Group A.
Flow Chart 2: Study flowchart of Group B.
| Cytologic Surveillance (n=63) | Immediate Colposcopy (n=63) | p Value | |
|---|---|---|---|
| Age (years) | |||
| ≤35 | 25 (39.68%) | 25 (39.68%) | 1 |
| 36-50 | 25 (39.68%) | 27 (42.85%) | 0.71 |
| >50 | 13 (20.64%) | 11 (17.47%) | 0.65 |
| Residence | |||
| Rural | 33 (52.38%) | 29 (46.04%) | 0.5 |
| Urban | 30 (47.62%) | 34 (53.96%) | 0.5 |
| Socio-Economic status | |||
| Upper, Upper middle, Upper lower | 12 (19.05%) | 13 (20.63%) | 0.82 |
| Lower Middle | 43 (68.25%) | 45 (71.43%) | 0.69 |
| Lower | 08 (12.70%) | 05 (7.94%) | 0.37 |
| Parity | |||
| 0 or 1 | 10 | 15 | 0.26 |
| ≥2 | 53 | 48 | 0.26 |
| Menopause | |||
| Yes | 17 (26.98%) | 14 (22.22%) | 0.53 |
| No | 46 (73.02%) | 49 (77.78%) | 0.53 |
| Contraception | |||
| Barrier | 16 (25.40%) | 15 (24.60%) | 0.83 |
| OC Pills | 4 (6.35%) | 3 (4.76%) | 0.69 |
| Sterilization | 40 (63.49%) | 41 (65.08%) | 0.85 |
| No contraception | 3 (4.76%) | 4 (6.35%) | 0.69 |
Table 1: Displaying study participants’ sociodemographic information.
| Group A | Group B | p value | Risk ratio (95% CI) | |
|---|---|---|---|---|
| Loss to follow up | 32 | 9 | 0.00001 | 3.555 (1.8527, 6.8236) |
| High grade lesions on colposcopy (SWEDE score ≥5) | 1 | 22 | 0.0132 | 6.111 (0.896, 41.71) |
| Histologic diagnosis of HSIL | 1 | 6 | 0.36 | 2.432 (0.31, 18.52) |
Table 2: Displays the risk ratio and p value for groups A and B.
| LSIL | HSIL | |
|---|---|---|
| Sensitivity | 41.02% | 85.70% |
| Specificity | 84.61% | 100% |
| PPV | 92% | 100% |
| NPV | 40.74% | 88.23% |
| Diagnostic accuracy | 65.38% | 88.46% |
Table 3: The test parameters of Pap smear for LSIL and HSIL as against colposcopically directed biopsy (CDB).
| Sensitivity | 100% |
| Specificity | 64.50% |
| PPV | 30.43% |
| NPV | 100% |
| Diagnostic accuracy | 69.23% |
Table 4: The performance parameters of SWEDE score for grading cytological abnormalities as against the colposcopically directed
Discussion
According to The Federation of Obstetric and Gynaecological Societies of India (FOGSI) Good Clinical Practice Recommendation (GCPR) screening guidelines [3], repeat cytology should be performed every 12 months for two years in women with age 30 or less and who have a Pap smear report of ASCUS and LSIL. If the preinvasive lesion is persistent even after 2 years, colposcopy should be performed. The multiple visits to the clinic required for this cytologic surveillance leads to a high number of dropouts. Repeat cytology could also delay referral, which would affect recall compliance. Therefore, immediate colposcopy or VIA (visual inspection after application of acetic acid) and directed biopsy may be acceptable in such cases. Women with ASC-US between the ages of 30 and 64 should be triaged, ideally with an HPV test, but if it is not available, repeat cytology after a year is recommended. If any of these tests is positive then colposcopy and directed biopsy should be performed. It is acceptable to perform an immediate colposcopy or VIA and directed biopsy at places where a triage test, particularly HPV DNA testing, is not available. Women over the age of 30 who have a Pap smear result of LSIL should undergo colposcopy. At places where colposcopy services are limited, a triage test like HPV DNA testing can be utilised. ‘See-and-Treat’ approach is acceptable if compliance is in doubt.
Immediate colposcopy is being considered even for screen detected minor cytologic abnormalities: firstly because of poor compliance for ‘cytology surveillance’. According to a UK report, their organised cervical screening programme had a default rate of 21%. This might be worse in resource-poor countries without such formal programmes [11]. Additionally, some cases of high-grade disease may fail to be picked up by cytologic surveillance due to loss of follow-up or the Pap smear’s limited sensitivity [12]. Errors in sampling and interpretation are primarily responsible for the low sensitivity [13] and ranges from as low as 1.5% to as high as 80% [14]. Doing immediate colposcopy in women with ASC-US and LSIL may aid in identifying women at risk of Cervical intraepithelial neoplasia 2+ (CIN2+) (significant lesions) [15]. Secondly, and most importantly, as the persistence rate and progression rate of LSIL is 35.71% and 7.15% respectively, immediate colposcopy may be of more use than ‘watchful waiting’ using a repeat Pap smear. According to a study, an immediate colposcopy would be less expensive than having multiple repeat smears done [16]. Colposcopy is eventually recommended for 65- 75% of women with LSIL, even at the best centres in the world [16, 17]. According to the ALTS (ASCUS/LSIL Triage) trial, women with an index cytology showing LSIL would benefit from an immediate colposcopy [18]. Our study was conducted to determine whether immediate referral to colposcopy is a better management strategy than watchful waiting with cytologic surveillance for women with minor cytologic abnormalities.
In the present study, 50.79% of the women in the cytologic surveillance group were lost to follow up i.e., these women did not come back after 6 months for repeat Pap smear despite repeated reminders. In comparison to the default rate of 42% reported in a study by Yoost J, et al. [4] the default rate for the cytologic surveillance group in our study was relatively higher [4] and also higher as compared to 37% in Ajah’s L, et al. [19]. The default rate in the study by Shafi MI, et al. [11] was also lower as compared to the present study where 21% women defaulted from the deferred treatment group during the 24 months surveillance period [11]. We observed that, 20 / 32 of our women who defaulted were residing in the rural areas. Thus, this high default rate could be due to the distant location of the hospital. Also, our study period coincided with the COVID restrictions, making it difficult for women to comply with the recall procedures. Group A had a three times greater risk of dropping out in comparison to group B i.e., immediate referral to colposcopy group (14.29%) with a significant p value (p=0.0001) (Table
2). p value was also significant in the study by Ajah L, et al. [19]. Flannelly G, et al. [20], Kitchener H, et al. [21], Little J, et al. [9], Walker J et al. [18], Shafi MI, et al. [11] observed the default rate at various periods (6, 12 and 24 months) (Table 5). They observed that the risk of non-compliance increased with the duration of the follow-up and was significantly higher for the repeat cytology arm [22]. According to Kyrgiou M, et al. [22] meta-analysis, there was a four-fold increase in non-compliance at 6 months, a six-fold increase at 12 months, and a 19-fold increase at 24 months for the cytologic surveillance group.
| Risk ratio (95% CI) | |
| Present study | 3.555 (1.8527, 6.8236) |
| Flannelly [20] | 35.37 (2.15, 580.52) |
| Kitchener [21] | 4.92 (2.01, 12.08) |
| TOMBOLA [9] | 1.88 (1.56, 2.27) |
Table 5: Comparison of risk ratio of the default rates with other studies.
We used the SWEDE scoring system for grading colposcopic abnormalities. According to this scoring system, in the present study, 22 women from the immediate colposcopy group had a score of ≥5 compared to 1 woman in the cytologic surveillance group (Table 2). But on final CDB and LEEP tissue, histologic diagnosis was HSIL in 6 (16.21%) women in immediate colposcopy group as opposed to 1 (6.67%) woman in the cytologic surveillance group suggesting no statistically significant difference in the proportion of women in the two groups who eventually received a histologic diagnosis of HSIL (p=0.36) (Table 2). This could have been because of a less number of women from the cytologic surveillance group were subjected to colposcopy and CDB, as the return rate in this group was poor. Our findings were comparable with those of the study conducted by Ajah L, et al. [19] (4.9% in the cytologic surveillance group versus 8.7% in the immediate colposcopy group; p=0.68). Flannelly G et al. [20] observed that in the six months surveillance group, immediate colposcopy arm could detect 22.1% CIN 2 lesions histologically as opposed to the 16.3% diagnosed in the cytological surveillance arm. Also, immediate colposcopy detected 67.6% CIN 2+ lesions histologically in immediate colposcopy arm as opposed to 36.9% diagnosed in the cytological surveillance group. Other studies like Solomon D, et al. [23], Shafi MI, et al. [11] presented the data more than one point time and observed that, at the first time point (prior to the exit examination at the trial’s completion), the immediate colposcopy group had a higher incidence of CIN2+, but there was no difference over time [22]. Accordingly, no statistically significant difference was found between the proportions of women in the two groups who were eventually histologically diagnosed with HSIL at the end of the study. This was also our observation.
In our study, the overall reversion rate with 6 months of cytologic surveillance of ASC-US and LSIL without HPV DNA testing was 51.61% (Table 6). ASC-US and LSIL each had a reversion rate of 58.82% and 42.85%, respectively. Among women who had cytologic surveillance, the regression rate of LSIL was 46.1% in a study carried out by Ajah L, et al. [19]
and 26% in Yoost J, et al. study [4]. The regression rate in the above studies was also reported in the absence of HPV testing. In a study carried out by Moscicki A, et al. [24] in France, the regression rates reported for LSIL over a period of 12 and 36 months was 61% and 91% respectively. They observed that negative HPV status of the recent visit was associated with regression, and no association was found between regression of LSIL and the baseline HPV status [24].
| Pap smear | Repeat Pap smear results after 6 months | Total | |||
|---|---|---|---|---|---|
| NILM | ASC-US | LSIL | HSIL | ||
| ASC-US | 10 (58.82%) | 7 (41.18%) | 0 | 0 | 17 (100%) |
| LSIL | 6 (42.85%) | 2 (14.28%) | 5 (35.72%) | 1 (7.15%) | 14 (100%) |
| Total | 16 (51.61%) | 9 (29.04%) | 5 (16.13%) | 1 (3.22%) | 31 (100%) |
Table 6: Results of Repeat Pap smear for women in cytologic surveillance Group A.
In our study, the persistence rate with 6 months of cytologic surveillance for ASC-US and LSIL was 41.18% and 35.71% respectively (Table 6). The persistence rate of LSIL was 43.4% in study by Ajah L, et al [19]. Yoost J, et al. [4] observed a persistence rate of 15% in cases of LSIL. According to Flannelly G, et al. [20] the persistence rate of LSIL and HSIL among women under cytologic surveillance was 42.2% after six months, 44.9% after a year, and 30.4% after 24 months.
The progression rate of LSIL with 6 months of cytologic surveillance was 7.15% in our study (Table 6). However, the estimation of progression in the cases who have defaulted cannot be commented upon. 6 months of cytologic surveillance for LSIL revealed a progression rate of 3.4%, according to Ajah L, et al. [19]. LSIL progression was observed to be 17%, according to Yoost J, et al. [4]. Flannelly G, et al. [20] observed that the persistence rate of LSIL and HSIL among women who had cytologic surveillance was 42.2% over a period of 6 months, 44.9% over a period of 12 months and 30.4% over a period of 24 months.
Since we had tissue for follow up, we correlated cytological findings with CDB and LEEP tissue. In comparison to a study by Patil P, et al. [25] where the correlation between cytology and histopathology was found to be 57% overall with the highest correlation in the HSIL category (87.5%), our study found an overall concordance between Pap smear and CDB of 63.46% (Table 3).
The test parameters of Pap smear for LSIL and HSIL in our study were comparable to a study by Dhakal R, et al. [26] in which the sensitivity was found to be 77.80%, whereas the specificity was 100%, the observed positive predictive value (PPV), and negative predictive value (NPV) of Pap smear in their study was 100%, and 97% respectively. According to Patil P, et al. [25] the observed diagnostic accuracy for Pap smear was 82.1% with a sensitivity of 77.7%, specificity of 84.2%, a positive predictive value of 70%, and negative predictive value of 88.8%25. The diagnostic accuracy of Pap smear was 88.23% for HSIL and 65.38% for LSIL in our study.
In our study, when the colposcopic scores and histopathologic diagnosis were correlated, then there was fair agreement of 69.23% (ĸ- 0.328, p= 0.001) (Table 4). Rahman Z, et al. [27] found that the colposcopic impression according to Swede score and histopathological report showed a good level of agreement using kappa statistics (ĸ= 0.761, p<0.001). In a study to determine the efficacy of colposcopy for the diagnosis of HSIL or worse (HSIL+) in women with human papillomavirus infection and ASCUS cytology, Ding Z, et al. [28] found that the agreement between colposcopic impression and cervical pathology was perfectly matched in 89.2% of cases (553/620), and the strength of agreement with the ĸ statistic was 0.698 (p<0.001). Colposcopy had a high specificity (96.9%) but a low sensitivity (67.5%) for detecting HSIL+ lesions in their study.
The Cohen’s kappa statistic in our study was 0.4286, indicating a moderate correlation between CDB and LEEP specimens. The overall histopathology concordance rate between CDB and LEEP was 76.92%. The underestimation rate for LSIL was found to be 57.14% (4 cases) meaning that these 4 cases were reported as CIN 1 on CDB which turned out to be CIN 2 or higher on LEEP tissue. Whereas there was no lower grade lesion detected in LEEP when CDB findings were of HSIL, meaning that the current study did not overestimate or overtreat patients. The 4 false negative cases could have been due to the limited amount of tissue provided in the CDB as against that provided in the LEEP biopsy. In order to ascertain the factors influencing the histopathologic discrepancy and final diagnosis between CDB
and LEEP, Jung Y, et al. [29] carried out a study. They noted that underestimation rates for biopsy results with normal, CIN 1, CIN 2, and CIN 3 were 75.0%, 24.7%, 23.4%, and 24.2%, respectively, and that the overall concordance rate of histopathology between punch biopsy and LEEP was 43.3%. In 47 patients who underwent LEEP, Massad L, et al. [30] compared the results with those of CDB and discovered that 28% of the women had no dysplasia and only 11% had worse lesions at the biopsy site. With a Spearman’s correlation of 0.43 and a Cohen’s ĸ statistic for biopsy grade on colposcopy and loop specimen site, it was determined that there was a moderate correlation between the two types of specimens. This was also the observation in our study.
Conclusion
- In the absence of HPV DNA testing and in situations where it is anticipated that there will be low compliance for cytological surveillance, women may be referred for an immediate colposcopy following a single Pap smear report of ASC-US or LSIL.
- Immediate colposcopy and CDB and / or LEEP could detect 6 high grade lesions (compared to only one in cytology surveillance arm). Therefore, there was a chance that all or few of these high-grade lesions would have been missed if an immediate colposcopy had not been performed on these women.
- In spite of the poor compliance of women in the surveillance group we could detect one high grade lesion indicating that aggressive and complete compliance may detect a greater number of HSILs.
- In a country like India, where ensuring compliance to recall for repeat smears is difficult, and the high persistence and progression rates of ASC-US and LSIL that we observed in our study is a testimony to the fact that immediate referral to colposcopy of women in the cytologic surveillance group can be a beneficial strategy.
Implication
• Portable colposcopes may be used during second visit to women participating in screening camps so that those with reports of ASC-US and LSIL can undergo Immediate colposcopy.
• In the scenario of rural camps, this may require lesser number of repeat visits by both the participating women and the doctors. Using the strategy of immediate colposcopy has the potential to increase the use of the “See and Treat” approach.
• At the community level, the results of this study are in a position to recommend a revised surveillance policy, for ASC-US & LSIL, to the National Cancer Control Program of India.
Disclaimer
Where authors are identified as personnel of the International Agency for Research on Cancer/World Health Organization, the authors alone are responsible for the views expressed in this article and they do not necessarily represent the decisions, policy or views of the International Agency for Research on Cancer/World Health Organization.
Acknowledgement and Source of financial support
This study was awarded the Indian Council of Medical Research (ICMR) Financial Support for the MD Thesis.
References
-
Mathur P, Sathishkumar K, Chaturvedi M, Das P, Sudarshan KL, et al. (2020) Roselind FS; ICMR-NCDIR- NCRP Investigator Group. Cancer Statistics, 2020: Report From National Cancer Registry Programme, India. JCO Glob Oncol 6: 1063-1075.
-
Bansal N, Wright JD, Cohen CJ, Herzog TJ (2008) Natural history of established low grade cervical intraepithelial (CIN 1) lesions. Anticancer Res 28(3B): 1763-1766.
-
Bhatla N, Singhal S, Saraiya U, Srivastava S, Bhalerao S, et al. (2020) Screening and management of preinvasive lesions of the cervix: Good clinical practice recommendations from the Federation of Obstetrics and Gynaecologic Societies of India (FOGSI). Journal of Obstetrics and Gynaecology Research 46(2): 201-214.
-
Yoost JL, Goetzl L, Hoda R, Soper DE, Barry A (2009) Management of the low grade squamous intraepithelial lesion Pap smear in a cross-sectional, observational cohort. J Reprod Med 54(7): 421-424.
-
Bulkmans NW, Berkhof J, Rozendaal L, Van Kemenade FJ, Boeke AJ, et al. (2007) Human papillomavirus DNA testing for the detection of cervical intraepithelial neoplasia grade 3 and cancer: 5-year follow-up of a randomised controlled implementation trial. Lancet 370(9601): 1764-1772.
-
Massad LS, Einstein MH, Huh WK, Katki HA, Kinney WK, et al. (2012) ASCCP Consensus Guidelines Conference. 2012 updated consensus guidelines for the management of abnormal cervical cancer screening tests and cancer precursors. Obstet Gynecol 121(4): 829-846.
-
Anorlu RI, Orakwue CO, Oyeneyin L, Abudu OO (2004) Late presentation of patients with cervical cancer to a tertiary hospital in Lagos: what is responsible? Eur J Gynaecol Oncol 25(6): 729-732.
-
Cronje HS (2004) Screening for cervical cancer in developing countries. Int J Gynaecol Obstet 84(2): 101- 108.
-
Little J, Day N, Marteau T, Parmar M, Patnick J, et al. (2009) Cytological surveillance compared with immediate referral for colposcopy in management of women with low grade cervical abnormalities: Multicentre randomised controlled trial. BMJ (Online) 339(7716): 329.
-
Bornstein J, Bentley J, Bosze P, Girardi F, Haefner H, et al. (2012) 2011 colposcopic terminology of the International Federation for Cervical Pathology and Colposcopy. Obstet Gynecol 120(1): 166-172.
-
Shafi MI, Luesley DM, Jordan JA, Dunn JA, Rollason TP, et al. (1997) Randomised trial of immediate versus deferred treatment strategies for the management of minor cervical cytological abnormalities. British Journal of Obstetrics and Gynaecology 104(5): 590-594.
-
Taylor RJ, Morrell SL, Mamoon HA, Wain GV (2001) Effects of screening on cervical cancer incidence and mortality in New South Wales implied by influences of period of diagnosis and birth cohort. J Epidemiol Community Health 55(11): 782-788.
-
Joste NE, Crum CP, Cibas ES (1995) Cytologic/histologic correlation for quality control in cervicovaginal cytology. Experience with 1,582 paired cases. Am J Clin Pathol 103(1): 32-34.
-
Pairwuti S (1991) False-negative Papanicolaou smears from women with cancerous and precancerous lesions of the uterine cervix. Acta Cytol 35(1): 40-46.
-
Dodd LG, Sneige N, Villarreal Y, Christina VF, Gregg AS, et al. (1993) Quality-assurance study of simultaneously sampled, non-correlating cervical cytology and biopsies. Diagnostic Cytopathology 9(2): 138-144.
-
Johnson N, Sutton J, Thornton JG, Lilford RJ, Johnson VA, et al. (1993) Decision analysis for best management of mildly dyskaryotic smear. Lancet 342(8863): 91-96.
-
Kyrgiou M, Koliopoulos G, Martin-Hirsch P, Kehoe S, Flannelly G, et al. (2007) Management of minor cervical cytological abnormalities: a systematic review and a meta-analysis of the literature. Cancer Treat Rev 33(6): 514-520.
-
Walker J (2003) A randomized trial on the management of low-grade squamous intraepithelial lesion cytology interpretations. Am J Obstet Gynecol 188(6): 1393-1400.
-
Ajah LO, Chigbu CO, Onah HE, Iyoke CA, Lawani OL, et al. (2014) Cytologic surveillance versus immediate colposcopy for women with a cervical smear diagnosis of low-grade squamous intraepithelial lesion in a poor setting in Nigeria. Onco Targets Ther 7: 2169-2173.
-
Flannelly G, Anderson D, Kitchener HC, Mann EM, Campbell M, et al. (1994) Management of women with mild and moderate cervical dyskaryosis. BMJ 308(6941): 1399-1403.
-
Kitchener HC, Burns S, Nelson L, Myers AJ, Fletcher I, et al. (2004) A randomised controlled trial of cytological surveillance versus patient choice between surveillance and colposcopy in managing mildly abnormal cervical smears. BJOG: An International Journal of Obstetrics and Gynaecology 111(1): 63-70.
-
Kyrgiou M, Kalliala I, Mitra A, Ng KYB, Raglan O, et al. (2017) Immediate referral to colposcopy versus cytological surveillance for low-grade cervical cytological abnormalities in the absence of HPV test: A systematic review and a meta-analysis of the literature. Int J Cancer 140(1): 216-23.
-
Solomon D (2003) R esults of a randomized trial on the management of cytology interpretations of atypical squamous cells of undetermined significance. Am J Obstet Gynecol 188(6): 1383-1392.
-
Moscicki AB, Shiboski S, Hills NK, Powell KJ, Jay N, et al. (2004) Regression of low-grade squamous intra- epithelial lesions in young women. Lancet 364(9446): 1678-1683.
-
Patil P, Jibhkate S (2016) Cytohistopathological correlation of Papanicolaou smears: a hospital based study. Int J Reprod Contracept Obstet Gynecol 5(6): 1695-1699.
-
Dhakal R, Makaju R, Sharma S, Bhandari S, Shrestha S, et al. (2016) Correlation of Cervical Pap Smear with Biopsy in the Lesion of Cervix. Kathmandu Univ Med J (KUMJ) 14(55): 254-257.
-
Rahman Z, Yadav G, Tripathi U (2020) The Diagnostic Efficacy of Swede Score for Prediction of Pre-invasive Cervical Lesions: A Prospective Hospital-Based Study. J Obstet Gynaecol India 70(6): 497-502.
-
Ding Z, Li Y, Chen A, Song M, Zhang Y (2016) Punch biopsy guided by both colposcopy and HR-HPV status is more efficient for identification of immediate high- grade squamous intraepithelial lesion or worse among HPV-infected women with atypical squamous cells of undetermined significance. Eur J Obstet Gynecol Reprod Biol 207: 32-36.
-
Jung Y, Lee AR, Lee SJ, Yong SL, Dong CP, et al. (2018) Clinical factors that affect diagnostic discrepancy between colposcopically directed biopsies and loop electrosurgical excision procedure conization of the uterine cervix. Obstetrics & Gynecology Science 61(4): 477-488.
-
Massad LS, Halperin CJ, Bitterman P (1996) Correlation between colposcopically directed biopsy and cervical loop excision. Gynecol Oncol 60(3): 400-403.
- Huddled and Preternatural- Atypical Lobular Hyperplasia
- Callow and Vernal-Hepatoblastoma
- Black Plum Fruit Extract as a Substitute for Haematoxylin in Haematoxylin and Eosin Staining Technique
- Critical Analysis of World Status of Research on the Development of High Yielding Strains of Jatropha Curcas L
- Non-Invasive Follicular Thyroid Neoplasm with Papillary-Like Nuclear Features: Pitfalls of Cytological and Histopathologic Diagnosis
- Melissopalynology in Some Regions of Kermanshah Province (West of Iran)