Ectopic Pregnancy in the Cervix-A Case Report with Review of Literature
Cervical ectopic pregnancy is a rare type of ectopic pregnancy with an evidence of less than 0.1% of all ectopic pregnancies. It is associated with high morbidity and mortality and may lead to massive hemorrhage, which may require hysterectomy to save the patient. We report a case of ectopic pregnancy in cervix in a 27-year-old female patient with a previous history of lower segment caesarean section (LSCS). The current pregnancy was complicated with a massive hemorrhage, hence leading to hysterectomy.
Introduction
Cervical ectopic pregnancy is the implantation of blastocyst in the intracervical canal. Cervical ectopic pregnancy is extremely rare and accounts for less than 1% of all ectopic pregnancies [1]. It is associated with high morbidity and mortality if it is not treated correctly. We present a case of ectopic pregnancy in the cervix who presented with massive bleeding and underwent hysterectomy.
Case Report
A 27 year old female patient presented with 10 weeks of amenorrhea and Per vaginal (PV) pleading on and off since one month.
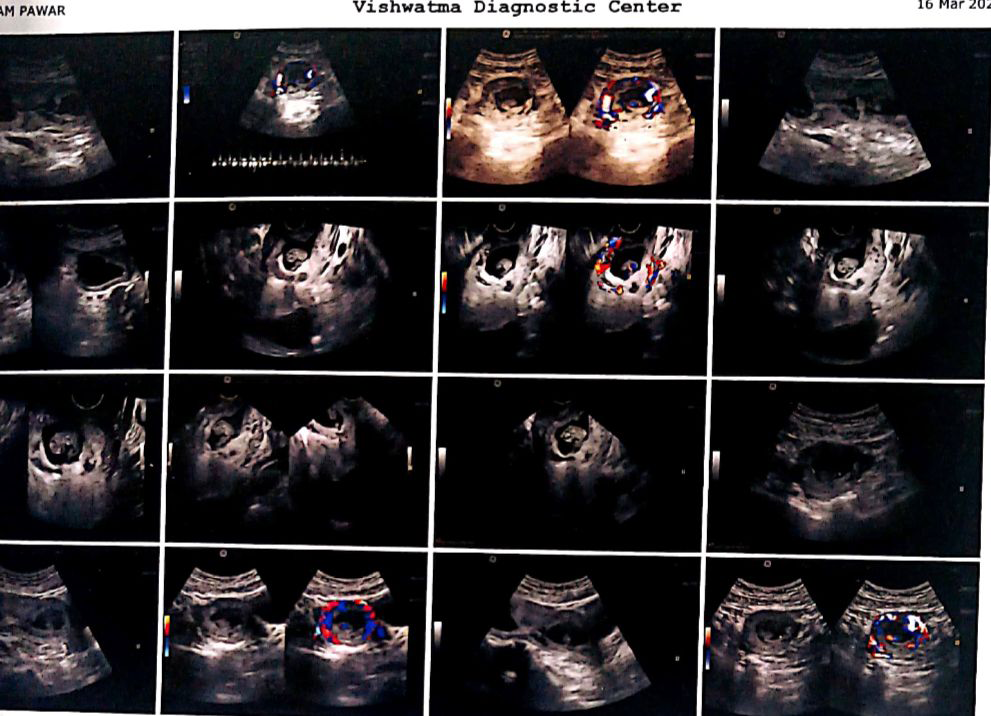
She was second gravida with history of LSCS during previous delivery. Recently, there was massive PV bleeding without abdominal cramps since two days. Ultrasonography revealed a single irregular gestational sac in the cervical canal. A single fetal pole with cardiac activity was noted. Features were suggestive of cervical ectopic pregnancy (Figure 1).
Patient underwent emergency hysterectomy because of massive bleeding per vagina and the specimen was sent for histopathological examination. Gross examination revealed specimen of uterus with cervix measuring 11 × 5 × 4 cm. External surface was unremarkable. On cut section, endometrial Canal was 6 cm in length with endometrial thickness of 0.7 cm. Endometrial cavity was unremarkable. Cervical canal was 3 cm in length and was obliterated by grey white to grey brown friable tissue mass measuring 1.5 x 0.5 x 0.3 cm, which was seen below the internal os (Figure 2).

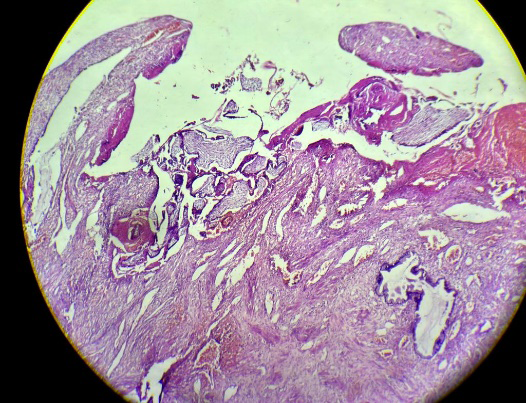
Microscope reveals chorionic villi and decidua attached to endocervical tissue which confirmed cervical ectopic pregnancy. Sections from endometrium reveal Arias-Stella reaction and no evidence of products of conception. Thus, the case was diagnosed as cervical ectopic pregnancy (Figure 3).
Discussion
Cervical ectopic pregnancy was first published in 1978 by Raskin [1]. Any compromise in the capacity of the uterine cavity that prevents implantation in the endometrium could be a contributing factor [2]. The major risk factors include in vitro fertilization, endometrial injury caused by pelvic inflammatory disease or postsurgical trauma such as cesarean section or uterine curettage, history of abortions, intrauterine device use, and structural uterine anomalies [3]. In our case, the risk factor seemed to be LSCS. The most common symptom is vaginal bleeding followed by a period of amenorrhea and urinary problems in cases of advanced pregnancies [4]. At times, massive bleeding can occur which may require emergency hysterectomy to save the patient as seen in our case. Paalman and Mcelein in 1959 proposed five clinical criteria for diagnosis of cervical ectopic pregnancy which include:
- Uterine Bleeding without cramping pain following period of amenorrhea.
- Soft enlarged cervix.
- Product of conception entirely confined and firmly attach with endocervix.
- Closed internal cervical os.
- Partially opened external cervical os [5].
Most of these criteria’s were seen in our case. Differential diagnosis of cervical ectopic pregnancy include aborting intra uterine pregnancy residing in cervix which can be differentiated by sliding sign on trans vaginal USG which was suggested by Jurkovic, et al. in 1966 [6]. Larger or globular uterus in uterine pregnancy compared to hourglass configuration in cervical pregnancy is helpful for definitive diagnosis. As a consequence of the rarity of the condition, therapeutic approaches are still mainly based on case series studies [7]. The therapeutic protocols for cervical ectopic pregnancy have not yet been standardized, although there are general recommendations [8]. The treatment method should be based on the patient’s desire to preserve fertility, hemodynamic state, and gestational age, taking into account initial serum hCG level, crown-rump length, and the presence or absence of fetal heartbeat [9]. For hemodynamically stable patient, a conservative treatment like systemic or local methotrexate injection is suggested [10, 11, 12, 13]. For uncontrolled bleeding, cervical cerclage, balloon tamponade, angiographic embolization, uterine artery ligation or hysterectomy may be needed [14].
Conclusion
Cervical ectopic pregnancy is a rare condition and can be life threatening. Early diagnosis and intervention is necessary in preserving patient’s fertility without significant complications.
References
-
Raskin MM (1978) Diagnosis of cervical pregnancy by ultrasound: a casereport. Am J Obstet Gynecol 130: 234- 235.
-
Marcovici I, Rosenzweig BA, Brill AI, Khan M, Scommegna A (1994) Cervical pregnancy: case reports and a current literature review. Obstet Gynecol Surv 49(1): 49-55.
-
Vora PH, Jassawalla MJ, Bhalerao S, Nadkarni T (2016) Cervical ectopic pregnancy: a clinician’s dilemma. J Obstet Gynaecol India 66(S2): 617-619.
-
Copas P, Semmer J (1983) Cervical ectopic pregnancy: sonographic demonstration at 28 weeks gestation. J Clin Ultrasound 11: 328-330.
-
Paalman RJ, McElin TW (1959) Cervical pregnancy; review of the literature and presentation of cases. Am J Obstet Gynecol 77: 1261-1270.
-
Kirk E, Condous G, Haider Z, Syed A, Ojha K, et al. (2006) The conservative management of cervical ectopic pregnancies. Ultrasound Obstet Gynecol 27(4): 430-437.
-
Elmokadem AH, Abdel-Wahab RM, El-Zayadi AA, Elrakhawy MM (2019) Uterine artery embolization and methotrexate infusion as sole management for caesarean scar and cervical ectopic pregnancies: a single-center experience and literature review. Can Assoc Radiol J 70(3): 307-316.
-
Diagnosis and management of ectopic pregnancy: green- top guideline no. 21 (2016) BJOG 123.
-
Hu J, Tao X, Yin L, Shi Y (2016) Successful conservative treatment of cervical pregnancy with uterine artery embolization followed by curettage: a report of 19 cases. BJOG 3: 97-102.
-
Jurkovic D, Hacket E, Campbell S (1996) Diagnosis and treatment of early cervical pregnancy: a review and a report of two cases treated conservatively. Ultrasound Obstet Gynecol 8(6): 373-380.
-
Chrestiana D, Cheng AB, Panebianco NL, Dean AJ (2014) Pitfalls in cervical ectopic pregnancy diagnosis by emergency medicine physicians using bedside ultrasonography: a case report. Am J Emerg Med 32(4): 397.
-
Surampudi K (2012) A case of cervical ectopic pregnancy: successful therapy with methotrexate. J Obstet Gynecol India 62(S1): 1e3.
-
Taylor JE, Yalcinkaya TM, Akar ME (2011) Successful conservative management of cervical ectopic pregnancy: a case series. Arch Gynecol Obstet 283(6): 1215-1217.
-
Parker VL, Srinivas M (2016) Non-tubal ectopic pregnancy. Arch Gynecol Obstet 294(4): 19-27.
- Genomic Landscape of Aggressive Penile Squamous Cell Carcinoma including TERT-p and NOTCH1 Mutations – An Institutional Experience
- Establishment of Baseline Haematological Values for Canine Population in North-Central Nigeria: A Cross-Sectional Study in the Federal Capital Territory
- Biochemical Assessment of Uroliths Extracted in Patients with Urolithiasis in a Tertiary Health Institution
- Update on Gastrointestinal Pecomas: Molecular Pathogenesis and Risk Stratification
- A Comparative Study of Serum C-reactive Protein Level Between Pre-eclampsia and Normal Pregnancy in Tertiary Level Hospital
- From Deformity to Alignment: Clinical Outcomes of the Schnepp Osteotomy in Hallux Valgus in 47 Feet