Leydig Cell Tumor of Ovary Non-Hilar Type: An Uncommon Histopathological Variant - Case Report and Literature Review
Leydig cell tumor originates from the hilum of the ovary, but a small number of them can be found in the ovarian cortical stroma with the latest known as non-hilar type. We report a case of a 45-year-old postmenopausal woman who presented with a history of virilization, polymenorrhea, dysmenorrhea, dysfunctional uterine bleeding of 6 month duration. On ultrasonography abdomen-pelvis showed bulky uterus with intramural fibroids along with a right ovary measured 2.8 x 2 x 1 cm showed nonspecific well-defined, solid mass with tiny cyst. She underwent an exploratory laparatomy, total hysterectomy with bilateral salpingo-oophorectomy. The gross and microscopic evaluation diagnosed as non-hilar Leydig cell tumor of right ovary. We report a rare case of a Leydig cell tumor - non- hilar type of right ovary for its clinical, radio imaging and histomorphological features.
Introduction
The recent World Health Organization classification of tumors of female reproductive organs, Hilus cell tumors were classified as a separate entity in the category of Sex Cord-Stromal Tumors (SCST) - pure stromal tumors [1].
Leydig cell tumors are rare, sex-cord stromal tumors. They account for 0.1% of ovarian tumors. The majority of these tumors are unilateral [2]. These are almost always benign in nature. There are approximately 150 reported cases of Leydig cell ovarian tumors in the literature to date [3, 4].
Leydig cell tumors of the ovary may produce androgens and cause virilization. The diagnosis is challenging and requires is proper clinical history, laboratory findings, histomorphological features and imaging.
We report a case of a 45-year-old postmenopausal woman who presented with a history of acne, increased muscle bulk, balding, virilization, polymenorrhea, dysmenorrhea, dysfunctional uterine bleeding of 6 month duration.
On ultrasonography abdomen-pelvis showed bulky uterus with three hypo echoic lesions, larger measuring 5.2x.5x3.5 cm, reported as intramural fibroid. The right ovary measured 2.8 x 2 x 1 cm showed nonspecific well-defined, solid mass with tiny cyst. The left ovary was 2.0 x 1.5 x 1 cm with 1cm cystic lesion.
The patient had increased levels of serum total testosterone 240 ng/dL (normal range, <41 ng/dL), free testosterone 5.10 ng/mL (normal range, 0.10–4.70), and a normal level of dehydroepiandrosterone sulfate 48 ug/dL (normal range, 26–460).
She underwent an exploratory laparatomy, total hysterectomy with bilateral salpingo-oophorectomy. Following the surgery, her hirsutism gradually disappeared and serum testosterone were of normal levels.
Gross Examination
We received specimen of uterus with cervix with bilateral fallopian tubes and ovaries. Uterus with cervix measures 9.5 x 7 x 6 cm and weighs 190 gm. External surface of uterus shows subserosal bulge measuring 2.5 cm in maximum diameter. Cut section was grey white, firm and showed whorled appearance. External surface of cervix appears unremarkable. On cut section endometrial canal measures 6 cm. Average endometrial thickness is 0.2 cm. Wall of uterus shows three intramural fibroids. Largest fibroid measures 3.5 cm in maximum diameter. Cut section of which is grey white and firm and shows whorled appearance. Average
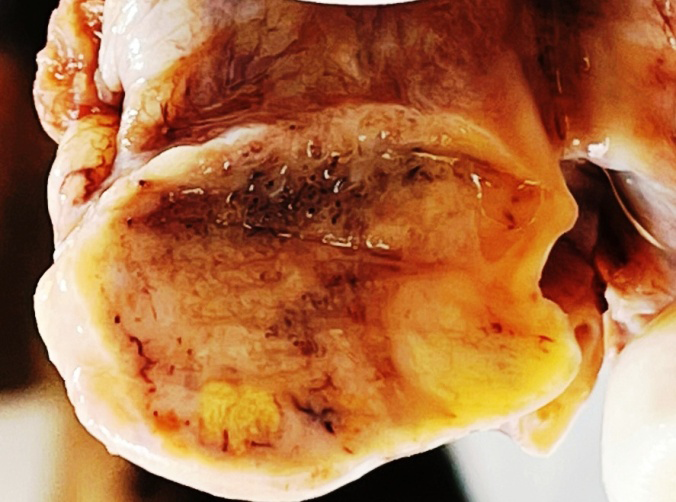
myometrial thickness is 2.7 cm. The cervical canal measures 2 cm in length. The right ovary measures 3 x 2 x 1 cm and cut section shows a circumscribed, encapsulated solid mass with smooth and lobulated external surface. Solid area measuring 1.4 x1.2 x 0.8 cm, cut surface was red-brown to yellow. and a cyst measuring 1.2 in maximum diameter. The right sided fallopian tube with attached fimbriae is 3.5 cm long and cut section dilated. The left sided ovary measures 2.5 x 1.5 x 1 cm and cut section shows serous fluid. The left sided fallopian tube with attached fimbriae is 2.5 cm long and cut section is dilate.
Microscopic examination reported as Leydig cell tumor - Non hilar type of right ovary, other findings were disordered proliferative endometrium, intramural leiomyomas with increased cellularity, hyaline and myxoid change, simple cyst - left ovary and hydrosalpinx of bilateral fallopian tubes, chronic non-specific cervicitis. We report a rare case of a Leydig cell tumor - Non hilar type of right ovary for its clinical, radioimaing and histomorphological features.
Discussion
Leydig stromal cell tumor are rare ovarian tumor that belongs to the group of sex-cord stromal tumors. Hilus or Leydig cell tumors are included in the WHO classification under the heading of “Steroid Tumors” Leydig cell tumors typically occurring in postmenopausal women. They cause hirsutism and virilization in 75% of cases. In addition, approximately 10–20% are also associated with some degree of estrogenic effect such as endometrial hyperplasia [5, 6].
Scully described a distinctive form of lipid cell tumor which closely resemble the stromal luteoma includes all neoplasms that are composed exclusively of cells with structural features common to adrenal cortical cells, Leydig cells, luteinized ovarian stromal cells, and luteinized theca interna cells [7]. Leydig cell tumors is distinguished from a stromal luteoma by the presence of characteristic crystalloids of Reinke within the tumor cells.
Leydig stromal tumor accounts for less than 0.1% of all ovarian tumors [8]. In most patients the etiology of Leydig cell tumor is unknown. Few cases sporadically observed mutations in the fumarate hydratase gene, while few cases area associated with hereditary leiomyomatosis and renal cell carcinoma syndrome. The Leydig cell tumor tumors are generally associated with a benign course. When hyperandrogenism with rapid progression or with signs of virilization an androgen-secreting tumor, origin from the adrenal glands, ovaries, or be ectopic are suspected.
Proper evaluation of women with postmenopausal hyperandrogenism requires a specific investigation protocol. The combined ovarian and adrenal venous blood sampling is a useful method to determine the site of androgen secretion. New-onset virilization in a postmenopausal woman is usually of acute or sub acute onset and is almost always due to tumors of the ovary than adrenal.
There is increased production of testosterone leading to hyperandrogenism and virilization. It shows clinical effect like growth of facial and body hair, voice deepening, clitoromegaly, hirsutism, breast atrophy, increased muscle mass in woman who are mostly postmenopausal [8].
Bancos I et al, observed that about 30% of patients may have endometrial hyperplasia and dysfunctional uterine bleeding. In our case patient presented with dysfunctional uterine bleeding [9]. Muechler EK reported a case of a hilar cell tumor resulting in erythrocytosis and bilateral deep venous thrombosis. [10].
These tumors are typically very small. These tumors are unilateral and confined to the ovary in about 90% of cases. Tumors are well-circumscribed with a smooth lobulated outer surface, homogenous, solid, firm, tan-yellowish on cut surface. In our case tumors are unilateral and confined to the ovary (Figure 1).
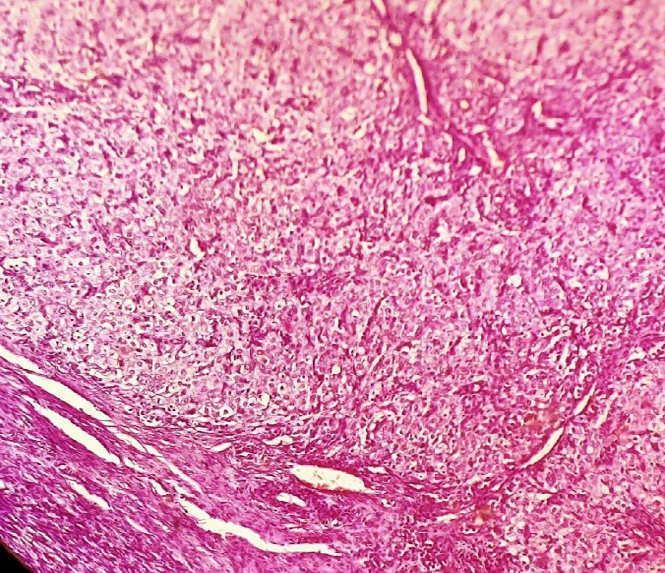
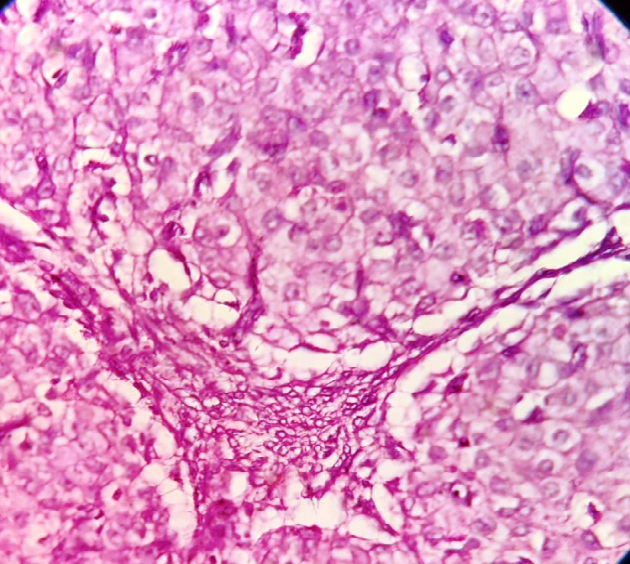
On histopatholical examination tumor is composed of nodules of leydig cells with a neoplastic stromal proliferation. The tumor is composed of Leydig cell which are arranged in diffuse sheets. The neoplatic cells are of uniform round or polygonal cells with abundant eosinophilic cytoplasm. The nuclei are round, uniform, having prominent central nucleoli (Figures 2 & 3) there is no cellular atypia. The mitotic activity is not increased. The stromal component resembles the theca cell tumor, and the presence of crystals reinke: cylindrical crystalloid eosinophilic cytoplasmic bodies in the leydig cells. The tumor cells are surrounded by delicate vasculature. The lipid-rich Leydig cell tumors have finely vacuolated or foamy cytoplasm. Other histomorphological patterns include pseudoglandular, spindle insular, nested, trabecular, ribbon-like, and microcystic.
In histopathological reporting carefully look for the features of malignancy in Leydig cell tumors. These are cells showing nuclear atypia, large tumor size, infiltrative margins, evidence of necrosis and increased mitoses (>3/10 HPF).In our case there were no any features of malignancy.
The ovarian leydig cell tumors are of hilar, non hilar, leydig cell not otherwise specified . The hilar leydig cell tumors arise in the hilus from hilar leydig cells mostly (80%). Other leydig cells tumors that are located within the ovarian stroma are referred to as non hilar leydig cell tumors. While the term leydig cell not otherwise specified is used when it is uncertain about the origin [11]. Non-hilar Leydig cell tumors, as in our patient, occur in ovarian cortical stroma and can be difficult to distinguish from other stromal tumors.
Hilus cell tumors may be associated with other female genital tract’s benign and malignant neoplasms such as granulosa cell tumor of the ovary, polycystic ovaries, leiomyoma uterus, endometrial adenocarcinoma etc [12]. The differential for Leydig cell tumor are hyperplastic/ hamartomatous nodules. It is observed in Klinefelter syndrome, adrenogenital syndrome, elevated gonadotropin levels Nelson syndrome etc. Other differential are stromal luteoma, stromal hyperthecosis, fibrothecoma, Leydig cell hyperplasia [13, 14]. Leydig cell tumors on immunochistochemistry are -alpha, calretinin, CD56, and vimentin positive.
A mutation in the DICER1 gene is associated with Sertoli- Leydig tumors as noted in recent data that indicate germline or somatic mutations in some genes are responsible for the development of some types of sex cord-stromal ovarian tumors [15].
The surgical resection of ovary is treatment for the sex cord –stromal ovarian tumors [16]. In patient who wants preserve their fertility conservative surgery with unilateral salpingo-oophorectomy is choice. The abdominal hysterectomy and bilateral salpingo-oophorectomy should be performed for the bilateral ovarian involvement, and patient who patient does not want to preserve her reproductive potential. On follow up our case showed well response to treatment.
Conclusion
Leydig cell tumors are rare, challenging to diagnose, and should be considered in the differential for virilizing symptoms in postmenopausal women. The histomorphological features play important role. Leydig cell tumors are rare, usually small size, seen in elderly women and having excellent prognosis. We report a rare case of a Leydig cell tumor - non- hilar type of right ovary for its clinical, radio imaing and histomorphological features.
References
-
Kurman RJ, Carcangiu ML, Herrington CS, Young RH (2014) WHO Classification of Tumours of Female Reproductive Organs. Lyon: IARC Ed 4th, 1st (vol).
-
Crum CP, Nucci M R, Lee K (2001) Diagnostic Gynecologic and obstetric pathology. 2nd (edn). Elsevier, saunders pp: 938-945.
-
Rothman MS, Wierman ME (2011) How should postmenopausal androgen excess be evaluated?. Clin Endocrinol (Oxf) 75(2): 160-164.
-
Pelusi C, Forlani G, Zanotti L, Gambineri A, Pasquali R (2013) No metabolic impact of surgical normalization of hyperandrogenism in postmenopausal women with ovarian androgen-secreting tumours. Clin Endocrinol (Oxf) 78(4): 533-538.
-
Pugeat M, Raverot G, Plotton I, Mirakian P, Dechaud H, et al. (2006) Androgen-secreting adrenal and ovarian neoplasms. In: Azziz R, Nestler JE, Dewailly D, eds. Androgen excess disorders in women. 2nd ed. Totowa, NJ: Humana Press: 75-84
-
RussellP, Robboy SJ Prat J (2002) Sex cord-stromal and steroid cell tumours of the ovaries. In: Robboy SJ, Anderson MC, Russell P eds. Pathology of the Female Reproductive Tract. 2nd ed. London, UK, Elsevier 625- 627.
-
Scully RE (1964) Stromal luteoma of the ovary. A distinctive type of lipoid-cell tumor. Cancer 17(6): 769- 778.
-
Nardo LG, Ray DW, Laing I, Williams C, McVey RJ, et al. (2005) Ovarian Leydig cell tumor in a peri- menopausal woman with severe hyperandrogenism and virilization. Gynecol Endocrinol 21(4): 238-241.
-
Bancos I, Prawius, Herbert D (2008) Leydig cell tumor of the ovary in a postmenopausal woman presenting with virilization. The Endocrinologist 18(3): 146-149.
-
Muechler EK (1977) Testosterone-producing ovarian tumor associated with erythrocytosis, hyperuricemia, and recurrent deep vein thrombosis. Am J Obstet Gynecol 129(4): 467-469.
-
Magyar E, Kisfaludy N (2002) Leydig cell tumors not classified as Sertoli-Leydig group. CME Journal of Gynecologic Oncology 7: 164-166.
-
Jagtap S, Beniwal A, Shah H, Kshirsagar N, Jagtap SS (2015) Endometrial carcinoma associated with bilateral ovarian adult granulosa cell tumor: synchronous malignancy. Indian Journal of Pathology 4: 77-79.
-
Young RH (2018) Ovarian sex cord-stromal tumours and their mimics. Pathology 50(1): 5-15.
-
Jagtap SV, Kshirsagar N, Jagtap SS, Singh R, Mittal S (2021) Ovarian fibrothecoma: presented as a large pelvic mass. Int J Health Sci Res 11(3): 145-148.
-
Macut D, Ilić D, Mitrović Jovanović A, Macut JB (2019) Androgen-secreting ovarian tumors. Front Horm Res 53: 100-107.
-
Colombo Ni, Parma GA (2005) Ovarian sex cord-stromal tumors. In: Gershenson DM, Mcguire Mc, Gore M, Quinn MA, Thomas G, editors. Gynecologic Cancer. Elsevier pp. 503-507.
- Genomic Landscape of Aggressive Penile Squamous Cell Carcinoma including TERT-p and NOTCH1 Mutations – An Institutional Experience
- Establishment of Baseline Haematological Values for Canine Population in North-Central Nigeria: A Cross-Sectional Study in the Federal Capital Territory
- Biochemical Assessment of Uroliths Extracted in Patients with Urolithiasis in a Tertiary Health Institution
- Update on Gastrointestinal Pecomas: Molecular Pathogenesis and Risk Stratification
- A Comparative Study of Serum C-reactive Protein Level Between Pre-eclampsia and Normal Pregnancy in Tertiary Level Hospital
- From Deformity to Alignment: Clinical Outcomes of the Schnepp Osteotomy in Hallux Valgus in 47 Feet