HPV Genotype Distribution and Correlation with Age in Women Before and After Leep- Conization and Evaporation in a Single Hospital in Japan
Persistent infection with high-risk (HR) human papillomavirus (HPV) is the major cause of uterine cervical cancer. Most Japanese women have not been vaccinated. The aim of the present study was to assess the prevalence of HPV genotypes and the relationship between HPV genotype and age in cervical intraepithelial neoplasia (CIN) in Japan. Also, we aimed to clarify the HR- HPV clearance and persistence status after loop electrosurgical excision procedure (LEEP) and evaporation. In LEEP and evaporation cases, HPV tests were examined at 1.5 and 6 months later. Of 1070 CINs, 111 were positive for HR-HPV (10.3%). The ratios of HR-HPV and highly progressive HPV in CIN2+ patients in their 20’s and 30’s were significantly higher than those in patients in their 60’s and 70’s. Forty-seven CIN2+ patients were treated with LEEP and evaporation. Twentyseven of these patients (57.4%) were negative for HR-HPV at 1.5 months later and 37 (78.7%) were negative 6 months later. The ratios of HR-HPV in CIN2+ patients in younger patients were significantly higher than those in elder. Adding evaporation to LEEP tended to improve the HPV elimination rate.
Introduction
Human papillomavirus (HPV) infection is the major cause of uterine cervical cancer [1]. Among high risk (HR) HPVs, the risk of developing cervical cancer depends on HPV detected [2]. HPV typing test results are considered useful for risk assessment during the follow-up of cervical intraepithelial neoplasia (CIN) 1/2 patients [3]. Based on the results of a meta-analysis of major HPV studies in Japan, it is estimated that 7 types of HPV 16, 18, 31, 33, 35, 52 and 58, which are frequently detected in invasive cancer, are associated with a high risk of progression [4]. In a follow- up study of 570 CIN1/2 cases conducted in Japan, it was reported that in cases that are positive for one of the above seven types, CIN is significantly less likely to disappear and more likely to progress to CIN3 [5]. In Japan, the detection rate of HPV45 in cervical cancer is extremely low [4], while in other countries, the detection rate is the second highest after HPV16 and 18 [2]. Thus, HPVs 16, 18, 31, 33, 35, 45, 52 and 58 should be managed separately from other HR-HPV types in Japan.
Several studies have shown that the HPV genotype distribution is age-related, regardless of the presence or absence (HPV infection alone) in uterine cervical lesions [6, 7]. The incidence of several types of HR-HPV, including HPV16, decreases with age, whereas other genotypes, such as HPV 33, 35 and 58 increase [8, 9]. Natural history research has focused on detailed aspects of viral and host interactions, such as viral persistence and the duration of infections, the identification of intermediate biomarkers, and the notion that viral latency and the prognosis might be significantly linked to the HPV type [10]. Despite the considerably elevated incidence of HPV infection, there is a strong rate of spontaneous clearance, reaching 77% within the first year and 93% in the following five years [11]. The persistence of HPV infection is required to initiate the oncogenic process in the uterine cervix. Clearance of the infection is more common in young adults than in elderly individuals [12]. Viral load and HPV type are the main cofactors for progression from infection to CIN [1].
For the treatment of CINs, loop electrosurgical excision procedure (LEEP), large loop excision of the transformation zone (LETZ), conization by cold knife, cryotherapy, laser treatment, interferon-alpha, therapeutic vaccination photodynamic therapy (PDT), and their combinations have been reported [12]. LETZ or LEEP with subsequent CO2 laser evaporation for surrounding area after local treatment have been reported to be associated with slightly higher clearance rates in comparison to other methods [12]. Therefore, as the main treatment in this study, we selected LEEP and subsequent evaporation of the surroundings as a less invasive and simple method.
In Japan, the HPV vaccine was routinely administered in 2013, but the active recommendation was discontinued due to side effects [13], and the active recommendation was resumed in 2023; thus, at the time of writing this report, most Japanese women have not been vaccinated. The aim of the present study was to assess the prevalence of HPV genotypes and the relationship between HPV genotype and age in CINs in a single hospital, Gujo City Hospital, in Gujo City in Japan.
Subjects and Methods
Cytology
First, cervical cytology was performed as resident screening. All specimens were stained using the Papanicolaou method.
The final cytological diagnosis was made using the Bethesda system, as follows:
- Normal or Inflammatory
- Atypical Squamous Cell Undetermined Significance (ASC-US)
- Low-Grade Squamous Intraepithelial Lesion (LSIL)
- High-Grade Intraepithelial Lesion (HSIL)
- Atypical Squamous Cells that Could not Exclude High- Grade SIL (ASC-H).
Case Selection
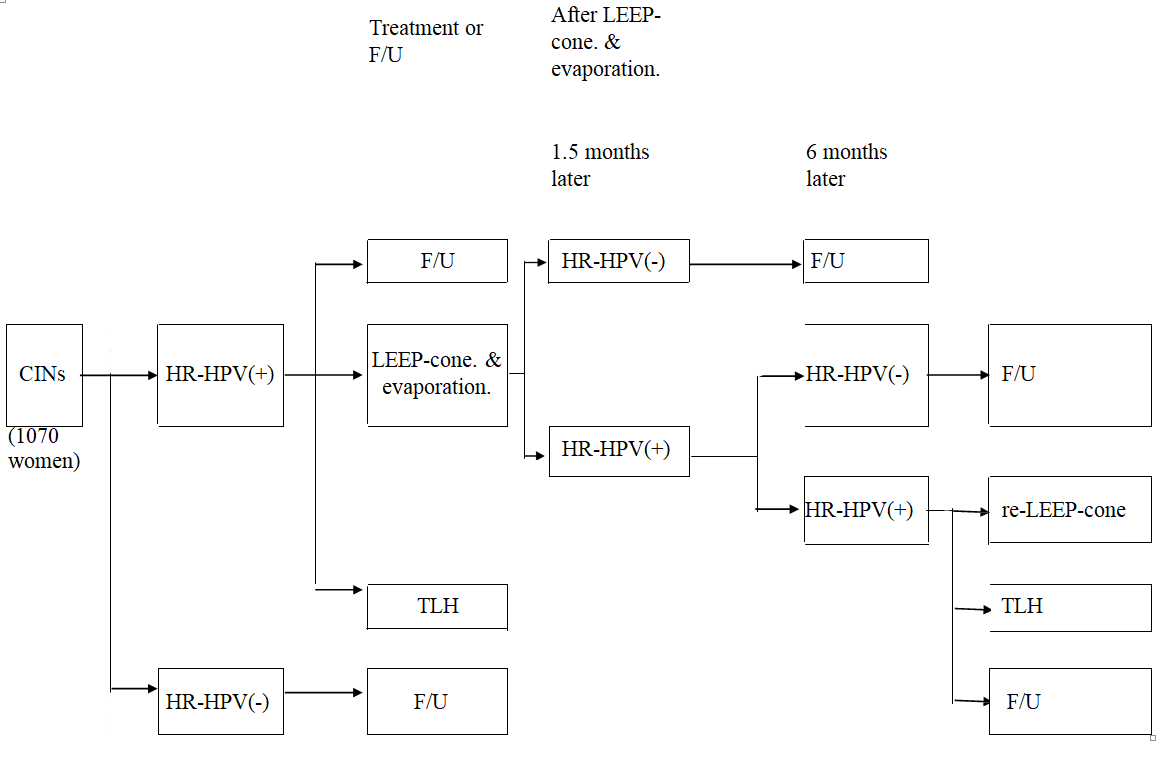
The study design is illustrated in (Figure 1). According to the cervical cancer screening system, patients with ASC-US underwent HPV genotype testing, and those with HR-HPV, LSIL, HSIL, and ASC-H underwent colposcope (DZ-C100, CASIO Co. LTD., Japan)-targeted biopsy in the Department of Obstetrics and Gynecology of the Gujo City Hospital from January 2013 to June 2023. The histological diagnosis of the uterine cervix was performed according to the WHO criteria for cervical intraepithelial neoplasia (CIN) 1 and CIN2/3 [14].
HPV Detection
HPV typing was performed on cervical samples in which CINs was diagnosed histopathologically by targeted biopsy under colposcopy. Cases in which HPV testing was performed several months or years after the 1st pathological diagnosis of CIN were included. HPV typing tests were performed at SRL Inc. (Tokyo), fundamentally using the Luminex × MAP method [15]. A copy number of ≥1,000 was considered positive. This could detect HPV16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59 and 68. Of these, HPV 16, 18, 31, 33, 35, 45, 52 and 58 have been reported to be frequently detected in invasive cancer based on the results of a meta-analysis of major HPV studies in Japan [12, 14]; thus, these types are associated with highly progressive HPV. HPV genotyping was performed at 1.5 months after treatment, when the wound had completely healed, and at 6 months after LEEP- conization and evaporation in cases that were positive a 1.5 months.
HPV Genotyping and Age Correlation
Of the 1070 patients, 111 were classified into the high- risk (HR)-HPV group (Table 1). Patients with CIN1 and CIN2+ HR-HPV and highly progressive HPV were compared every 10 years. Fisher’s exact probability test was used to compare the groups.
| High progression risk group | 16, 18, 31, 33, 35, 45, 52, 58 |
| Other high risk group | 39, 51, 56, 59, 68 |
Table 1: High progression risk group and others in HR-HPV- typing test.
LEEP and Evaporation
Before starting LEEP, the cervical lesions were reconfirmed using colposcopy. The uterine cervix was exposed using a speculum under intravenous anesthesia with pentazocine and thiamylal sodium, and local anesthesia with lidocaine. The LEEP was performed using a high-frequency electrical generator. The loop was selected based on the size of the excised area (Megadyne Medical Products Inc., Draper, UT, USA). Lesion’s margin of ≥5 mm was resected with a 60 W continuous wave. After excision, hemostasis was achieved using a ball electrode (ERBE Electromedical GmbH, Germany) with a 40 W continuous wave. Furthermore, the area around the excised lesion was evaporated (lightly burned) using the same ball electrode as widely as possible. LEEP specimens were anatomically oriented, pinned to a cork board, and fixed in 10% buffered formalin. The final histological diagnoses of the uterine cervix were performed according to the WHO criteria: cervical intraepithelial neoplasia (CIN) 1 and CIN2/3 [14]. Most CINs were immunohistochemically stained for p16 (clone E6H4, Roche Diagnostics, Basel, Switzerland), according to the manufacturer’s protocol [16].
Results
HPV Distribution
Of the 1070 CIN cases tested for HR-HPV, 111 were HPV-positive (10.3%). Of the 111 HR-HPV- positive cases, 82 had highly progressive HPV (73.9%). The ratio of highly progressive HPV to HR-HPV in each age group was the highest in the 20s, and tended to decrease as age increased. The ratios of HR-HPV and highly progressive HPV for CIN1/ CIN2+ in each age group are shown in (Figure 2). The ratios of HR-HPV and highly progressive HPV for CIN2+ in patients in their 20s were significantly higher in comparison to patients in their 60s and 70s (P<0.001). Furthermore, the ratios in patients in their 30s were significantly higher than those in patients in their 60s and 70s (P<0.001 and P<0.05, respectively).
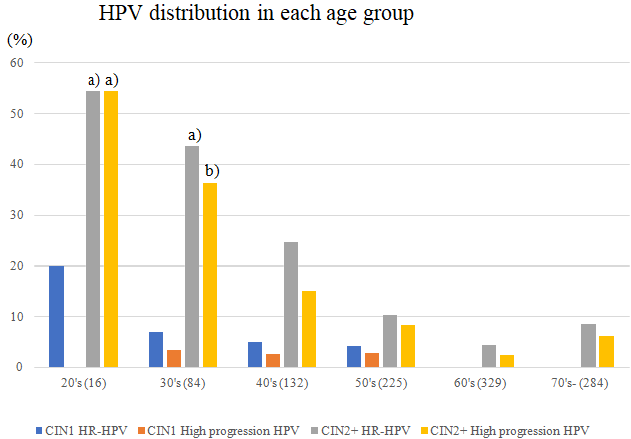
Figure 2: The distribution of HR-HPV and highly progressive HPV in each age group. The ratios of HR-HPV and highly progressive HPV in CIN2+ in their 20s were significantly higher in comparison to those in their 60s and 70s (P<0.001). The ratios of HR-HPV and highly progressive HPV in CIN2+ patients in their 30s were significantly higher in comparison to those in their 60s and 70s (P<0.001 and P<0.05, respectively).
Follow-Up Cases
Three patients with CIN1 and 19 patients with CIN2+ were followed up without treatment at the patients’ request (Table 2). These cases were followed up with routine cytology and colposcopy every 6 months during the year. CIN persisted in all cases, but no cases worsened (Table 2). Some patients underwent additional HPV testing, which yielded negative results.
| Number of Cases | Follow up Period (Yr) | Aggravation | |
|---|---|---|---|
| CIN1 | 3 | 4.0 ± 4.2 (1 ~ 10) | none |
| CIN2+ | 19 | 4.8 ± 2.3 (1 ~ 8) | none |
Table 2: Untreated follow-up cases with HR-HPV positive CIN1 and CIN2+.
LEEP- Conization and Evaporation Cases
Figures 3 & 4 show characteristic case. Cytological examination revealed ASC-H (Figure 3a). A colposcope- targeted biopsy showed CIN3 (Figure 3b) and p16 positivity, suggesting HPV infection (Figure 3c). This case was HPV31- positive. Figure 4a shows a schematic diagram of the LEEP conization and avaporation. Before LEEP conization, colposcopic findings showed a thickened white epithelium with coarse punctures (Figure 4b). Figure 4c shows the findings after hemostasis with LEEP conization. The area around the excited lesion was evaporated as widely as possible with the same ball electrode (Figure 4d). The cut
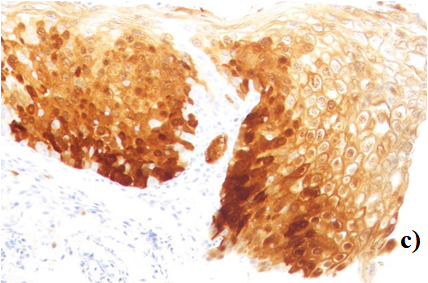
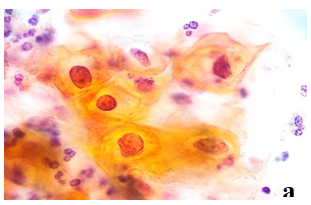
edge was negative, and the final pathological diagnosis was CIN3. After 1.5 months, an HPV test was negative.
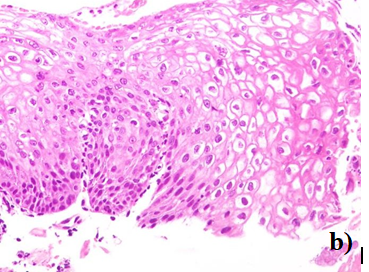

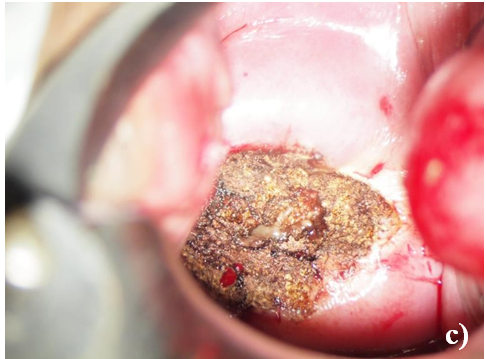
Figure 4: a. Shema of LEEP conization and evaporation. The cut line is indicated by a light blue dot line. The evaporation sites are indicated by blue dots. b. Before LEEP-conization, colposcopy findings showed thickened white epithelium with coarse punctation. c. Findings after hemostasis with LEEP conization. d. The area around the excised lesion was evaporated with the same ball electrode as widely as possible.

Forty-seven CIN2+ patients were treated with LEEP- conization and evaporation. All cases were negative at the cut-edges and cytologically NILM 1.5 months later. Twenty- seven of 47 (57.4%) were negative for HR-HPV 1.5 months later and 37 of 47 cases (78.7%) were negative for HR-HPV 6 months later. The mean age of patients in each subgroup is shown in (Table 3).
| 1.5 months later | 6 months later | |
|---|---|---|
| CIN2+ (47) | clearance | clearance |
| (48.0 y.o.) | 57.4% (27) | 78.7% (37) |
| (46.7 y.o.) | (45.5 y.o.) | |
| persistence | persistence | |
| 44.4% (20) | 22.2% (10) | |
| (49.9 y.o.) | (57.4 y.o.) |
Table 3: HR-HPV clearance and persistence status after LEEP-cone & evaporation.
Five of the 10 CIN2+ cases with HR-HPV underwent total laparoscopic hysterectomy (TLH) at the patient’s request. The other five cases were followed-up by cytology and colposcopy every 6 months.
Only one patient had been vaccinated against cervical cancer (Cervarix® against HPV 16 and 18); unfortunately, she had HPV31 and developed CIN3. All other cases were unvaccinated.
TLH cases
TLH cases there were 14 cases of TLH due to complications such as uterine fibroids.
Discussion
The rate of HR-HPV positivity in CIN1 and CIN2+ cases was much lower in comparison to previous reports (approximately 60%) [12]. This might be related to the inclusion of cases in which HPV testing was performed several months or years after the pathological diagnosis of CIN was made. HPV prevalence declines over time, both before and after treatment [12]. There is also a report that only HPV other than so-called HR-HPV was detected in CIN3 [17]. It is possible that HPV other than HR-HPV was involved in the CINs in this study. Other possible carcinogenic HPV subtypes were not included in the clinical HPV tests in this study, which accounts for the small gap in missed CIN2+ in clinical HPV screening [18]. True HPV-negative CIN2+ is exceedingly rare. In addition to the expansion of HPV testing to include more possibly carcinogenic HPV subtypes, vaccination against possibly carcinogenic HPV subtypes may further reduce the development of cervical cancer.
Three cases of CIN1 and 19 cases of CIN2+ were followed- up for 1-10 years without any treatment; however. None of the cases worsened. HPV infection is often transient, and even cases with CIN may be negative for HPV [10]. It has also been reported that HPV infection become negative over time [12].
Regarding the evaluation of HPV distribution depending on patient age, it has been reported that in non-vaccinated areas, the ratio of HR-HPV (represented by HPV16/18) in CIN3 cases decreased with age, whereas the ratio of other HPVs showed a relative increase [17]. In our CIN2+ data, a tendency for the proportion of highly progressive HPV among HR-HPV to decrease with age was observed. It could be said that the younger age group had a higher rate of involvement with typical highly progressive HPV, and the rate of involvement of other types of HPV increased with age.
Although the estimated post-treatment HPV persistence appear to be somewhat higher for studies utilizing HC2 alone in comparison to PCR alone, there have been an increasing number of reports using the PCR method [12]. In the present study, the persistence rates were 44.4% at 1.5 months later and 22.2% at six months later. The median HPV persistence estimate in five studies that used with PCR-based detection was 26% at 6 months. It has been reported that the HPV persistence rate after 6 months is lower with LEEP, CO2 vaporization, and large loop excision of the transformation zone (LLETZ) with wide excision. The LEEP and evaporation method that we applied had a minimal resection area did not require the use of a special laser ablation device, produced an effective therapeutic effect, and tended to be associated with a low rate of HPV persistence at 6 months after treatment [12]. The mean ages of patients with persistent HPV at 1.5 and 6 months were 49.9 and 57.4 years, respectively. The HPV persistence rate tends to increase with age. Although spontaneous elimination has been reported [10], our findings suggest that the addition of evaporation to LEEP could improve the HPV elimination rate, as suggested by our findings.
Conclusion
Of the 1070 CIN cases tested for HR-HPV, 111 were HR- HPV positive (10.3%). Forty- seven CIN2+ patients were treated with LEEP-conization and evaporation. Twenty- seven of 47 (57.4%) were negative for HR-HPV 1.5 months later and 37 were negative for HR-HPV (78.7%) six months later. The addition of evaporation to LEEP improved the HPV elimination rate.
Acknowledgements
We thank the editor and reviewers for the constructive comments, which helped us improve our manuscript. Part of the cost of this clinical research was supported by the Gifu Prefectural Medical Association’s Working Physician Subcommittee, ``Investigation and research subsidies for the study of medical science, the promotion of medicine, and the improvement of the work environment. This article was approved by all the patient’s verbal consents before writing. Written consent for publication was obtained for cases for which photographs and pathological specimens were provided.
Competing interests
The authors declare that they have no competing interests.
Ethical Approval
Ethical approval for this clinical study was obtained from the ethics committee of our hospital (approval no. 23030601).
References
-
Tao X, Zheng B, Yin F, Zeng Z, Li Z, et al. (2017) Polymerase chain reaction human papillomavirus (HPV) detection and HPV genotyping in invasive cervical cancers with prior negative HC2 test results. Am J Clin Pathol 147 (5): 477-483.
-
Smith JS, Lindsay L, Hoots B, Keys J, Franceschi S, et al. (2007) Human papillomavirus type distribution in invasive cervical cancer and high-grade cervical lesions: a meta-analysis update. Int J Cancer 121(3): 621-632.
-
Wheeler CM, Hunt WC, Schiffman M, Castle PE, Atypical squamous cells of undetermined significance/low- grade squamous intraepithelial lesions triage study group (2006) Human papillomavirus genotypes and the cumulative 2-year risk of cervical precancer. J Inf Dis 194(9): 1291-1299.
-
Miura S, Matsumoto K, Oki A, Satoh T, Tsunoda H, et al. (2006) Do we need a different strategy for HPV screening and vaccination in East Asia? Int J Cancer 119(11): 2713- 2715.
-
Matsumoto K, Oki A, Furuta R, Maeda H, Yasugi T, et al. (2011) Predicting the progression of cervical precursor lesions by human papillomavirus genotyping: a prospective cohort study. Int J Cancer 128(12): 2898- 2910.
-
Baser E, Ozgu E, Erkilinc S, Togrul C, Caglar M, et al. (2014) Risk factors for human papillomavirus persistence among women undergoing cold-knife conization for treatment of high-grade cervical intraepithelial neoplasia. Int J Gynaecol Obstet 125(3) : : 275-278.
-
Park JY, Lee KH, Dong SM, Kang S, Park SY, et al. (2008) The association of pre- conization high-risk HPV load and the persistence of HPV infection and persistence/ recurrence of cervical intraepithelial neoplasia after conization. Gynecol Oncol 108(3): 549-554.
-
Castle PE, Shaber R, LaMere BJ, Kinney W, Fetterma B, et al. (2011) Human papillomavirus (HPV) genotypes in women with cervical precancer and cancer at Kaiser Permanente Northern California. Cancer Epidemiol Biomarkers Prev 20(5): 946-953.
-
Guardado-Estrada M, Juarez-Torres E, Roman-Bassaure E, Medina-Martinez I, Alfaro A, et al. (2014) The distribution of high-risk human papillomaviruses is different in young and old patients with cervical cancer. PLoS One 9(10): e109406.
-
Bosch FX, Burchell AN, Schiffman M, Giuliano AR, de Sanjose S, et al. (2008) Epidemiology and natural history of human papillomavirus infections and type-specific implications in cervical neoplasia. Vaccine 26 Suppl 10: K1-16.
-
Molano M, Van den Brule A, Plummer M, Weiderpass E, Posso H, et al. (2003) Determinants of clearance of human papillomavirus infections in Colombian women with normal cytology: a population-based, 5-year follow- up study. Am J Epidemiol 158 (5) 486-494.
-
Hoffman SR, Le T, Lockhart A, Sanusi A, Dal Santo L, et al. (2017) Patterns of persistent HPV infection after treatment for cervical intraepithelial neoplasia (CIN): A systematic review. Int J Cancer 141(1): 8-23.
-
Ugumori N, Ueda Y, Yagi A, Abe H, Shiomi M, et al. (2021) A potential means to help the HPV vaccine penetrate the Japanese public while under the continued suspension of governmental recommendation. Hum Vaccin Immunother 17(9): 3096-3101.
-
Mills AM, Park KJ, Carriho C, Regauer S, Focci GRA, et al. (2020) Squamous intraepithelial lesions of the uterine cervix. In Herrington CS, Kim K-R, Kong CS, Longacre TA, McCluggage WG, Mikam Lyon, France: IARC, pp. 342-346.
-
Ozaki S, Kato K, Abe Y, Hara H, Kubota H, et al. (2014) Analytical performance of newly developed multiplex human papillomavirus genotyping assay using Luminex XmapTm technology (Mebgen HPV Kit). J Virol Meth 204: 73-80.
-
Nicolas I, Saco A, Barnadas E, Marimon L, Rakislova N, et al. (2020) Prognostic implications of genotyping and p16 immunostaining in HPV-positive tumors of the uterine cervix. Mod Pathol 33(1): 128-137.
-
Giannella L, Giorgi Rossi P, Delli Carpini G, Di Giuseppe J, Bogani G, et al. (2021) Age-related distribution of uncommon HPV genotypes in cervical intraepithelial neoplasia grade 3. Gynecol Oncol 161(3): 741-747.
-
Reich O, Regauer S, Kashofer K (2020) Possibly carcinogenic HPV subtypes are a cause of HSIL and negative clinical HPV tests - A European prospective single center study. Gynecol Oncol 158(1): 112-126.
- Genomic Landscape of Aggressive Penile Squamous Cell Carcinoma including TERT-p and NOTCH1 Mutations – An Institutional Experience
- Establishment of Baseline Haematological Values for Canine Population in North-Central Nigeria: A Cross-Sectional Study in the Federal Capital Territory
- Biochemical Assessment of Uroliths Extracted in Patients with Urolithiasis in a Tertiary Health Institution
- Update on Gastrointestinal Pecomas: Molecular Pathogenesis and Risk Stratification
- A Comparative Study of Serum C-reactive Protein Level Between Pre-eclampsia and Normal Pregnancy in Tertiary Level Hospital
- From Deformity to Alignment: Clinical Outcomes of the Schnepp Osteotomy in Hallux Valgus in 47 Feet