Short Root Anomaly (SRA)/Rhyzomicroly-Report of an Unusual Radicular Anomaly with Comprehensive Literature Review
Dental anomalies are the anomalies involving either crown or root portion of a tooth which may affect size, shape, number, structure and composition of a tooth and can be seen as a part of syndrome or in non-syndromic patients. Anomalies involving root portion of a tooth include different variations like larger size, extra root and extra canals. Short root anomaly is an uncommon root variation characterized by short roots with blunt and closed apices. The purpose of this article is to report an unusual occurrence of short roots involving permanent mandibular molars which is rarely reported so far. Detailed information pertaining to short root anomaly is also discussed in this paper.
Introduction
Short Root Anomaly (SRA) is a rare developmental dental disorder pertaining to anomaly of the root structure and was first mentioned by Volmer Lind to the scientific literature in 1972. Lind named it as short root anomaly or in short, the SR anomaly [1]. In his 1972 research article author has described a method for measuring “the relative root length of the tooth” using radiographs which helps in quantitative comparisons of the roots in clinical cases. He described this abnormal short root morphology mainly in maxillary central incisors with compromised crown to root ratio [1]. Further, Lind carried out clinical, metric and radiographic examinations on 112 children with maxillary central incisors having abnormally short roots and 100 children with normally developed roots which used as a control group. From this study he concluded with following findings.
- The “relative root length” of the maxillary central incisor on an average is 1.6 times that of the length of the crown and the corresponding ratio in children with SR anomaly is 1:1, with no difference in either of sex.
- The shortness of the roots is not due to resorption or to any developmental disturbance of exogenous disruption. The condition is a constitutional anomaly and its prevalence varies with race, sex and hereditary predisposition.
- The SR anomaly is associated with a predisposition to root resorption in the maxillary anterior teeth. [1].
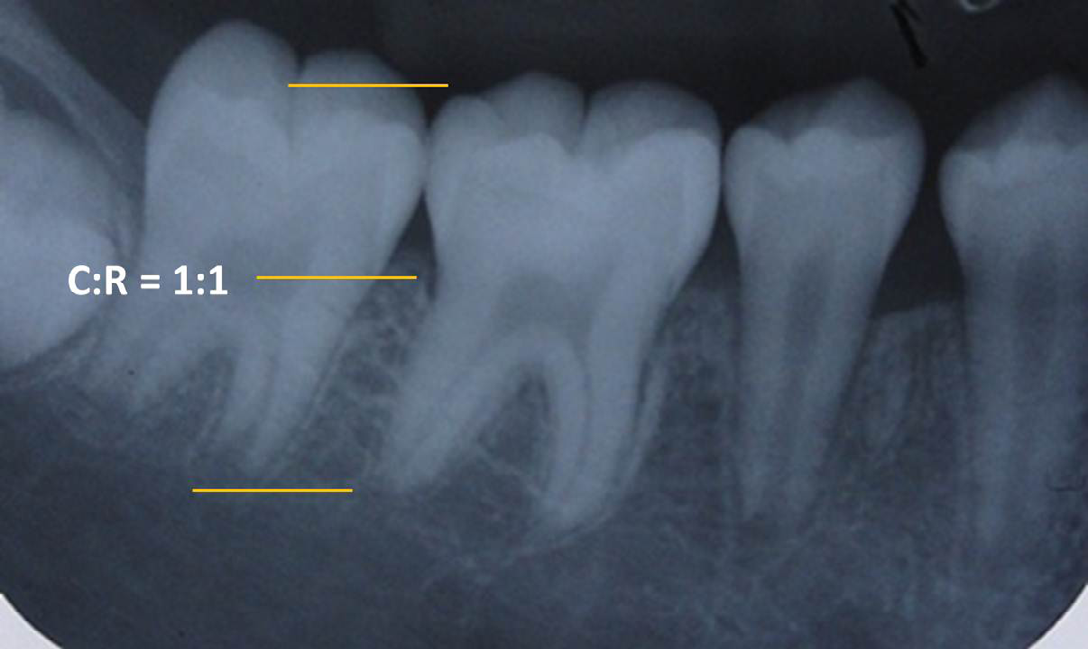
Therefore, based on Lind suggestions, the SR anomaly is characterized by permanent teeth with short and blunt root, closed and round apices with reduced crown to root ratio. The ratio of crown to root (C:R) of the affected tooth usually varies from 1:1 or less. Completely developed roots with closed apices are the typical feature seen in this condition. Unilateral occurrence of SRA is more common compared to bilateral presence and is frequently seen in the maxillary central incisors followed by maxillary premolars and maxillary lateral incisors. Mandibular premolars, canines and molars are the least affected teeth with this condition. When
it occurs bilaterally it commonly involves 2 to 4 teeth affected pair. However, a generalized occurrence involving multiple teeth is rarely reported. Few authors have also referred this condition as hereditary non-syndromic idiopathic root malformation [2, 3]. Extensive search of literature revealed scarcity of data on this anomaly and reports of SRA involving mandibular molars is rarely reported. Although there are reports on generalized occurrence involving multiple teeth [2, 3], but mandibular molars affected with SRA are very less. Hence, the purpose of this article is to show the occurrence of SRA in mandibular molars and also to discuss in detail about its prevalence, etiology, associated pathology, clinical significance, differential diagnosis by comprehensively reviewing the literature pertaining to SRA.
Case Series
SRA was noticed in three pediatric patients who reported to a private dental clinic complaining of pain in the lower right back teeth. Age of the patients ranged from 13 to 15 years. Among three patients, two were females and one male. On physical examination all three patients appeared moderately built, well-nourished with no signs and symptoms of any systemic, metabolic or syndromic features. Medical history in all revealed normal. There was no history of previous trauma or orthodontic treatment in these patients. On intraoral examination all three patients showed complete permanent dentition. The crowns of all three teeth appeared normal in morphology, the surrounding periodontal tissue appeared normal with absence of other dental anomalies. Tooth mobility was also not noticed in all three cases. In two patients, the permanent mandibular right molars were affected with dental caries. One patient exhibited deep pit and fissures in mandibular first molar. An intraoral periapical radiograph was made in all three patients who showed presence of short roots involving only first molars and not involving either second molars or premolars. Radiographic measurement was carried out for all three teeth with short roots which showed crown root ratio of 1:1 along with closed and round root apices (Figures 1-3). The periodontal tissue and the alveolar bone surrounding the short roots appeared normal in architecture. Finally based on clinical, radiographic findings and using literature search, the condition was diagnosed as SRA in all three patients. In first patient, pit and fissure sealant application was done as there were deep non cleansing developmental grooves. In second patient, root canal treatment was planned and in third patient, extraction of the affected tooth was advised as the tooth was in non-restorable condition due to gross destruction of the tooth crown (Table 1).
| Sl. No. | Age / Gender | Tooth found with SRA | Associated signs/symptoms | Associated other dental anomalies | Treatment given |
|---|---|---|---|---|---|
| 1. | 14 years/ Female | Permanent mandibular left first molar (Figure 1) | |||
| 2. | 15 years/ Female | Permanent mandibular right first molar (Figure 2) | Decayed | Root canal treatment | |
| 3. | 13 years/ Male | Permanent mandibular right first molar (Figure 3) | Grossly destructed due to long standing periapical infection | Extraction of the tooth |
Table 1: Detailed description of patients found with Rhizomicroly/SRA.


Discussion
The first report of SRA was found in 19 year old boy having poorly developed dental roots and early exfoliation of the permanent teeth [4]. This condition is the main causes of early exfoliation of teeth and hence early diagnosis highly essential. In this paper, author has made a sincere effort to describe this rare radicular condition in detail pertaining to its all aspects including synonyms, etiology, prevalence, clinical presentation, radiographic presentation and its clinical significance in various specialties of dentistry which is mentioned below in the following paragraphs under subheadings.
Synonyms
Following introduction of SRA to the dental literature by Lind [1], hardly countable number of publications can be seen in the PubMed or Google search. The scientific term given by him is still used and followed in all publications. Author of this paper has studied the literature pertaining to anomalies of roots both in primary and permanent teeth and has published various articles on Radix entomolaris, Radix paramolaris, short root and other dental anomalies [5, 6, 7, 8]. In the English literature, tooth with extremely long roots are referred by a term “Rhyzomegaly” or “Root gigantism” or “Radiculomegaly” [9]. With reference to this, author has given new terms for the tooth with short roots like “Rhyzomicroly” or “Root Dwarfism” or “Radiculomicroly” along with Short root anomaly which was given by Lind.
Prevalence of SRA/Rhyzomicroly
Prevalence of SRA among different ethnic groups has been studied (Table 2). In Swedish children, Jacobson and Lind found 2.4% of SRA in maxillary central incisors. Ando, et al. [10] got 10% prevalence in maxillary central incisors of Japanese school children [11]. In Mongolian population, the reported prevalence was 10% [12] and in Caucasians it varies from 2.4 – 2.7% [13]. In Finnish population the reported prevalence was 1.3% [14, 15, 16]. All these studies have shown that it is three times more common in females compared to males. From Indian context there are no studies showing prevalence of SRA except for few case reports. Therefore, some more future studies investigating the prevalence of SRA in other population around the globe is required.
| Author/Year | Population group | Prevalence (%) |
|---|---|---|
| Jacobson, et al. [10] | Swedish children | 2.4 |
| Ando, et al. [11] | Japanese | 10 |
| Apajalahati et, al. [17] | Mangolian | 10 |
| Apajalahati, et al. [17] | Caucasians | 2.4-2.7 |
| Apajalahati, et al. [13] | Finnish | 1.3 |
| Cutrera, et al. [14] | Hispanic | 10 |
Table 2: Survey of published studies showing prevalence of Rhyzomicroly/SRA.
Clinical presentation of Rhyzomicroly/SRA
On clinical examination, rhyzomicroly affected teeth shows normal size and shape in morphology. Even surrounding tissues with these teeth appear normal and asymptomatic. It is more often diagnosed on routine radiographic examination, as a result, most of the time this condition remain un-diagnosed [1, 2, 3]. In addition to this, it is difficult to diagnose for teeth with short roots in the mixed dentition. However tooth mobility has been reported as a first clinical finding encountered in SRA cases [15]. Therefore proper meticulous early diagnosis of rhyzomicroly by ruling out presence of tooth mobility is very essential for successful management of these cases and from preventing these teeth from early tooth loss. In case of maxillary central incisors, peculiar characteristic root morphology like short roots with “lack of significant tapering towards the root apex” and round apices is been reported. In case of mandibular second premolars less round and blunted apices are noticed. Therefore careful examination is required for not misdiagnosing this clinical condition from root resorption. In all three cases presented here the crown morphology appeared normal except for presence of dental caries in second the third cases. Short roots were accidentally noticed on radiographic examination [6].
Radiographic Presentation of Rhyzomicroly/ SRA
Teeth with rhyzomicroly are accidentally diagnosed on routine radiographic examination as these clinically appear normal in morphology. Radiographically apart from short roots, the pulp chamber, root canals and periodontium appear normal except for few cases reported showing taurodontium [16]. In the cases presented here too the surrounding periodontal tissues and alveolar bone architecture appeared normal except for presence of periapical infection in the third case. The external root resorption arising from periapical infection was ruled out in this case. The resorption pattern in external root resorption exhibit a typical shape in the apical surface of the root compared with SRA. In external root resorption, the apical surface of the resorbed roots depicts irregular and gradual shortening compared to SRA which shows rounded and smooth roots without any resorption [1, 2, 3]. Therefore based on this finding the third case was diagnosed as SRA.
In a recent article published by Trimeridou, et al. [2] short roots were found generalized but surprisingly not involving molars in both maxillary and mandibular arch. Contrary to this in cases described here, the rhyzomicroly was observed only in mandibular molars. Although orthopantomograph was not taken to rule out generalized appearance, but second and premolars were absolutely normal on intraoral periapical radiograph. Therefore this is the unique case showing rhyzomicroly in the permanent mandibular molars.
Etiology
The exact etiology behind occurrence of rhyzomicroly is still not known. It is hypothesized towards idiopathic occurrence. However some authors have stated that this anomaly occurs as a result of impairment in the Hertwig’s epithelial root sheath and apical proliferation during root development of the involved tooth [1]. Root resorption or due to any systemic disorders is also not reported in the literature. However, familial occurrence of this condition in parents and children of the same family has been reported showing it as an autosomal dominance pattern of inheritance [17]. Apajalahti, et al. [17] extensively studied hereditary predisposition of SRA by collecting detailed family data. They finally concluded from their study that an apparent genetic heterogeneity of the pedigree did not reveal definitive conclusions towards mode of inheritance. However, autosomal dominant pattern was observed in 3/8 families. In 2/8 families the disorder was seen in siblings but not in parents. Hence these single cases of SRA indicate that this condition occurs due to fresh mutations [1, 2]. In addition to this an autosomal recessive pattern inheritance has also been reported.[2] Other etiologies like congenital or developmental origin, chemotherapy and radiotherapy and external influences like trauma, syndromes have also been reported [18].
Previous molecular studies show the fragmentation, activation and complex formation of the matrix metalloproteinase 9 (MMP-9) particularly in gingival crevicular fluid (GCF) of rhyzomicroly patients [19]. From this it is confirmed that compared to other MMPs, MMP- 9 has low collagenolytic resorptive activity thereby not causing severe root resorption. Whereas in patients with active periodontitis and gingivitis patients other MMPs present in GCF cause severe root resorption due to high collagenolytic activity [20]. Therefore it is speculated that the rhyzomicroly is a developmentally induced anomaly rather than due to root resorption. One more recent animal research also stated that deficiency of nuclear factor Ic (Nfic) gene causes the development of short and abnormal roots by disturbing odontoblast differentiation, because Nfic gene is significantly responsible for the odontoblast differentiation and for development of root formation [21, 22].
SRA in Association with other Anomalies
Literature shows an association of SRA with other dental abnormalities. There are case reports showing presence of hypodontia [17], obliterated pulp chambers, dens invaginatus and supernumerary teeth, generalized microdontia [15, 16, 17, 18]. Some authors have shown increased tendency of root resorption in SRA cases [20]. In 1999 research work, authors studied series of families for association of various dental anomalies like peg shaped lateral incisors, ectopic eruption, tooth agenesis, supernumerary teeth, taurodontism, dens invaginatus and tendency for root resorption [17]. Authors measured mesiodistal dimensions of the crown in teeth affected with SRA to evaluate any change in increase or decrease in dimensions. They found 46% of tooth agenesis and 33% of ectopic canines along with SRA. Authors have also stressed on the fact of not misdiagnosing this condition with root resorption. Yu, et al. [15] reported a case of generalized SRA in association with other dental anomalies like dens invaginatus and enamel hypoplasia. They also reported peculiar extra-oral finding like bridging of sella turcica. In sella turcica bridging, an excessive calcification of interclinoid ligaments of sella turcica which mostly caused by congenital defects is observed. This condition frequently seen associated with multiple dental anomalies which could be due to sharing of genes and neural crest cells, which are necessary for development and differentiation of both teeth and sella turcica. Leonardi, et al. [23] also reported that early diagnosis of sell turcica bridging in early age will help practitioners to identify possible occurrences of dental anomalies which form later.
Differential Diagnosis of SRA
Reports shows that short roots of teeth are seen in other conditions and hence rhyzomicroly should be carefully differentially diagnosed from other conditions. Short and tapered roots have been reported in those children who had received radiotherapy or chemotherapy for the cancer treatment (head-neck region/ total body) [24, 25, 26]. This may be due to arrested root development and premature apical closure or even complete absence of root development. The more severe developmental anomalies of the roots and teeth are seen in younger children with higher dose of the treatment received. One more clinical condition like dentin dysplasia type I (dd – I), the teeth appear normal in shape and color or opalescent, amber-colored crowns [27]. In patients with dd-I the roots of the teeth appear blunt and short. But the only distinguishing feature from SRA is the presence of obliterated pulp chambers in dd-I cases. In addition an apical radiolucency in absence of caries is also reported in dd-I. Moreover, dd-I is seen both in primary and permanent dentition, in contrast to rhyzomicroly which is reported only in permanent teeth [27]. Presence of previous trauma should also be differentiated from SRA. Mainly root shape should be considered. In traumatized teeth, short roots, thin radicular walls and wide open apex is seen which is due to disturbance and arrest of root growth. Molar incisor malformed hypoplastic teeth (MIMH), a newly researched dental abnormality mainly affects roots of permanent molars and crowns of incisors. This condition too should be differentiated from short roots [28]. In MIMH, affected molars typically exhibit thin, short and divergent hypoplastic roots with narrow slits in the pulp chamber. Clinical symptoms are usually absent in MIMH and a characteristic enamel notch at the cervical third of the tooth crown especially in incisors is seen [28].
SRA in Association with Other Disorders
Short roots are even reported in patients with short stature. Short roots are also reported in some metabolic disorders like Vitamin D-dependent rickets, pseudohypoparathyroidism and hypophosphatasia [29]. Patients with syndromes exhibiting short stature conditions such as Hallerman-Streiff syndrome, Schimcke immune- osseous dysplasia, Stevens-Johnson syndrome, Frazer
syndrome and Turner syndrome have shown short roots in multiple teeth [2, 3, 4, 5, 6, 7, 8, 9, 10]. In thalassemia major patients spiky- shaped short roots along with alveolar bone malformations have been reported [30]. In the three cases presented here, authors did not come across any of the above diseases or syndromic, or metabolic features and medical history in all three patients found uneventful. Moreover history of trauma was also ruled out. So by ruling out presence of all the above factors, the present case was diagnosed as non-syndromic idiopathic rhizomicroly or short root anomaly. Clinical Significance of SRA/Rhyzomicroly in Pediatric Dentistry It is a well-known fact that SRA is a poorly understood developmental radicular anomaly. As a result this disorder significantly affects dental treatment. The presence of SRA has various implications in orthodontics and orthognathic treatment.
a. Orthodontic Implications In patients going for orthodontic treatment the careful evaluation of crown-root ratio of each tooth is essential to rule out iatrogenic root resorption. Therefore use of pretreatment radiographs as baseline or reference points is of more advantageous to evaluate further decrease in root length due to resorption arising from inadvertent orthodontic forces [3]. Ponraj, et al. have advised for use of periodic radiographs mandatorily in every orthodontic patient with SRA to monitor the root resorption of the teeth. Moreover, judicious judgment of risks and benefits is thought before commencing orthodontic treatment as each case of SRA are challenging to an orthodontist. When mobility of the affected tooth or teeth is present, orthodontic treatment is absolutely contraindicated. It is also recommended that use of light forces throughout the treatment with longer intervals in each activations and appointments will definitely give better stability for these teeth with short roots. In cases when mobility is seen with short roots, authors have advised for the use of splints to stabilize the teeth (mainly for incisors) with mobility following an orthodontic treatment. Therefore increased awareness of rhyzomicroly is essential not only for orthodontist but also for oral and maxillofacial surgeons in order to reduce root resorption.
b. Orthognathic implications Both orthodontics and Orthognathic surgery is required for patients with a skeletal discrepancy to achieve best functional and esthetic outcome [3]. Although orthodontic treatment is the first phase of treatment in patients with skeletal discrepancy Orthognathic surgery is always required. Therefore meticulous diagnosis of short roots is not only important for planning of orthodontic treatment planning but also essential for success of Orthognathic surgery.
c. Prosthodontic Implications In patients with rhyzomicroly a fixed prosthesis is usually not recommended if the adjacent tooth with short roots is acting as an abutment [2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18]. Such tooth may not withstand the occlusal forces. Rather a removable appliance can be given. Permanent prosthetic replacement with dental implants is of great option in SRA patients as the alveolar bone is absolutely normal. However, it is mandatory to consider the age of the patients before going for replacement of mobile tooth with short roots using implants.
Conclusion
Rhyzomicroly/SRA is an uncommon radicular anomaly requiring special attention from all specialties of dentistry as presence of short roots poses a challenging situation for every treatment options. Therefore thorough diagnosis using accurate clinical, radiographic and genetic examinations is highly essential to render proper treatment. Future prospective studies are required to evaluate its prevalence in all ethnic groups around the globe. References
1. Lind V (1972) Short root anomaly. Scand J Dent Res 80(2): 85-92.
2. Trimeridou AS, Arhakis A, Arapostathis K (2023) Presentation of a case of short root anomaly in an 11- year old child. Case Report Dentistry 2023: 1766133.
3. Lamani E, Feinberg KB, Kau CH (2017) Short root anomaly-a potential “Landmine” for orthodontic and orthognathic surgery treatment of patients. Ann Maxillofac Surg 7(2): 296-299.
4. Brown H (1944) Hypoplasia of the dentition. Am J Orthod Oral Surg 30(1): 102-103.
5. Nagaveni NB, Umashankara KV (2012) Radix entomolaris and paramolaris in children: A review of the literature. J Indian Soc Pedod Prev Dent 30(2): 94-102.
6. Nagaveni NB, Umashankara KV (2009) Radix entomolaris in permanent mandibular first molars: Case reports and literature review. Gen Dent 57(3): e25-29.
7. Nagaveni NB, Umashankara KV, Radhika NB (2012) A retrospective analysis of accessory roots in mandibular molars of Indian pediatric patients. Int J Dent Anthropol 20: 38-46.
8. Umashankar KV, Radhika NB, Satisha TS (2011) Third root (Radix entomolaris) in permanent mandibular first molars in pediatric patients. An endodontic challenge. J Oral Health Comm Dent 5(1): 49-51.
9. Alhussain M, Almosa N, Alnofaie H (2022) Nonsyndromic generalized radiculomegaly of permanent dentition: A rare case report. Case Rep Dent pp: 3548370.
10. Jakobsson R, Lind V (1973) Variation in root length of the permanent maxillary central incisor. Scan J Dent Res 81(4): 335-338.
11. Ando S, Kiyokawa K, Nakashima T, Shibo K, Sanka Y (1967) Studies on the consecutive survey of succedaneous and permanent dentition in the Japanese children. 4. Behaviour of short rooted teeth in the upper bilateral central incisors. J Nihon University Sch Dent 9(2): 67-82.
12. Puranik CP, Hill A, Henderson Jeffries K, Harrell SN, Taylor RW, et al. (2015) Characterization of short root anomaly in a Mexican cohots-Hereditary idiopathic root malformation. Orthod Craniofac Res 18 Suppl 1: 62-70.
13. Apajalahti S, Holtta P, Turtola L, Pirinen S (2002) Prevalence of short-root anomaly in healthy young adults. Acta Odontol Scand 60(1): 56-59.
14. Cutrera A, Allareddy A, Azami N, Nanda R, Uribe R (2018 ) Is short root anomaly (SRA) a risk factor for increased external apical root resorption in orthodontic patients?. A retrospective case control study using cone beam computerized tomography. Orthod Craniofac Res 22(1): 32-37.
15. Yu D, Kim D (2021) Generalized short root anomaly with various dental anomalies: A case report with a 5 -year follow-up. J Korean Acad Pediatr Dent 48(1): 1226-8496.
16. Desai RS, Vanaki SS, Puranik RS, Rashmi GS, Nidawani p (2006) An unusual combination of idiopathic generalized short-root anomaly associated with microdontia, taurodontia, multiple dens invaginatus, obliterated pulp chambers and infected cyst: a case report. J Oral Pathol Med; 35(7): 407-409.
17. Apajalahti S, Arte S, Pirinen S (1999) Short root anomaly in families and its association with other dental anomalies. Eur J Oral Sci 107(2): 97-101.
18. Venkataraghavan K, Karthik S, Krishnakumar (2014) K Short root anomaly-A rare occurrence: Review of literature and report of a case. Ind J Dent Sci 6(4).
19. Apajalaht S, Sorsa T, Ingman T (2003) Matrix metalloproteinase-2,8,9, and -13 in gingival crevicular fluid of short root anomaly patients. Eur J Orthod 25(4): 365-369.
20. Newman WG (1975) Possible etiologic factors in external root resorption. Am J Orthod 67(5): 522-539.
21. Park JC, Herr Y, Cho MI, Kim HJ, Gronostajski RM (2007) Nfic gene disruption inhibits differentiation of odontoblasts responsible for root formation and results in formation of short and abnormal roots in mice. J Periodontol 78(9): 1795-1802.
22. Huang XF, Chai Y (2012) Molecular regulatory mechanism of tooth root development. Int J Oral Sci 4(4): 177-181.
23. Leonardi R, Barbato E, Vichi M, Caltabiano M (2006) A sella turcica bridge in subjects with dental anomalies. Eur J Orthod 28(6): 580-585.
24. Sonis AL, Tarbell R, Valachovic RW, Gelber R, Schwenn M, et al. (1990) Dentofacial development in long-term survivors of acute lymphoblastic leukemia: a comparison of three treatment modalities. Cancer 66(12): 2645- 2652.
25. Nasman M, Forsberg CM, Dahllof G (1997) Long term dental development in children after treatment for malignant disease. Eur J Orthod 19(2): 151-159.
26. Holtta P, Alaluuasua S, Saarinen-Pihkala M, Wolf J, Nystrom M, et al. (2002) Long –term adverse effects on dentition in children with poor-risk neuroblastoma treated with high-dose chemotherapy and autologous stem cell transplantation with or without total body irradiation. Bone Marrow Trans 29(2): 121-127.
27. Ye X, Li K, Liu L, Yu F, Xiong F, et al. (2015) Dentin dysplasia type I-novel findings in deciduous and permanent teeth. BMC Oral Health 15(163): 163.
28. Lee HS, Kim SH, Kim SO, Lee JH, Choi HJ (2014) A new type of dental anomaly: molar-incisor malformation (MIM). Oral Surg Oral Med Oral Pathol Oral Radiol 118(1): 101-109.
29. Zambrano M, Nikitakis G, Sancheq-Quevedo C, Sauk J, Sedano H, et al. (2003) Oral and dental manifestations of vitamin D-dependent rickets type I: report of a pediatric case. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 95(6): 705-709.
30. Hazza AM, Al-Jamal G (2006) Radiographic features of the jaws and teeth in thalassaemia major. Dento Maxillo Fac Radiol 35(4): 283-288.
- Genomic Landscape of Aggressive Penile Squamous Cell Carcinoma including TERT-p and NOTCH1 Mutations – An Institutional Experience
- Establishment of Baseline Haematological Values for Canine Population in North-Central Nigeria: A Cross-Sectional Study in the Federal Capital Territory
- Biochemical Assessment of Uroliths Extracted in Patients with Urolithiasis in a Tertiary Health Institution
- Update on Gastrointestinal Pecomas: Molecular Pathogenesis and Risk Stratification
- A Comparative Study of Serum C-reactive Protein Level Between Pre-eclampsia and Normal Pregnancy in Tertiary Level Hospital
- From Deformity to Alignment: Clinical Outcomes of the Schnepp Osteotomy in Hallux Valgus in 47 Feet