Gaint Coronary Artery Aneurysm Presenting with the Acute Coronary Syndrome
Raghu TR and Manjunath CN
Sri Jayadeva Institute of Cardiovascular Sciences and Research, India
080-22977261, Email: drnatrajsetty75@gmail.com
Introduction
The incidence of coronary aneurysms varies from 1.5% to 5% of cases at angiography [1]. The primary complications are ischemia and infarction due to thrombosis or dissection. Spontaneous rupture is rare. The presence of coronary aneurysms, with or without obstructive disease, is an independent risk factor for death [2].
A 72 years old male, hypertensive and diabetic presented to casualty with a history of chest pain, shortness of breath NYHA class II of one-day duration. His electrocardiogram (ECG) was showing T-wave inversion in the precordial Leads. Blood investigation showed positive troponins, and echocardiography showed regional wall motion abnormality in LAD territory with an ejection fraction of 44% without any valvular abnormalities. Coronary angiogram revealed distal left main stenosis of 90% and gaint aneurysm of LAD at its origin measuring 14 × 15mm was noted (Figures 1A & 1B). The patient also had significant stenosis involving
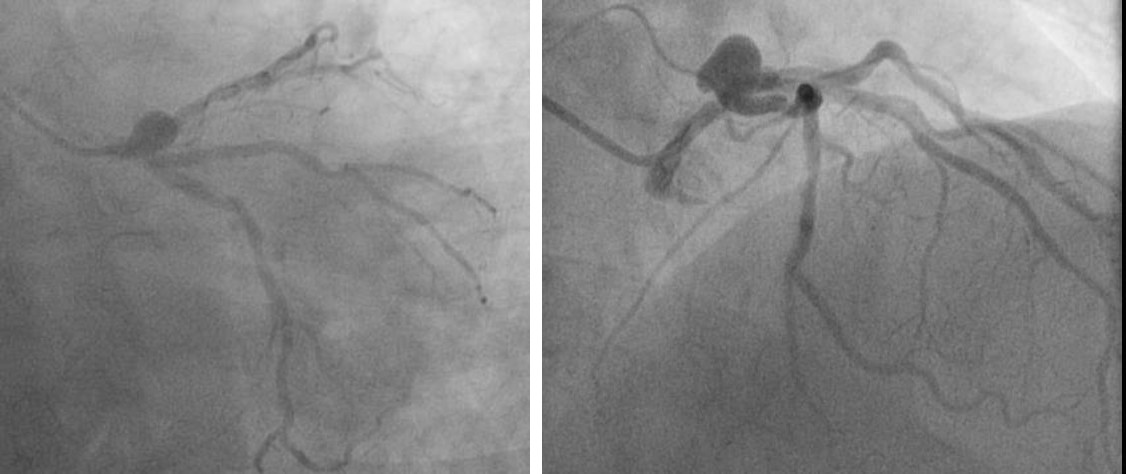
Image Article
proximal Ramus intermedius and LCX. The patient was stabilized and then transferred to the CTVS department for CABG (3 grafts LIMA-LAD, SVG-Ramus, SVG–OM) with the isolation of LAD aneurysm from coronary circulation by proximal and distal ligation. The patient had a usual course of hospitalization and discharged without any complications. At 6 months of follow-up, he has been asymptomatic Giant coronary artery aneurysm is defined as a coronary dilatation that exceeds at least four times of the reference diameter or has a diameter exceeding 8mm [3]. It is a rare coronary pathology, most commonly due to the atherosclerotic origin. Also, other causes include the Kawasaki disease, autoimmune disorders and angioplasty complications [4]. It may manifest with angina pectoris. Surgery is the best-preferred management for giant coronary artery aneurysms, which requires median sternotomy and coronary revascularization [3, 4]. Due to the lack of controlled trials, the prognosis of giant coronary artery aneurysm is under controversies. During 6 months of follow-up, our patient remained asymptomatic without any limitation in his quality of life.
Coronary artery aneurysms are rare malformations caused by atherosclerosis, connective tissue disease or vasculitis, and are usually discovered incidentally with invasive coronary angiography. Coronary artery aneurysms are associated with atherosclerosis and have similar risk factors including dyslipidemia, hypertension, male sex and family history. Patients with a known history of abdominal aortic aneurysm also appear to be at higher risk for Coronary artery aneurysms. Coronary artery aneurysms are a common finding mostly in patients undergoing coronary angiography are located mostly on the right coronary artery and their management depends on the size and clinical presentation [5].
References
-
Syed M, Lesch M (1997) Coronary artery aneurysm: a review. Prog Cardiovasc Dis 40(1): 77-84.
-
Baman TS, Cole JH, Devireddy CM, Sperling LS (2004) Risk factors and outcomes in patients with coronary artery aneurysms. Am J Cardiol 93(12): 1549-1551.
-
Halapas A, Lausberg H, Gehrig T, Friedrich I, Hauptmann KE (2013) Giant right coronary artery aneurysm in an adult male patient with non-ST myocardial infarction. Hellenic J Cardiol 54(1): 69-76.
-
Jha NK, Ouda HZ, Khan JA, Eising GP, Augustin N (2009) Giant right coronary artery aneurysm-case report and literature review. J Cardiothorac Surg 4: 18.
-
Kostopanagiotou K, Poulou A, Chatzis A, Khoury M (2018) Multiple Giant Coronary Artery Aneurysms Surgically Treated with Bypass Grafting: A Challenging Rarity. Case Rep Surg 2018: 2096902.