Serum Cystatin C and Early Diabetic Kidney Disease Prediction: A Preliminary Study in Ivorian Patients with Type 2 Diabetes
Diabetic Kidney Disease (DKD) is the most common cause of the end stage renal disease worldwide. The gold standard for the early detection of this disease is the urinary albumin creatinine ratio (ACR). However, a significant proportion of people with type 2 diabetes have renal failure while remaining normoalbuminuric. This study aimed to evaluate the utility of cystatin C (cys C), as an early biomarker of renal impairment among Ivorian type 2 diabetics. Serum and urinary creatinine, serum glucose, albuminuria and serum cystatin C were determined in 50 diabetic patients. The glomerular filtration rate (eGFR) was estimated using the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation and the ACR was calculated. A Receiver Operating Characteristic (ROC) analysis was applied. Among normoalbuminuric patients, the cys C level in patients with lowered eGFR was statistically higher than those with normal eGFR. Moreover cystatin C was well correlated with eGFR (r= -0,74, P < 0,001). The Receiver Operating Characteristic (ROC) curve analysis, in normoalbuminuric patients with eGFR less than 90 ml/min/1.73 m2 GFR as reference, revealed an area under the curve (AUC) of 0,89 (95%). Serum cystatin C could help for early detection of diabetic kidney disease in support of urinary albumin, especially in normoalbuminuric patients with type 2 diabetes in Cote d’Ivoire.
Introduction
A total of 231, 200 people lived with diabetes in Ivory Coast in 2021 and among them 3,991 died [1]. Diabetic Kidney Disease (DKD) is the most common cause of end stage renal disease worldwide. Its early detection, crucial in the management of diabetic patients, relies mainly on ACR. However, several studies demonstrated that there is a significant number of patients with type 2 diabetes who have impaired renal function with an eGFR less than 60 ml/min/1.73 m2 in the absence of microalbuminuria [2, 3, 4, 5, 6]. The prevalence of the normoalbuminuric diabetics with renal insufficiency increased and has become a prevailing phenotype of DKD at present. A higher incidence of more than 60 % has been observed in recent years [7]. This suggests a need to screen diabetic patients before the onset of microalbuminuria. Cystatin C, a protein secreted by all human nucleated cells, has been proposed as an endogenous marker for the early detection of renal impairment [8, 9]. It is freely filtered through the glomerulus, it is not secreted, but completely catabolized by the proximal tubular cells without entering the bloodstream. Therefore, its plasma concentration seems to be influenced only by the glomerular filtration rate. Many authors present it as a marker of choice for the early detection of diabetic nephropathy [10, 11, 12, 13]. However, its routine use is still controversial [14, 15]. The aim of this study was to investigate the usefulness of cystatin C to predict early kidney failure in subjects with type 2 diabetes. To the best of our knowledges, no documented study has assessed the diagnostic value of the serum cys C, to detect early decline of renal function and compared the performance of the new Chronic Kidney Disease Epidemiology Collaboration (CKD EPI) cr equation with the previous one in type 2 diabetic patients in Ivory Coast.
Materials and Methods
This cross-sectional study was carried out in the Biology and Medical Research Laboratory of the National Institute of Public Health (INSP). It involved fifty (50) patients of black race with type 2 diabetes, from of Antidiabetic Center of Abidjan located at INSP. We excluded patients with hypertension, congestive heart failure, infection, cancer disease or urinary infection. Anonymity ensured data confidentiality and written informed consent was obtained from all individual patient included in the study. Each fasting patient underwent a venous blood sample which was used to assay blood glucose by hexokinase method, serum creatinine (Cr) by isotope dilution mass spectrometry –traceable creatinine Cobas C311, Roche Diagnostics, Basel, Switerzland) and serum cystatin C ( Cys C) by enhanced turbidimetric assay using the Cobas Integra 400 plus®. Part of the morning urine collected on the same day in a sterile specimen cup was analyzed by urine dipsticks, and patients whose sample tested positive for red blood cells, nitrites or leukocytes were excluded from the study. The other part was used for the determination of albumin by immunotubidimetric method and creatinine using Cobas C311. In addition, sociodemographic data (age, gender, profession, place of origin), history (duration of diabetes) and clinical data (body max index, blood pressure) were recorded. eGFR was estimated using four Chronic Kidney Disease Epidemiology Collaboration equations: 2009 CKD-EPI Cr [16], 2012 CKD-EPI Cys C, 2021 CKD-EPI Cr and 2021 CKD EPI Cr-Cys C [17]. The KDIGO classification [18] was used for the interpretation and classification of eGFRs. The ACR was calculated and all subjects were classified as normoalbuminuric (< 3 mg/mmol) or microalbuminuric (3- 30 mg/mmol) patients according to the recommendations of the UK National Institute for Health and Care Excellence NICE on the CKD assessment and management [19]. Using, EXCEL® and XLSTAT® software, the numerical data were represented as mean± SD. The non-parametric Mann-Whitney test at the threshold of 0.05 was used for the comparison of means. The Pearson correlation was applied to evaluate the association between cys C and eGFR values. GFR is the gold standard test for the assessment of the degree of renal impairment. The accuracy of cys C was analyzed against 2021 CKD EPI Cr eGFR. We perform ROC curve to define the discriminating power of the serum level of cys C for detecting eGFR lower than 90 mL/min/1.73 m2 normoalbuminuric patients. This study is part of a project whose study protocol receives the agreement of the national ethical committee.
Results
The sociodemographic and clinical variables of the 50 type 2 diabetic patients included on this study are presented in table I. The mean value of cystatin C was 0, 9 ± 0, 2 mg/L. There was a significant difference among subgroups regarding to age, creatininemia and eGFR. On average, 2009 CKD EPI Cr eGFR was higher than 2012 CKD EPI Cys C eGFR (+12, 3 mL/ min/1.73 m2, P= 0,009), 2021 CKD EPI Cr eGFR (+9, 7 mL/ min/1.73 m2, P= 0, 09) and 2021 CKD EPI Cr-Cys C eGFR (+7, 28 mL/ min/1.73 m2, P=0, 09).
| Setting | Mean | Sub group | Frequency | Cystatin C(mg/L) | P |
|---|---|---|---|---|---|
| Age | 52,2 | < 50 | 20 | 0,81 ± 0,18 | 0, 038 |
| (years) | ≥ 50 | 30 | 0,96 ± 0,22 | ||
| Gender | 0,61 | Male | 19 | 0,9 ± 0,12 | 0,453 |
| (odds) | Female | 31 | 0,9 ± 0,25 | ||
| BMI | 25,63 ± 4 | < 25 | 25 | 0,9 ± 0,15 | 0,449 |
| (Kg /m2) | ≥ 25 | 25 | 0,9 ± 0,27 | ||
| Duration of diabete | 5,5 ± 4 | < 10 | 39 | 0,89 ± 0,23 | 0,392 |
| (years) | ≥ 10 | 11 | 0,92 ± 0,16 | ||
| Glucose sugar | 1,5 ± 0,7 | ≤ 1,1 | 13 | 0,89 ± 0,18 | 0,791 |
| (g/L) | >1,1 | 37 | 0,9 ± 0,22 | ||
| Creatinine | 8,6 ± 1,9 | ≤11 F ; ≤ 13H | 48 | 0,88 ± 0,18 | 0,023 |
| (mg/L) | > 11 F; >13 H | 2 | 1,41 ± 0,41 | ||
| Albuminuria | 25,5 ± 42,3 | ≤ 30 | 39 | 0,9 ± 0,2 | 0,266 |
| (mg/L) | >30 | 11 | 1 ± 0,22 | ||
| ACR | 2,1 ± 3,8 | < 3 | 40 | 0,89 ± 0,21 | 0,416 |
| (mg/ mmol) | ≥3 | 10 | 0,96 ± 0,23 | ||
| GFR | 102 ± 22 | < 90 | 15 | 1,06 ± 0,25 | 0,0003 |
| CKD EPI Cr 2009 | ≥ 90 | 35 | 0,82 ± 0,14 | ||
| (ml /min/1,73m2) | |||||
| GFR | 92,3 ± 18 | < 90 | 19 | 1,07 ± 0,23 | < 0,0001 |
| CKD EPI Cr 2021 | ≥ 90 | 31 | 0,8 ± 0,13 | ||
| (ml /min/1,73m2) | |||||
| GFR | 89,7 ± 22 | < 90 | 24 | 1,05 ± 0,20 | < 0,0001 |
| CKD EPI Cys C 2012 | ≥ 90 | 26 | 0,76 ± 0,10 | ||
| (ml /min/1,73m2) | |||||
| GFR | 94.72 ± 21 | < 90 | 19 | 1,09 ± 0,21 | < 0,0001 |
| CKD EPI Cr-Cys C 2021 | ≥ 90 | 31 | 0,78 ± 0,102 | ||
| (ml /min/1,73m2) |
Table 1: Cystatin C level variation in normoalbuminurics patients.
- Overall, the equations did not differ statistically from each other. Only one significant difference was found between 2009 CKD EPI Cr eGFR and 2012 CKD EPI Cys C eGFR (P=0,009). The classification of patients into 3 stages of CKD using 2021 CKD EPI Cr eGFR, 2012 CKD EPI Cys C
- Among the 40 normoalbuminuric patients, 32, 5 % had an eGFR lower than 90 mL/min/1.73 m2. In this group, the mean cystatin C value of patients with an eGFR lower than eGFR CKD EPI creat 2021 (mL /min/1,73m2)
- < 90
- 13
- 1,07 ± 0,24
- < 0.0001
- ≥ 90
- 27
- 0,8 ± 0,13
Table 2: Cystatin C level variation in normoalbuminurics patients.
| 2012 CKD EPI Cys C | 2021 CKD EPI Cr-Cys C | |||||||
|---|---|---|---|---|---|---|---|---|
| 2021 CKD EPI Cr | I | II | III | Total | I | II | III | Total |
| I | 23 (46%) | 8 (16%) | 0 | 31 | 28 (58%) | 3 (6%) | 0 | 31 |
| II | 4 (8%) | 10 (20%) | 3 (6%) | 17 | 3 (6%) | 13 (28%) | 1 (2%) | 17 |
| III | 0 | 1 (2%) | 1 (2%) | 2 | 0 | 0 | 2 | 2 |
| Total | 27 | 19 | 4 | 50 | 31 | 16 | 3 | 50 |
Table 3: Cystatin C level variation in normoalbuminurics patients.
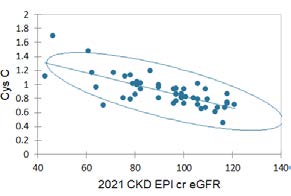
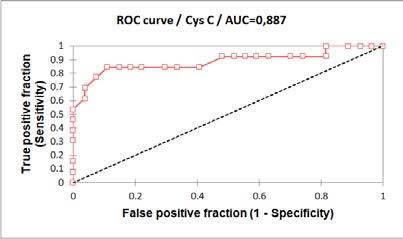
Moreover, we found a significant strong negative correlation (r = - 0 ,74 ; P < 0,0001) between serum cys C and eGFR. Cystatin C values increased with decreasing eGFR (Figure 1). In addition, cystatin C ROC curve analysis (Figure 2) showed an area under the curve (AUC) of 0, 89 p < 0.0001 (95 % CI). The cut off value for the identification of eGFR lower than 90 mL/ min/1.73 m2 conducted by eGFR CKD EPI cr 2021 in normoalbuminutics patients was 0, 94 mg/L with a sensitivity of 84,6 % and a specificity of 88,9 %.
Discussion
The early detection of DKD allows rapid and effective management and slows the progression to chronic renal failure. Several biomarkers and formulas based in these biomarkers may be used to estimate GFR and evaluate renal function. However there is stilll no ideal marker. Classic assessment of DKD includes the appearance of micro albuminuria, a decreased creatinine clearance an increased serum creatinine. But both albuminuria and creatinine have limitations. In this study we assessed the potential added value of serum cystatin C based equation and evaluated the diagnostic value of serum cystatin C to detect early decline of renal function. We used four CKD EPI equations to estimate GFR. In accordance with previous studies [20, 21, 22], CKD EPI Scr 2009, containing black population correction factor, led to an overestimation of the eGFR compared to the three others. In comparison with 2021 CKD EPI Cr eGFR, 2012 CKD EPI Cys C eGFR (P= 0,581) and 2021 CKD EPI Cr-Cys C eGFR (P= 0,508) did not show significant difference. This is consistent with the results of some authors who claim that there is no gain in using cys C to estimate GFR [23, 24, 25]. Moreover, 23,5% of participants did not retain the same CKD stages using theses equations. The large discordance observed in the absence of measured GFR data as reference suggests that either one or all equation loose precision in our cohort. The discrepant CKD categorisation would warrant different dose adjustment and carry different prognostic implications. On the other hand, some authors assert that equations based on cys C are more accurate [26, 27] That highlights the need for further study to investigate the performance of different methods of estimating GFR in Ivorian type 2 diabetic patients. Concerning the serum cystatine C level, we observed a statistically significant difference according to eGFR values. It appears that some normoalbuminuric patients had an eGFR lower than the reference value, with an average level of cystatin C higher than that of patients with a normal eGFR. This reflects the ability of cystatin C to detect slight decreases in eGFR and to be an earlier measurable marker of renal impairment even before the onset of albuminuria. Moreover, strong negative linear relationship was found between cystatin C and eGFR meaning that cystatin C increases with the progression of disease. The AUC of cystatin C curve (0, 89) showed its good performance to distinguish normoalbuminuric patients with renal impairment. This is consistent with findings from previous studies like those of Suman, et al. [28] who obtained similar conclusions (AUC = 0,611 and r = - 0,925). All these results suggest that serum cystatin C is useful and had a good diagnostic accuracy for acute kidney injury in especially normoalbuminuric patients. Despite encouraging results, there are some limitations in our study. First, the small sample size. Indeed, we were not able to achieve a good categorization of the 40 normoalbuminuric patients according to their GFR. In addition, the use of eGFR while the gold standard of GFR is measured by intravenous infusion of exogenous markers. Therefore, ours findings are only suggestive. Those preliminary results suggest planning further studies in our country on large size patient with appropriate gold standard assay to validate the possible application of novel biomarkers like cystatin C for the early detection of DKD and the monitoring of the disease progression.
Conclusion
The determination of serum cystatin C coupled with albuminuria in diabetic patients, could optimize the early detection of renal damage occurring in normoalbuminuric patients.
References
-
(2022) Federation international du diabetes site official.
-
An N, Wu BT, Yang YW, Huang ZH, Feng JF (2022) Re- understanding and focusing on normoalbuminuric diabetic kidney disease. Front Endocrinol 13: 1077929.
-
Ito H, Antoku S, Izutsu T, Kusano E, Matsumoto S, et al. (2020) The prognosis of subjects showing a reduced estimated glomerular fltration rate without albuminuria in Japanese patients with type 2 diabetes: a cohort study for diabetic kidney disease. Clin Exp Nephrol 24(11): 1033-1043.
-
Jia X, Zang L, Pang P, Jiang L, Du J, et al. (2022) A study on the status of normoalbuminuric renal insufficiency among type 2 diabetes mellitus patients: A multicenter study based on a Chinese population. J Diabetes 14(1): 15-25.
-
R Khalaf, Ali ZH, Htira Y, Mami FB (2020) Linsuffisance renale en labsence de microalbuminurie chez le diabetique : a propos de 110 cas. Ann Endocrinol 81(4): 449.
-
Pichaiwong W, Homsuwan W, Leelahavanichkul A (2019) The prevalence of normoalbuminuria and renal impairment in type 2 diabetes mellitus. Clin Nephrol 92(2): 73-80.
-
Deng L, Wenjie LD, Gaosi X (2021) Update on pathogenesis and diagnosis flow of normoalbuminuric diabetes with renal insufficiency. Eur J Biomed Res 26(1):144.
-
Fang WC, Chen HY, Chu SC, Wang PH, Chan LC (2022) Serum Cystatin C Levels Could Predict Rapid Kidney Function Decline in A Community-Based Population. Biomedecine 10(11): 2789.
-
Vivien SS, Delanaye P, Pieroni L, Mariat C, Froissart M (2008) Cystatin C: current position and future prospects. Clin Chem Lab Med 46(12): 1664-1686.
-
Ayesha Q, Asma H, Tariq MA, Alamgir K, Mohammad N, et al. (2018) Serum Cystatin C as an Early Diagnostic Biomarker of Diabetic Kidney Disease in Type 2 Diabetic Patients. J Coll Physicians Surg Pak 28(4): 288-291.
-
Cheng MC, Duan CC, Huang RC, Tang HQ (2020) Circulating cystatin C levels with type 2 diabetes mellitus: a systematic review and meta-analysis. Arch Med Sci 16(3): 648-656.
-
Stankute I, Radzeviciene L, Monstaviciene A, Dobrovolskiene R, Danyte E, et al. (2022) Serum Cystatin C as a Biomarker for Early Diabetic Kidney Disease and Dyslipidemia in Young Type 1 Diabetes Patients. Medicina 58(2): 218.
-
Xueling LYA, Chao X (2022) Value of serum cystatin C for diabetic nephropathy: a meta-analysis. BMC Endocr Disord 22(1): 149.
-
Oddoze C, Morange S, Portugal H, Berland Y, Dussol B (2001) Cystatin C is not more sensitive than créatinine for detecting early renal impairment in patients with diabetes. Am J Kidney Dis 38(2): 310-316.
-
Vigan J, Ahoui S, Agboton BL, Sabi KA, Tchaba R, et al. (2019) Assessment of serum cystatin C in the early detection of type 2 diabetic nephropathy in Cotonou, Benin. African J Nephrol 22(1): 17-20.
-
Levey AS, Stevens LA, Schmid CH, Zhang YL, Castro AF, et al. (2009) A new equation to estimate glomerular filtration rate. Ann Intern Med 150(9): 604-612.
-
Lesley AI, Nwamaka DE, Coresh J, Tighiouart H, Wang D, et al. (2021) Chronic Kidney Disease Epidemiology Collaboration. New creatinine- and cystatin c-based equations to estimate gfr without race. N Engl J Med 385(19): 1737-1749.
-
Kidney Disease Improving Global Outcomes (2013) Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney Int Suppl 3: 136-150.
-
(2021) Chronic kidney disease: assessment and management. NICE.
-
Eneanya ND, Yang W, Reese PP (2019) Reconsidering the consequences of using race to estimate kid-ney function. JAMA 322(2): 113-114.
-
Delgado C, Baweja M, Crews DC, Eneanya ND, Gadegbeku CA, et al. (2021) A unifying approach for GFR évaluation: recommendations of the NKF-ASN task force on reassessing the inclusion of race in diagnosing kidney disease. J Am Soc Nephrol 32(12): 2994-3015.
-
Rulan SP, Jeffrey P, Auguste B, Manish MS (2022) Retrait delelement race dans levaluation de la fonction renale pour une prise en charge impartiale au Canada. CMAJ 194(18): E663-E665.
-
Bukabau JB, Yayo E, Gnionsahe A, Monnet D, Pottel H, et al. (2019) Performance of creatinine- or cystatin C-based equations to estimate glomerular filtration rate in sub-Saharan African populations. Kidney Int 95(5): 1181-1189.
-
Iliadis F, Didangelos T, Ntemka A, Makedou A, Moralidis E, et al. (2011) Glomerular filtration rate estimation in patients with type 2 diabetes: creatinine- or cystatin C-based equations? Diabetologie 54(12): 2987-2994.
-
Xia LH, Bin XG, Wang XJ, Zhang XC, Yang JM (2010) Diagnostic accuracy of various glomerular filtration rates estimating equations in patients with chronic kidney disease and diabetes. Chin Med J 123(6): 745-751.
-
Domingueti CP, Foscolo RB, Silva ACE, Dusse LMS, Reis JS, CarvalhoMDG, et al. (2016) Evaluation of creatinine- based and cystatin C-based equations for estimation of glomerular filtration rate in type 1 diabetic patients. Arch Endocrinol Metab 60 (2): 108-116.
-
Lima SL, Cabrera BE, Mena NN, Estupinan S, Mallen PD, et al. (2019) Chronic kidney disease staging with cystatin C or creatinine-based formula : flipping the coin. Nephrol Dial Transplant 34(2): 287-294.
-
Sapkota S, Khatiwada S, Shrestha S, Baral N, Maskey R, et al. (2021) Diagnostic Accuracy of Serum Cystatin C for Early Recognition of Nephropathy in Type 2 Diabetes Mellitus. Int J Nephrol 2021: 8884126.
- Superposition of Cryo-EM and AlphaFold Predictions of Dengue Antigen-Antibody Complexes
- Jugular-Applied Coherent Low-Level Laser Therapy Enhances Systemic Mitochondrial Metabolic Function and Antioxidant Response
- Role of OMC32 Polypeptide in Acrosin-Mediated Exocytosis during the Bovine Sperm Acrosome Reaction
- Association of Galectin-3 but not Laminin in Tamoxifen-Induced Growth Suppression in Breast Cancer MCF-7 Cells
- Effect of Different Wavelengths of Light on the Rate of Photosynthesis
- Nutritional, Therapeutic, and Environmental Effect of Oyster Mushrooms: An Editorial