Coccidioidomycosis with Laryngeal Nodule and Cavitary Lung Disease: A Case Report
Coccidioidomycosis is the infection caused by the dimorphic fungi of the genus Coccidioides. Primary pulmonary infection is caused by inhalation of airborne mycelial arthroconidia located in soil. While most infections are asymptomatic, clinical illness ranges from acute pneumonia (Valley Fever) to extra-thoracic disseminated infection. Most cases of coccidioidomycosis in the United States are endemic in the southwestern part of the country, particularly in Arizona, the San Joaquin Valley of California; parts of Mexico and Central and South America. Here we describe the case of a 13- year-old boy with an unusual history of hoarseness of voice, in whom laryngoscopy and biopsy were performed, and subsequent histologic diagnosis of coccidioidomycosis was established.
Case Report
A 13-year-old male with no significant past medical history presented to the primary care at Harbor-UCLA Medical Center with 9 months of persistent hoarseness and productive cough, associated with dysphonia. Over this period, his voice worsened to the point that patient was only able to speak very softly. He had associated increased white sputum production and occasional nose bleeds. He also had history of fever with chills and rigor one month prior to presenting at Harbor UCLA. The patient otherwise denied any history of hemoptysis, fatigue, weight loss, swollen lymph nodes, chest pain, shortness of breath, orthopnea or rash. The mother denied any exposure to tuberculosis contacts or any recently incarcerated individuals. The family went to a trip to Tijuana (Baja California, located on the Pacific Coast of Mexico) about a year ago. The patient was admitted for further work up. The investigations complete blood count, TB QuantiFERON gold, AFB sputum culture, urine culture, PCR, HIV antibody were ordered. Chest X-Ray was noted for left upper lung scarring. CT chest showed circumferential thickening in the walls of the larynx; and a 2.6 cm thick-walled cavitary lesion in the left lung apex. Subsequently, the patient underwent laryngoscopy that was revealed “scattered papular lesions along posterior pharynx; the supraglottis was irregularly thickened with multiple exophytic, round polypoid-appearing lesions.” The laryngeal tissue biopsy was sent to pathology. The clinical picture, CT and laryngoscopy findings were most concerning for pulmonary TB with extrapulmonary spread to larynx.
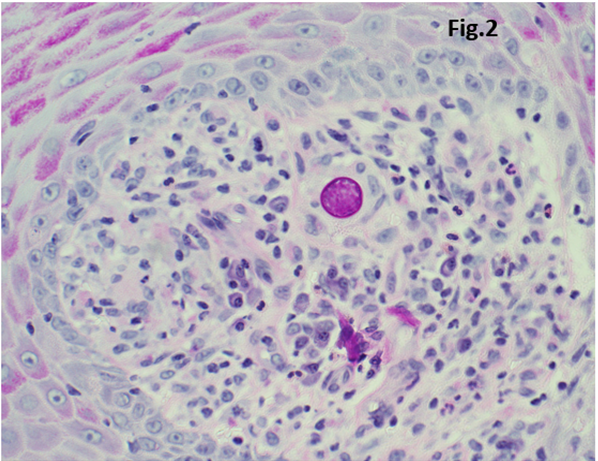
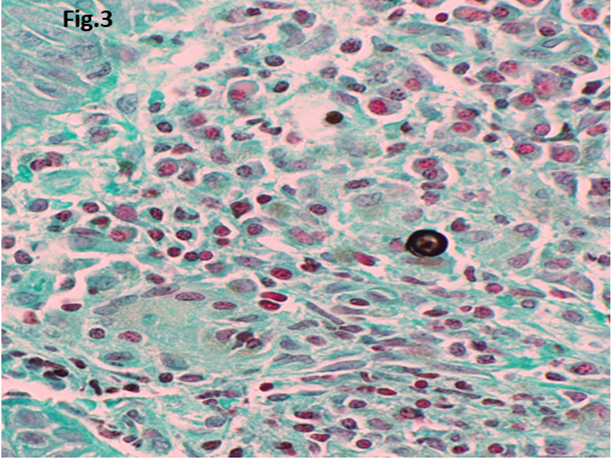
The investigation results revealed that TB QuantiFERON gold, AFB sputum culture, urine culture, PCR and HIV antibody were negative. Microscopic examination on hematoxylin and eosin stain of the left vocal cord lesion revealed squamous mucosa with well-formed granulomas (Figure 1A). At higher power, the granulomas contained spherules and endospores, surrounded by mixed inflammatory infiltrate (Figure 1B). At high magnification, large spherical fungal forms with eosinophilic wall and multiple basophilic endospores can be identified (Figure 1C). Special stains of PAS (Figure 2) and GMS (Figure 3) highlighted the fungal organisms. The coccidioidomycosis with an eosinophilic wall measured up to 100 μm in diameter and contained multiple basophilic endospores (5 μm).
The patient was subsequently treated with anti-fungal azole agent, fluconazole over a period of 6 months, following which his symptoms improved. The patient was followed up with repeat chest X-ray one year after initiation of treatment and revealed a fibrotic scar measuring 1.2 cm at the left apical lung.
![Figure 1: Representative photomicrographs of the left vocal cord lesion. A. Low power view showing squaumous mucosa with well formed granulomas. B. At high power, the granulomas contained spherulus and endospores, surrounded by mixed inflammatory infiltrate. C. At high magnification, large spherical fungal forms with eosinophilic wall and multiple basophilic endospores can be identified. (H&E stain; original magnification, x 40 [A], x 200 [B], x 400.](/fulltextimages/10981/fig_1.png)
Figure 1: Representative photomicrographs of the left vocal cord lesion. A. Low power view showing squaumous mucosa with well formed granulomas. B. At high power, the granulomas contained spherulus and endospores, surrounded by mixed inflammatory infiltrate. C. At high magnification, large spherical fungal forms with eosinophilic wall and multiple basophilic endospores can be identified. (H&E stain; original magnification, x 40 [A], x 200 [B], x 400.
Discussion
The dimorphic fungus Coccidioides causes coccidioidomycosis is also known as San Joaquin Valley fever. It is endemic to the regions of the south western parts of United States, parts of Mexico and Central and South America [1]. Coccidioides is a genus of dimorphic fungi that exist as mycelium in soil and produces a spherule form in the host organism [2]. Arthroconidia is the infectious particles of Coccidiosis species. Infections usually occur due to inhalation of the arthroconidial spores after soil disruption and transform into spherules in the tissues [3]. Spherules are filled with endospores (2 micrometers to 5 micrometers). This spherule can burst within the tissues to release endospores, which can disseminate the infection [4]. Most infections are asymptomatic (60%), and when symptoms do occur, the presentation can be confused with community- acquired bacterial pneumonia or bronchitis. Fever, cough, shortness of breath or chest pain are the most common presenting symptoms, mimicking pulmonary tuberculosis. Headache, fever or rash may be seen. Other pulmonary manifestations include peripheral lung nodules and cavities. On the other hand, immunocompromised host such as HIV or pregnant patient may show disseminated disease and may develop vertebral osteomyelitis, joint infection or CNS involvement which is often fatal [5, 6, 7].
Conclusion
Coccidioidomycosis can be acquired by individuals who travel even briefly through an endemic area presenting a diagnostic dilemma. The clinical and radiographic manifestations of pulmonary coccidioidomycosis often mimic pneumonia. However, because its treatment differs substantially from bacterial community-acquired pneumonia, an accurate and timely diagnosis of coccidioidomycosis is essential. The clinician should have a high degree of suspicion, especially in an individual with history of travel to an endemic area.
Author Contributions Statement
KV identified the case and conceived of the presented idea. KV performed the literature search and wrote the first draft of the article. AB and AK prepared the figures/figure legends and helped shape the manuscript. PJ provided critical feedbacks. KV supervised this work, performed additional literature search, and wrote the final version of the article.
References
-
Saubolle MA, McKellar PP, Sussland D (2007) Epidemiologic, clinical, and diagnostic aspects of coccidioidomycosis. J Clin Microbiol 45(1): 26-30.
-
Deresinski S, Mirels LF (2019) Coccidioidomycosis: What a long strange trip it’s been. Med Mycol 57(1): S3-S15.
-
Taylor JW, Barker BM (2019) The endozoan, small- mammal reservoir hypothesis and the life cycle of Coccidioides species. Med Mycol 57(1): S16-S20.
-
Thompson GR, Lewis JS, Nix DE, Patterson TF (2019) Current Concepts and Future Directions in the Pharmacology and Treatment of Coccidioidomycosis. Med Mycol 57(1): S76-S84.
-
Sondermeyer GLC, Jain S, Vugia DJ (2019) Epidemiology of coccidioidomycosis among children in California, 2000-2016. Med Mycol 57(1): S64-S66.
-
Laniado-Laborín R, Arathoon EG, Canteros C, Muñiz- Salazar R, Rendon A et al. (2019) Coccidioidomycosis in Latin America. Med Mycol 57(1): S46-S55.
-
Lauer A, Baal JD, Mendes SD, Casimiro KN, Passaglia AK, et al. (2019) Valley Fever on the Rise-Searching for Microbial Antagonists to the Fungal Pathogen Coccidioides immitis. Microorganisms 7(2): 31.
- Assessing the Accuracy of Refractive Prediction of Different IOL Formulas in Medium Long Eyes
- The Effect of Imatinib on the Fetus Growth and Development of a Pregnant Woman Involved with CML, a Case Report and a Literature Review
- Acquired Neutropenia and Fever, its Treatment and Complications in an Infant, A Case Report
- Hodgkin Lymphoma in a Girl with Common Variable Immune Deficiency: A Case Report and Review of Literature
- Public Administration and the Management of Beliefs in Risks and Dangers in the COVID-19 Era
- Histopathological Study of Placentas of Hypertensive Disorders