Histopathological Study of Placentas of Hypertensive Disorders
Background and Objective: Pre-eclampsia and eclampsia are common complications in pregnancy, and they lead to utero placental vascular insufficiency. More than 38% of pregnant women succumb to seizures without meeting the clinical criteria for pre-eclampsia and eclampsia. This signifies the importance of a confirmatory diagnosis of pre-eclampsia or eclampsia using the histopathological changes seen in placenta . Hence, the aim of the study was to determine the incidence of histopathological abnormalities in the placentas of singleton pregnancies with hypertensive disorders. Materials & Methods: The study was carried out at Rajendra Institute of Medical Sciences, Ranchi, India from June 2018 to July 2020. In this study spanning two years, 134 cases of pre-eclampsia/eclampsia were included. Placenta tissues were collected from the labor room and histological slides were prepared in the Histology Lab. All the steps of Tissue Processing were done and slides were observed under the light microscope after proper staining. Results: A significant association between the histopathological parameters of the placenta, including fibrin deposition, syncytial knots, hypovascular villi and clinical diagnosis of pre-eclampsia and eclampsia was found. Conclusion: This study elucidates a significant association between placental histopathological patterns, caused by preeclampsia and eclampsia.
Introduction
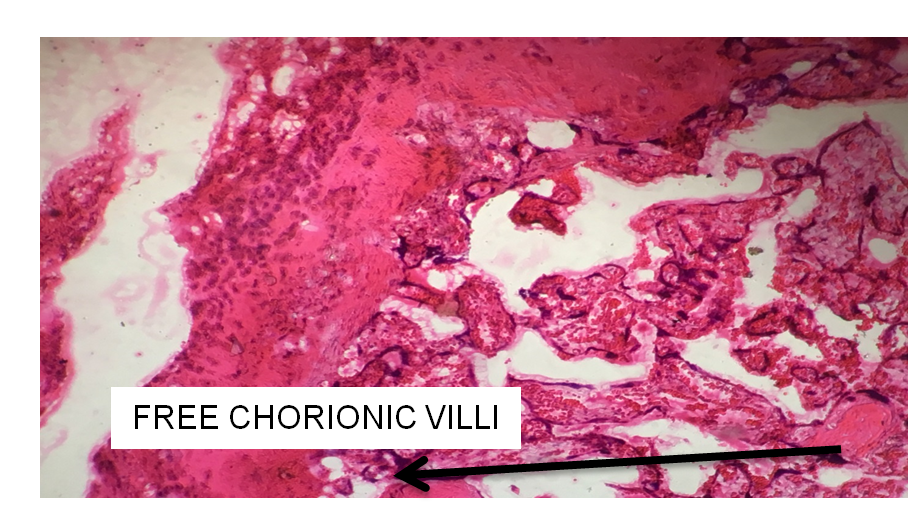
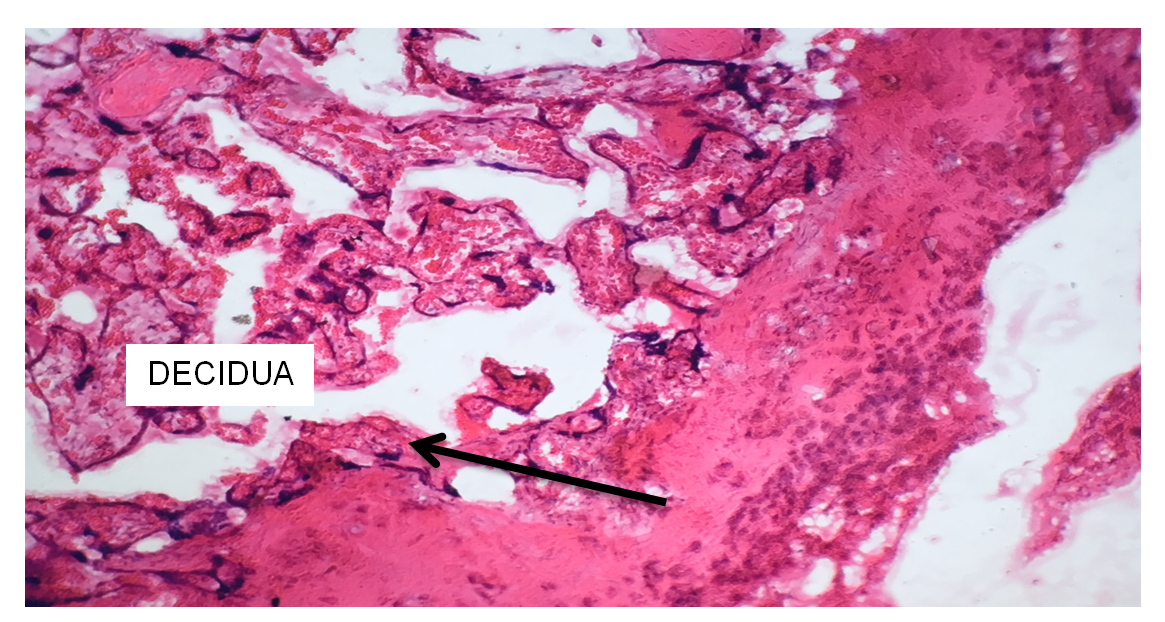
Humans have a hemochorial and bidiscoid type of placenta. Histologically, the placenta of humans is composed of the placental villi, the chorionic plate, the basal plate and the decidua (Figures 1 & 2).
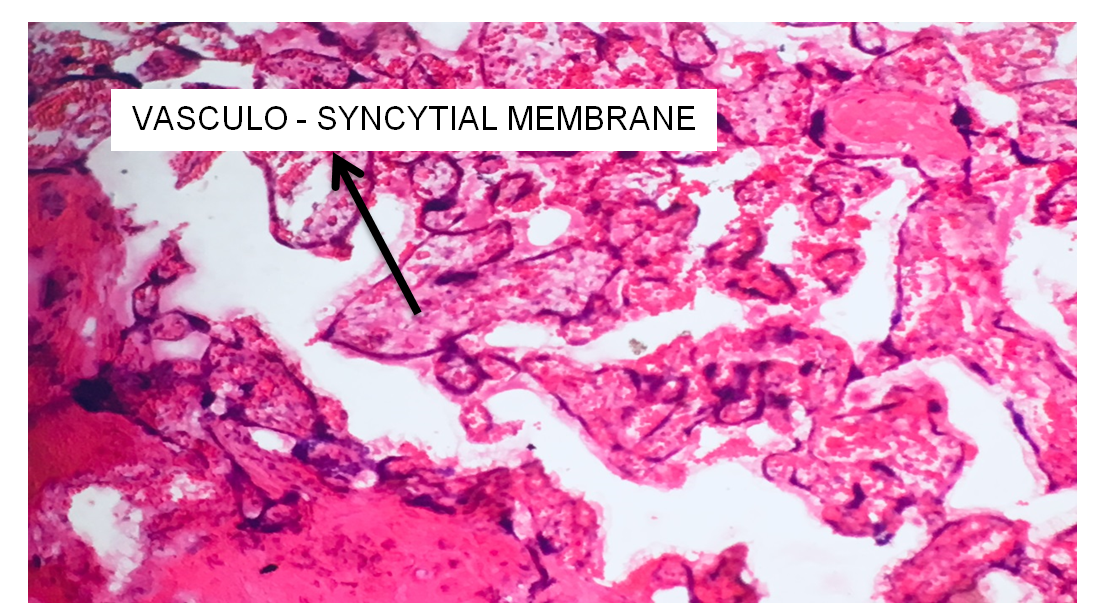
The placental villi protrude into the intervillous space and are bathed directly in maternal blood. The anchoring villi are peripheral ones that are connected to the basal zone. The placental villous surface is composed of an outer continuous layer of syncytiotrophoblasts in contact with maternal blood and an inner discontinuous layer of cytotrophoblasts (Figure 3).
The stroma of the placental villi is composed of fetal vessels and mesenchyme. The chorionic plate is populated with mesenchymal cells within a fibrous connective tissue, and represents the cover of the intervillous space. Tree- like arranged placental villi arise from the chorionic plate. The basal plate is the bottom of the intervillous space and the junction of the endometrium with fetal tissues. The basal plate is composed of extravillous cytotrophoblasts, endometrial stromal cells, decidual cells, etc. According to GP Pal in his Textbook of Histology (3rd Edition), a slide of placenta will show the cross - section of many villi (Figure 1). A villus is lined with the inner layer of cytotrophoblasts and outer layer of syncytiotrophoblasts. The cytotrophoblasts are cuboidal in shape and lie on basement membrane. The syncytiotrophoblast layer is the layer of multi- nucleated cytoplasm with indistinct cell margins. The core of the villi contains umbilical blood capillaries embedded in thin layer of fetal connective tissue. The cross - section of villi are surrounded by maternal blood (RBCs) [1, 2]. The villus capillary pressure varies from 20 to 40 ml of Hg. The fetal blood flow through placenta is 400 ml / minute. This is mainly facilitated by pumping action of fetal heart. Dutta DC [3]. In general, hypertensive disorders lead to maternal vascular compromise resulting in placental ischemia, which further leads to various histopathological changes in the placenta.
In the present study group, the histology revealed various structural changes such as significant number of syncytial knots, areas of fibrinoid necrosis, areas of stromal fibrosis and areas of hypovascular villi. Microscopic findings of localized fibrinoid necrosis, stromal fibrosis and hypovascular villi depict the mosaicism of placenta. Ramsey and Donner presented a summary of Anatomical studies and uteroplacental vasculature. Ramsey found that maternal blood enters the intervillous space in spurts produced by maternal blood pressure [4]. According to Robertson, the cause of reduction in blood flow is due to vasculopathies of spiral arteries, which in turn causes reduction in the weight of placenta. It has been recorded that maternal utero-placental blood flow is decreased in pre-eclampsia because of maternal vasospasm. Reduced maternal utero- placental blood flow indirectly leads to constriction of fetal stem arteries [5]. Fibrinoid is a term applied to any acellular, eosinophilic, largely homogeneous substance in the placenta. Although not part of the structural framework of the villous trees, fibrinoid necrosis is a regular finding in every normal placenta [2]. Stromal fibrosis of terminal villi may possibly result from impairment of placental circulation of different causative background.
Histological Abnormalities
• Increased Syncytial Knot Formation: These are fetal clumps of syncytial nuclei protruding from the outer surface of villous trophoblasts.
• Villous Hypo Vascularity: These are areas of reduced blood supply, may be due to placental insufficiency.
• Stromal Fibrosis: Stromal fibrosis is introduced by transient activation of mesenchyme of the terminal villi. Edema of villous stroma may be of diffuse or focal manifestation in the terminal villi and in advanced cases may affect all parts of the placenta.
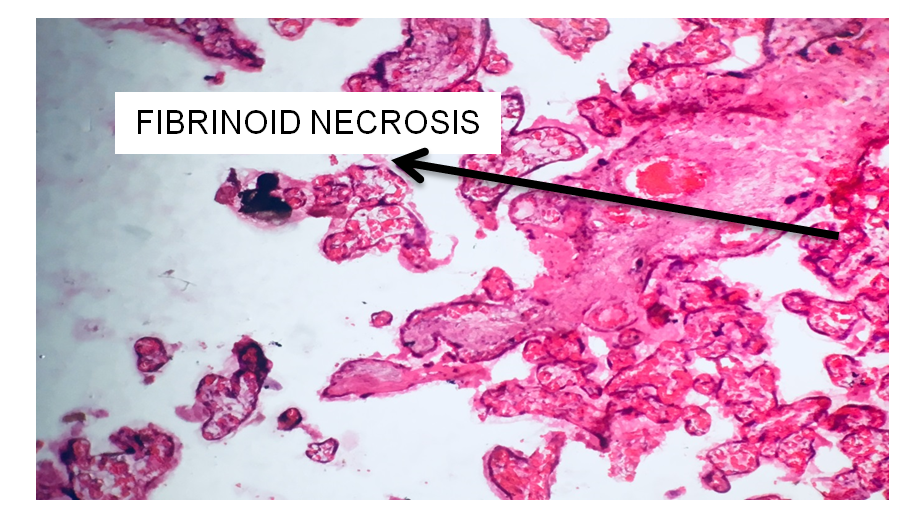
• Fibrinoid Necrosis: Fibrinoid necrosis is a specific pattern of irreversible, uncontrolled cell death that occurs when antigen-antibody complexes are deposited in the walls of blood vessels along with fibrin. It is common in the immune-mediated vasculitides which are a result of Type III hypersensitivity. When stained with hematoxylin and eosin, they appear brightly eosinophilic and smudged.
Aims and Objectives
The main aim of the present study is to determine the incidence of placental histopathological abnormalities such as fibrin deposition, syncytial knot formation, hypovascular villi in singleton pregnancies with Pre- Eclampsia and Eclampsia.
Materials & Methods
Intact and fresh placentas were obtained from the labor room of Department of Gynecology, RIMS, and Ranchi.
Materials Used for Data Collection
- Tray
- Test - tubes
- Dissecting forceps
- Beakers
- Scalpel
- Knife
- Glass jar
Chemicals Used
- 10% Formalin
- Alcohol ( 90% ,70%, 50%, absolute)
- Methyl Benzoate
- Haematoxylin stain
- Eosin 1%
- Xylol
- 0.5% HCL
Equipment Used
- Incubator
- Automatic Embedding Machine
- Rotary Microtome
Histological Examination
1. Tissue Processing 2. Tissue Cutting and Fixation: Membranes were rolled from the periphery, stripped up to the center and removed. A 1 x 1 cm sized tissue was taken from near the center. These tissues were fixed in 10% formalin in separate containers and were labeled. Tissue Fixation was done for 1-2 days.
3. Rinsing: The tissue was rinsed in running tap water. 4. Dehydration: Tissue was subjected to ascending grades of alcohol. a. 50% - 24 hrs. b. 70% - 24 hrs. c. 90% - 24 hrs. d. Absolute Alcohol - 24 hrs. 5. Clearing: Clearing was done by Methyl Benzoate for 24 hrs. 6. Embedding: Impregnation of the tissue by a solid medium, paraffin wax, was done. Wax Blocks were prepared and kept on cold plate (Figure 4).
7. Trimming: Paraffin embedded blocks were trimmed by a sharp knife leaving an edge of 2 - 3 mm. 8. Section Cutting: Sections were cut approximately 7 microns thick and ribbons were made (Figure 5).
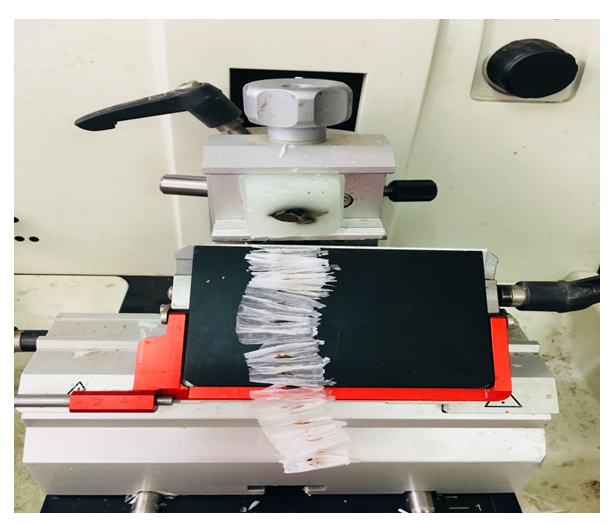
Ribbons were floated on hot water bath. Sections were taken on a slide and kept on a hot plate for drying. Slides were stored in boxes.
Staining
Slides were stained routinely by hematoxylin and eosin.
Preparation of Haematoxylin Stain
- Physical balance was adjusted.
- Heamatoxylin powder (1 gm.) was taken on a paper.
- In a test - tube it was dissolved in 10 ml of Absolute Alcohol (Solution no. 1).
- Potassium Alum (20 gm.) was taken and dissolved in 200 ml distilled water (Solution no. 2).
- Solution no. 1 and Solution no. 2 were added in a jar and shaken thoroughly.
- A tripod stand was put on a Bunsen burner and the jar was put on it.
- The solution was allowed to boil.
- 0.5gm of Mercuric Oxide was slowly added to it.
- Color of the solution changed to blue.
- Rapid cooling of the solution was done in a tap water.
- Solution was filtered using a filter paper and was stored in a dry bottle.
- 8 ml Glacial Acetic Acid was taken by a pipette and mixed to the solution.
Preparation of Eosin Stain
Eosin powder (1gm) was taken and added to 100 ml of 70% Alcohol. The solution was shaken thoroughly.
Preparation of Section Adhesive
A fresh egg was taken. Yolk was separated from the egg white using a spoon.
- Egg white - 50 ml,
- Glycerol - 50 ml, and
- Sodium Salicylate - 1 gm. were taken All three were mixed well and Mayor’s Glycerol Albumin was prepared.
Staining Method used in the study was Haematoxylin and Eosin Staining Method.
This Procedure is as Follows
- Sections on the slides were de waxed through descending grades of alcohol keeping the slide in each for 2 minutes.
- Stained in Haematoxylin stain for 5-7 minutes, then washed in distilled water and differentiated in 0.5% HCL.
- Washed in running tap water to remove excess stain.
- Treated with ascending grades of alcohol for 2 minutes each.
- Stained for 30 seconds in alcoholic solution of Eosin (1% Eosin in 70% alcohol).
- Rinsed rapidly in 90% alcohol.
- Dehydrated in two changes of absolute alcohol, cleared in xylene and mounted in D.P.X, using egg albumin as adhesive.
- The stained slides were observed under light microscope.
Discussion
The present study was undertaken on the placentas obtained from labor room of RIMS Ranchi. The present work has been conducted on a total of 134 placentas obtained from pre - eclampsia or eclampsia cases, either delivered normally or by cesarean section.
Results
This study was carried out using the following parameters (Table 1).
| Histopathological Findings | No. of Specimen | Percentage | |
|---|---|---|---|
| 1 | Fibrinoid Necrosis | 32 | 24% |
| 2 | Syncytial Knots | 38 | 28% |
| 3 | Villous Fibrosis | 44 | 33% |
| 4 | Hypovascular Villi | 20 | 15% |
Table 1: Showing Histology Observation with the number of specimens and percentage.
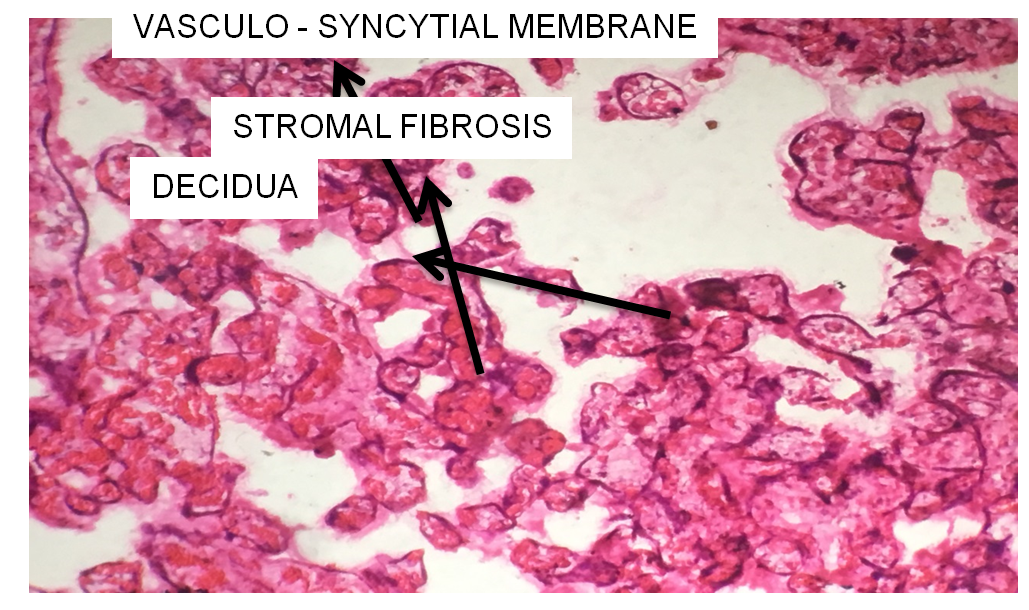
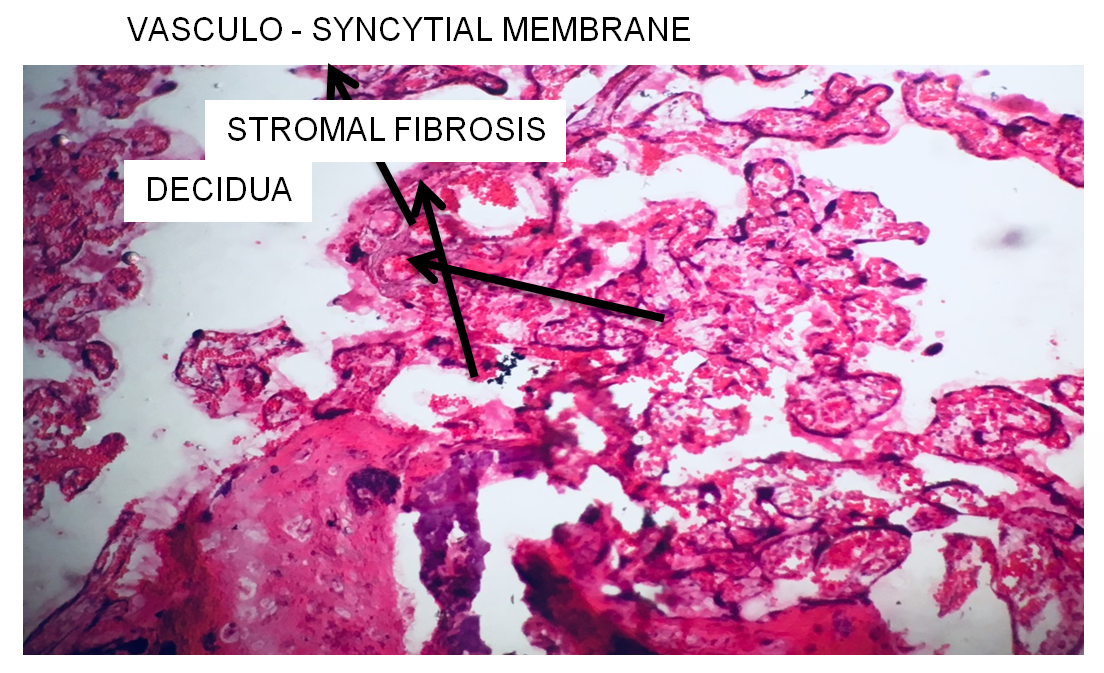
Stromal Fibrosis
33% of placentas, showed villous / stromal fibrosis (Figure 6). The two main factors thought to be responsible for the formation of stromal fibrosis are normal aging and reduced blood flow, stromal fibrosis due to reduced blood flow seems more conclusive as excess stromal fibrosis was sees in cases of hypertensive disorders [6].
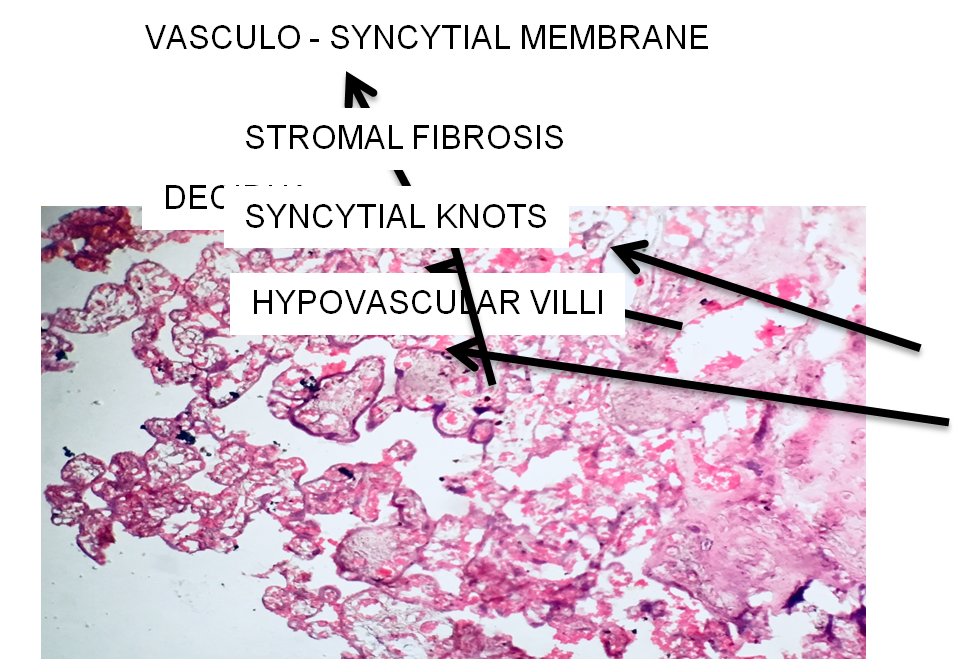
Syncitial Knot Formation
28% of placentas showed syncitial knot formation (Figure 7). Significant high percentage of placentas was found with syncytial knots in hypertensive case. It may be related to reduce fetal villous flow in these cases. Fox concluded from his study that excess syncytial knot formation occur in generalized form whenever the foetal circulation through the villi appears to be reduced. Irrespective of the mechanism which is responsible for reducing fetal blood flow through the villi the inevitable result is stromal fibrosis and excess syncytial knot formation both of which are good indices of the degree of reduction in villous perfusion [7].
Villous Hypo Vascularity
15% of placentas showed hypovascular villi (Figure 8). The mechanism involved in producing hypovascular villi is not fully understood. In the present study statistically significant percentage of hypovascular villi was observed in cases of hypertensive placenta. Few authors have reported that fibrinoid necrosis, endothelial proliferation of arteries and hypovascular villi depict the mosaicism of placenta and probably the aftermath of hypertension. Again the mosaicism of the placenta probably leads to placental insufficiency and ultimately to fetal growth retardation, thus creating a vicious cycle [8].
Fibrionoid Necrosis
24% of placentas showed fibrinoid necrosis (Figure 9). Appearance of fibrinoid necrosis is that of a mass of structure less, homogenous, acidophilic material around the periphery of which are a few degenerate syncytial nuclei. Many workers have thought that this lesion is due to replacement of the villus by fibrin , this being formed either from the maternal blood in the intervillous space or from the fetal blood in the villous capillaries.
Conclusion
By observing the histological results, it has been concluded that all the parameters of evaluation, i.e., fibrin deposition, syncytial knots and hypovascular villi were found in sufficient percentage in the placentas. Hence, in the view of the present author, it has been suggested that all the placentas of hypertensive cases must be examined histologically, to foresee any obstetrical, pathological or neonatal complications.
Acknowledgement
The author would like to express thanks to the Department of Obstetrics and Gynecology (RIMS) for the permission to collect the placentas. The author also owes a big thank you to colleagues at the Department of Pathology (RIMS) for their great help whenever needed. The author declares that submitted manuscript is original research work and has not been published. It is not under simultaneous consideration for publication elsewhere. Due permission was taken from the ethical society at Rajendra Institute of Medical Sciences, Ranchi, India.
References
-
Donthi D, Malik P, Mohamed A, Kousar A, Subramanian RA (2020) An Objective Histopathological Scoring System for Placental Pathology in Pre-Eclampsia and Eclampsia. Cureus 12(10): e11104.
-
Pal GP (2012) Textbook of Histology. 3rd (Edn.), Publisher Paras.
-
Dutta DC (1993) Placental circulation Placental function. Obs and Gynae.
-
Donner R (1980) Placental Vascular and circulation. Saunders, Philadelphia.
-
Robertson WB, Brosens I, Dixon HG (1967) The Pathological Response of the Vessels of the Placental Bed to Hypertensive Pregnancy. J Pathol Bacteriol 93(2): 581-592.
-
Benirschke K, Burton GJ, Baergen RN (2012) Pathology of the Human Placenta. 6th (Edn), Springer Berlin, Heidelberg, 18: 941.
-
FOX H (1978) Pathology of Human Placenta. Monography, Saunders, Philadelphia 7.
-
Emmrich P, Pathol Z (1992) Pathology of the placenta. Intrauterine fetal death. Regression. Edema and Fibrosis of the villous stroma. PubMed 138(1): 1-8.
- Assessing the Accuracy of Refractive Prediction of Different IOL Formulas in Medium Long Eyes
- The Effect of Imatinib on the Fetus Growth and Development of a Pregnant Woman Involved with CML, a Case Report and a Literature Review
- Acquired Neutropenia and Fever, its Treatment and Complications in an Infant, A Case Report
- Coccidioidomycosis with Laryngeal Nodule and Cavitary Lung Disease: A Case Report
- Hodgkin Lymphoma in a Girl with Common Variable Immune Deficiency: A Case Report and Review of Literature
- Public Administration and the Management of Beliefs in Risks and Dangers in the COVID-19 Era