Association of Tumor Necrosis Factor-α 308A/G Gene Polymorphism with Obesity among a Population of Southwestern Nigeria
Obesity often results from interplay of genetics, nutrition and lifestyle. A polymorphic variant of the Tumor Necrosis Factor-α (TNF- α) promoter region (308G/A) is associated with increased production of TNF- α protein, which could lead to fat accumulation implicated in the development of obesity and cardiovascular disease. This study investigated the association of TNF-α 308G/A polymorphism with obesity among a population residing in Southwestern Nigeria. Two hundred (200) obese and 197 age and sex matched non-obese subjects were enrolled. Blood pressure, weight, height, waist and hip circumferences were measured. Estimation of fasting blood sugar level, DNA extraction from whole blood and genotyping of single nucleotide polymorphisms of TNF-α 308G/A were done using standard laboratory procedures. Data were analyzed and p-value < 0.05 was considered significant. Mean body weight and BMI were significantly increased in the obese group (81.92±1.00 kg, 33.01±0.25kg/m2) compared with controls (72.03±1.01 kg, 22.06±0.22kg/m2). Waist and hip circumferences were increased among obese subjects (p
Introduction
Obesity, described as excessive fat in the body is associated with dyslipidemia, high blood pressure and Type
2 diabetes mellitus. It is preventable if interplay of genetics, nutrition and lifestyle is fully understood [1, 2]. An imbalance between energy intake and utilization is often responsible for obesity. This could result from changes to ‘Western’ lifestyle and dietary habits [3]. Obesity linked to cardio- metabolic disorders may result in poor health outcomes and mortality. There were estimated 12 million obese individuals in Nigeria with a female preponderance. A high prevalence of obesity (31%) has been reported among a population of Southwestern Nigerian descent [4]. Activation of the innate immune system in adipose tissue promotes pro-inflammatory status and oxidative stress, triggering a systemic acute-phase response. Inflammation of adipose tissue in obese patients was hypothesized to play a critical role in the pathogenesis of obesity-related complications [5]. Tumor Necrosis Factor-α gene, an adipocyte-derived cytokine, and its 308A allele are up regulated in obesity and is a genetic marker for susceptibility to obesity [6, 7, 8]. Tumor Necrosis Factor- 308 polymorphism has been found on promoter region of TNF- alpha gene with G → A substitution therefore increasing transcriptional activation of the gene [9].
Genetic variation is a non-modifiable factor for interpersonal propensity to develop and regulate obesity [2]. The impact of TNF-α G308A polymorphism on obesity might be limited because of involvement of multiple factor [1, 2]. Despite extensive work done on different populations [3, 7], there are inconsistent reports on association between TNF-α G308A polymorphism and obesity [3, 4, 5, 6, 7, 8, 9]. The present study investigates the frequency of occurrence of TNF-α G308A polymorphism and its association with cardiovascular disease risk among an obese population of Southwestern Nigeria.
Methods
Study Design
This is a case-control study carried out in Ladoke Akintola University of Technology Teaching Hospital, Osun and Oyo States, Nigeria from 2nd February to 11th August 2017. The study protocol was approved by the Ethical Review Committees of LAUTECH Teaching Hospital Ogbomoso (LTH/ OGB/EC/2015/083) and College of Health Sciences Osogbo (LAU/CHS/DEAN/ETHICAL/052/pro/2015/009) Nigeria respectively. Written informed consent was obtained from all participants before commencement of study after the protocol has been explained. Participant’s Height (m) and weight (kg) were measured using Stadiometer and weight scale (to one decimal place) while waist-hip measurement (cm) was done by tape rule.
Genomic DNA isolation was done by salting out. Genotyping was carried out by Anti-Refractory Mutation System (ARMS) Polymerase Chain Reaction (PCR) and allelic distribution analyzed statistically. Two hundred (200) obese and one hundred and ninety-seven age and sex-matched non-obese controls were recruited based on sample size calculation using Cochrane formula ( ) 2 $$ n = \frac {Z ^ {2} p (1 - p)}{d ^ {2}} $$ ( )
2
2 1.96 0.148 0.852 $$ \text {w h e r e} = \frac {\left(1 . 9 6\right) ^ {2} 0 . 1 4 8 \times 0 . 8 5 2}{0 . 0 5 ^ {2}} = 1 9 3. 6 7 $$
- n is sample size.
- Z, the standard deviation at 95%
confidence interval (1.96);
- p, the prevalence (14.8%); (7)
0.05 - d, degree of accuracy (0.05)
Obese subjects (defined by BMI ≥ 30kg/m2) that are not diabetic, hypertensive or suffering from any cardiovascular disease were included in the study. Non-obese individuals with BMI ≤ 25 Kg/m2 without any lipid metabolism – related pathological disorder were included as controls. Subjects diagnosed with diabetes mellitus, cardiovascular diseases, chronic hepatic or renal disease, inflammatory or endocrine disorders were excluded from the study.
TNF-α 308G/A Genotyping
Genomic DNA was isolated from filter paper dried blood spot by proteinase-K digestion and a standard high salt- extraction method using QIAamp DNA blood mini kit (Hilden, Germany, Lot number 51104). The blood spot filter was kept at room temperature. An internal control was used to assess the success of PCR detailed as follows:
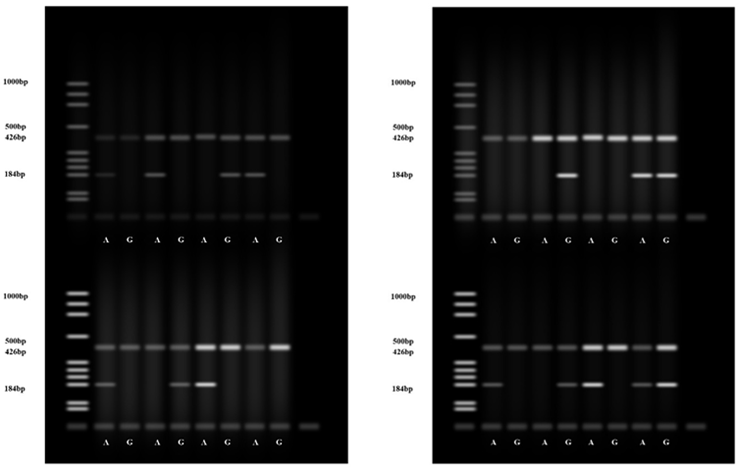
Primer Sequence Base pair size TNF-α-308 (G/A) TCTCGGTTTCTTCTCCATCG - 184bp; TNF-α-308 (G) ATAGGTTTTGAGGGGCATGG - 184bp; TNF-α-308 (A) AATAGGTTTTGAGGGGCATGA - 184bp; Growth factor Forward Primer- CCTTCCAACCATTCCCTTA - 426bp; Growth factor Reverse Primer- TCACGGATTTCTGTTGTGTTTC - 426bp For each sample there were two lanes representing A and G alleles, each lane was labeled after the possible polymorphism. The band for each allele was separated at 184 base pair while the Human Growth Factor which served as the internal control were separated at 426 base pair. AA genotype was present where only the A band was visible; GG genotype was represented where only G band was visible and AG genotype where both bands were visible (Figure 1).
Statistical Analysis
Descriptive analysis and One-way Analysis of variance were used to compare data. Pearson’s correlation coefficient (r) was used to determine the association between variables. Odds ratio (OR) and 95 % confidence interval were computed. p < 0.05 was considered significant.
Results
The mean ages of obese and non-obese subjects were 38.57±0.90 and 39.22±0.93 years (p>0.05), all female participants have a mean age of 37.54 years while their male counterparts were aged 43.63 years respectively. The mean values of body weight, height, body mass index and waist circumference of the non-obese group were significantly increased compared to that of obese subjects (Table 1).
| Obese(n=200) | Non-obese (n=197) | p-value | |
|---|---|---|---|
| Body Weight (kg) | 81.92±1.00 | 72.03±1.01 | 0.001* |
| Height (m) | 1.57±0.01 | 1.81±0.01 | 0.001* |
| BMI (kg/m2) | 33.01±0.25 | 22.06±0.22 | 0.001* |
| WC (cm) | 86.65±1.54 | 82.65±1.04 | 0.030* |
| HC (cm) | 98.01±1.10 | 96.92±1.05 | 0.47 |
| WHR (cm) | 0.87±0.01 | 0.86±0.01 | 0.53 |
| SBP (mmHg) | 114.35±0.69 | 113.99±0.57 | 0.74 |
| DBP (mmHg) | 76.55±0.58 | 75.59±0.68 | 0.97 |
| FBS(mmol/L) | 4.77±0.66 | 4.65±0.70 | 0.77 |
Table 1: Anthropometric, Phenotypic Parameters and FBS levels among Obese and Non-obese Subjects (mean ±SD). *significant at p<0.
Table 1: Anthropometric, Phenotypic Parameters and FBS levels among Obese and Non-obese Subjects (mean ±SD). *significant at p<0.05(female obese vs non-obese) #significant at p<0.05 (male obese vs non-obese) WC - Waist Circumference; HC - Hip Circumference; WHR - Waist Hip Ratio; SBP - Systolic Blood Pressure; DBP - Diastolic Blood Pressure; FBS - Fasting Blood Sugar There were no significant differences in the mean age distribution among the female obese (37.55±0.89) and non- obese (37.54±0.94) as well as the male obese (48.89±2.56) and non-obese subjects (48.40±1.75) at p>0.05. The mean BMI, SBP and FBS values were increased among the male obese compared to non-obese subjects (p<0.05) while mean body weight, BMI, WC, HC were significantly increased in obese than non-obese females (Table 2).
| Female | Male | |||
|---|---|---|---|---|
| Group/Parameters | Obese (n=136) | Non-obese (n=122) | Obese (n=64) | Non-obese (n=75) |
| Age | 37.55±0.89 | 37.54±0.94 | 48.89±2.56 | 48.40±1.75 |
| Body Weight (Kg) | 82.03±1.07 | 71.87±1.12* | 80.78±2.27 | 72.93±2.43# |
| Height (cm) | 1.57±0.01 | 1.80±0.01 | 1.59±0.02 | 1.83±0.03 |
| BMI(Kgm2) | 33.13±0.27 | 22.09±0.25* | 31.79±0.44 | 21.85±0.48# |
| WC (cm) | 86.56±1.64 | 82.15±1.10* | 87.56±4.71 | 85.40±3.10 |
| HC (cm) | 97.86±1.17 | 96.65±1.15* | 99.56±3.32 | 98.40±2.67 |
| WHR | 0.86±0.01 | 0.85±0.01 | 0.90±0.05 | 0.90±0.04 |
| SBP (mmHg) | 113.74±0.73 | 113.66±0.83 | 120.56±1.02 | 115.80±2.93 |
| DBP (mmHg) | 76.30±0.60 | 76.93±0.77 | 79.11±2.06 | 74.73±1.09 |
| FBS(mmol/L) | 85.58±0.67 | 84.92±0.77 | 88.78±2.86 | 89.27±1.48* |
Table 2: Genotypic Frequency Distribution of TNF-α308 in all subjects *significant@p<0.05 Differences in anthropometric parameter
- *significant at p<0.05(female obese vs non-obese)
- Genotypic distribution among the obese group showed a highest frequency of homozygous AA genotype (51%) followed by AG (43%) then wild type GG (6%). heterozygous
- AG genotype had the highest distribution among the non-
- Variable
- Obese
- Non-obese
- Total
- OR
- (95% CI)
- AA
- 102 (51%)
- 22 (11.17%)
- 124(31.23%)
- 8.137
- (3.882 - 17.060)*
- TNFα
- AG
- 86 (43%)
- 127 (64.47%)
- 213(53.65%)
- 0.4071
- (0.229 - 0.724)*
- GG
- 12 (6%)
- 48 (24.37%)
- 60(15.11%)
- 0.2054
- (0.079 - 0.530)
- Total
- 200
- 197
- 397
Table 3: Genotypic Frequency Distribution of TNF-α308 in all subjects
| Groups | Obese (n=200) | Non-obese (n=197) | ||||||
|---|---|---|---|---|---|---|---|---|
| Genotypes/Parameters | AA (n=102) | AG (n=86) | GG (n=12) | p | AA (n=22) | AG (n=127) | GG (n=48) | P |
| FBS (mmol/L) BW (kg) | 86.14± 0.93 | 85.14± 0.97 | 88.83± 3.47 | 0.408 | 85.09± 2.47 | 85.97± 0.86 | 84.78± 1.41 | 0.761 |
| 82.14± 1.39 | 81.67± 1.57 | 81.83± 3.91 | 0.975 | 68.82± 2.68 | 72.44± 1.27 | 72.43± 2.14 | 0.53 | |
| Height (m) BMI (kg/m2) | 1.58±0.01 | 1.57±0.01 | 1.57±0.04 | 0.667 | 1.81±0.03 | 1.80±0.02 | 1.81±0.03 | 0.928 |
| 32.92± 0.36 | 33.35± 0.38 | 33.17± 1.05 | 0.714 | 21.00± 0.59 | 22.30± 0.28 | 22.04± 0.45 | 0.189 | |
| WC(cm) | 86.65± 2.18 | 86.42± 2.42 | 88.33± 5.3 | 0.961 | 81.09± 2.42 | 83.27± 1.42 | 81.70± 1.72 | 0.716 |
| HC(cm) | 98.41± 1.6 | 97.56± 1.67 | 97.87± 3.42 | 0.933 | 93.73± 1.94 | 96.43± 1.3 | 99.79± 2.41 | 0.23 |
| WHR | 0.86±0.02 | 0.88±0.02 | 0.84±0.03 | 0.596 | 0.86±0.02 | 0.87±0.01 | 0.83±0.01 | 0.174 |
| SBP mmHg | 114.43± 1 | 114.40± 1 | 113.33± 3.85 | 0.935 | 114.09± 2.43 | 114.84± 0.86 | 111.61± 2.3 | 0.268 |
| DBP mmHg | 77.67± 0.9 | 75.44± 0.77 | 75.00± 1.44 | 0.141 | 75.82± 1.44 | 77.41± 0.87 | 74.70± 1.37 | 0.23 |
Table 4: Comparison of TNF-α308 Genotypes and FBS/anthropometric parameters in all subjects.
Discussion
Worldwide, more than 3 million deaths were related to overweight and obesity [4]. Chronic Inflammation accompanied with high levels of proinflammatory cytokines such as TNF-α, is an important feature of obesity [10]. This case-control study investigated the relationship of TNF-α 308G/A polymorphism, phenotypic and anthropometric parameters with obesity among a population of Southwestern Nigeria. Our findings in this study did not show a significant difference in mean age distribution within the obese and non-obese groups. This is at variance with a report that showed increased obesity in older adults [11]. A possible explanation for the disparity in the results could be due to small sample size. It was previously suggested that increased hormonal changes and inactive lifestyle common with aging increases risk of developing obesity. In addition, muscle mass tends to reduce with age [12] giving rise to decreased body metabolism. Data from this study showed that obesity has a female preponderance with higher mean BMI recorded among obese females compared to males. This finding is in agreement with earlier studies that found an association between TNF-α levels and obesity risk in women [3, 13]. Tumor Necrosis Factor - α has two regions G-308A and G-238A of which 308 is a promoter region for TNF- α and has been linked with increased TNF- α production in adipose tissue which is implicated in pathogenesis of obesity [9]. Waist and hip circumferences are important estimations in predicting cardiovascular disease occurrence in obesity with increased WC and decreased HC associated with increased risk of obesity-related mortality [14, 15]. We recorded a contrasting observation of lower WC among our study participants. This coupled with the non-significant differences of FBS and measured anthropometric parameters in the TNF- α G-308A genotypes suggests that our subjects are at reduced risk of developing cardio-metabolic disorders associated with obesity. We hope to establish this in a further investigation involving a larger sample size.
The G-308A mutation in the promoter region of TNF- α acts as a potent transcriptional activator resulting in higher TNF- α concentrations with consequent reduction in insulin sensitivity [16, 17]. Genotyping of TNF-α 308 loci in this present study showed that the distribution of homozygous genotype AA was higher among obese than non-obese participants while the AG genotype showed a higher frequency in the non-obese. This is similar to results from an investigation that reported an association between AA genotype and increased TNF- α expression with obesity[7] but at variance with another that linked heterozygous TNF-a-308 G>A gene polymorphism to higher risk of developing obesity and associated disorders [18].
Obese carriers of the TNF- α 308 A allele have been shown to be more susceptible to increased effect of dyslipidemia and development of insulin resistance [17]. However, the mean FBS value (4.77±0. 66 mmol/l) of the obese participants of this study was not up to the fasting glucose diagnostic criteria for diabetes mellitus of ≥7.8 mmol/l [19] suggesting that the subjects did not develop insulin resistance nor diabetes mellitus, both metabolic consequences of obesity. Findings from this study also showed a higher occurrence of GG genotype among the non-obese controls than the obese group thereby indicating a weak association of GG with obesity. A similar observation reported that the odd of being obese was lower in individuals with G/G genotype [3] and at variance with another [20].
Results of this study revealed that AA (51%) and AG (43%) genotypes show a trend for association (OR = 0.4071, 8.137, p<0.05) in the obese participants. Another study also reported increased risk of developing obesity among participants with AG and AA genotype. And that TNF- α 308 G/A gene polymorphism reconciles the relationship between dietary fat intake and obesity risk [3] while another reported no associations [21]. Significant changes in TNF- α 308 G/A gene polymorphism observed among our studied population suggests that AG genotype was not independently associated with obesity.
Conclusion
It could be hypothesized from our observations that AA genotype of TNF- α 308 may be a predisposing factor for development of obesity whereas GG genotype did not show a significant association (p>0.05) with obesity in our study population. We suggest a more detailed dietary –genetic interaction based study to establish the contributions of TNF- α 308 G/A gene polymorphism to obesity among a larger cohort in our study population. This is important in predicting susceptibility to obesity for quick intervention.
References
-
Sikaris KA (2004) The Clinical biochemistry of obesity. The Clinical Biochemist Reviews 25(3): 165-181.
-
Milagro FI, Mansego ML, Miguel CD, Martinez JA (2013) Dietary factors, epigenetic modifications and Obesity outcomes: progresses and perspectives. Molecular Aspects of Medicine 34(4): 782-812.
-
Joffe YT, Merwe LVD, Carstens M, Collins M, Jennings C, et al. (2010) Tumor necrosis factor alpha gene-308 G/A polymorphism modulates relationship between dietary fat intake, serum lipids and obesity risk in Black South African women. The Journal of Nutrition 140(5): 901- 907.
-
Adeloye D, Ige-Elegbede JO, Ezejimofor M, Owolabi EO, Ezeigwe N, et al. (2021) Estimating the prevalence of overweight and obesity in Nigeria in 2020: a systematic review and meta –analysis. Ann Med 53(1): 495-507.
-
Ogundele OE, Adekoya KO, Osinubi AA, Awofala AA, Oboh BO (2018) Association of adiponectin gene (ADIPOQ) polymorphisms with measures of obesity in Nigerian young adults. Egyptian Journal of Medical Human Genetics 119(2): 123-127.
-
Tsigos C, Kyrou I, Chala E (1999) Circulating tumor necrosis factor alpha concentrations are higher in abdominal versus peripheral obesity. Metabolism 48(10): 1332-1335.
-
Brand E, Schorr U, Kunz I, Kertmen E, Ringel J (2001) Tumor necrosis factor-α-308 G/A polymorphism in obese Caucasians. International Journal of Obesity 25(4): 581-585.
-
Amole IO, Adeniran A, Awotunde OT, Durodola OA, Oyelade BO (2014) The Prevalence of Adult Obesity in Ogbomoso, Southwest Nigeria. Research Journal of Health Sciences 2(3): 34-43.
-
Hedayati M, Sharifi K, Rostami F (2012) Association Between Tumor Necrosis Factor alpha Promoter G-308A And G-238A Polymorphisms And Obesity. Mol Biol Rep 39(2): 825-829.
-
Qasim AQ, Fareed YY, Hassan JK (2017) Evaluation of inflammatory state in diabetic patients by measuring interleukin-6 and TNF-α in obese and non-obese type 2 diabetes mellitus patients. Iraqi JMS 15(3): 297-304.
-
Batsis JA, Zagaria AB (2018) Addressing obesity in aging patients. Med Clin North Am 102(1): 65-85.
-
Sayer AA, Syddal H, Martin H, Patel H, Baylis D (2008) Developmental origins of sarcopenia. J Nutr Health Aging 12(7): 427-432.
-
Hoffsted J, Ericksson P, Hellstrom L, Rossner S, Ryden M (2000) Excessive fat accumulation is associated with TNF- Α 308 G /A promoter polymorphism in women but not men. Diabetologia 43(1): 117-120.
-
Depres JP, Lemiex I, Prud’homme D (2001) Treatment of obesity: need to focus on high risk abdominally obese patients. BMJ 322(7288): 716-720.
-
Cameron AJ, Magliano DJ, Shaw JE, Zimmet PZ, Carstensen B, et al. (2012) The influence of hip circumference on the relationship between abdominal obesity and mortality. Int J Epidemiol 41(2): 484-494.
-
Nieto-Vazquez I, Fernandez-Veledo S, Kramer DK, Vila- Bedmar R, Garcia-guerra l (2009) Insulin resistance associated to obesity: the link TNF-alpha. Arch Physiol Biochem 114(3): 183-194.
-
Vikram NK, Bhatt SP, Bhushan B, Luthra K, Misra A, et al. (2011) Associations of -308G/A polymorphism of TNF- alpha gene and serum TNF-a levels with measures of obesity, intra-abdominal and subcutaneous abdominal fat, insulin resistance in Asia Indians. Disease Markers 31(1): 39-46.
-
Chang W, Wang Y, Chen C, Zhang S, Liu C, et al. (2012) 308G/A of tumor necrosis factor-α and 825C/T of guanidine nucleotide binding protein3 are associated with the onset of acute MI and obesity in Taiwan. Int J Mol Sci 13(2): 1846-1857.
-
WHO (2019) Classification of diabetes mellitus. World Health Organization, pp: 36.
-
Um JY, Park JH, Kim HM (2003) Gene polymorphisms -in tumor necrosis factor alpha locus and waist hip ratio in obese Koreans. Clin Chim Acta 338(1-2): 117-122.
-
Romeo S, Sentinelli F, Capici F, Arca M, Berni A, et al. (2001) The G -308A variant of TNF- alpha gene is not associated with obesity, insulin resistance and body fat distribution. BMC Med Genet 2: 10.
- Assessing the Accuracy of Refractive Prediction of Different IOL Formulas in Medium Long Eyes
- The Effect of Imatinib on the Fetus Growth and Development of a Pregnant Woman Involved with CML, a Case Report and a Literature Review
- Acquired Neutropenia and Fever, its Treatment and Complications in an Infant, A Case Report
- Coccidioidomycosis with Laryngeal Nodule and Cavitary Lung Disease: A Case Report
- Hodgkin Lymphoma in a Girl with Common Variable Immune Deficiency: A Case Report and Review of Literature
- Public Administration and the Management of Beliefs in Risks and Dangers in the COVID-19 Era