Safety and Efficacy of a Combination Therapy (Autologous Bone Marrow Derived Mononuclear Cells and Umbilical Cord Derived Mesenchymal Stem Cells) in Duchenne Muscular Dystrophy Patients
Duchenne muscular dystrophy is a neuromuscular disorder caused due to mutations in dystrophin gene. It is characterized by progressive muscle degeneration; cellular therapies pose as a possible treatment option for this debilitating disorder. Earlier many cellular therapies with autologous and allogenic stem cells have provided evidences of their efficacy in the treatment of DMD. This study was carried out in different hospitals of India to prove the safety & efficacy of combination of autologous and allogenic stem cells in DMD patients. 30 patients were enrolled of which 18 were in the treatment group and 12 in the control group. Patients from each treatment group were given 4 sessions; 1 with autologous BM-MNCs and 3 with allogenic UC-MSCs. Assessments were done on the basis of Muscle strength, Functional Independence scale, Brooke and Vignos scales. Among the treatment group, 77.7% patients showed positive response. There was 63% and 50% rise in upper and lower limb’s power respectively after the completion of the protocol in the treatment group. When control group (n=12) was compared with treatment group (n=18), it was observed that the muscle strength in upper and lower limbs declined from the baseline by 41% and 47% respectively. Furthermore, Functional-Independence Measure score and Brooke-Vignos score also improved, suggestive of the efficacy of the treatment.So, the combination therapy has shown significant improvement in the muscle strength of the DMD patients compared to untreated group, without causing any deleterious effects. Therefore this combination therapy may be effective and safe option to be considered for therapeutic use in DMD patients.
Introduction
Duchenne muscular dystrophy (DMD) is one of the hereditary neuromuscular disorders and a focal reason for the high mortality in children’s [1, 2]. DMD is an X linked recessive disorder which mainly affects male child with the incidence of 1:3500 live births [2, 3, 4]. However, in the rare cases of X skewed inactivation, girls suffer from DMD [5]. The cause of DMD is a genetic abnormality in the gene dystrophin, resulting in faulty or less production of Dystrophin, a cytoskeleton protein. The kinds of mutations occur in DMD gene are classified as Deletion (60-65%), Point mutation (35-40%) and Duplication (5- 6%) which results in partial or complete abnormal Dystrophin protein[6]. The dystrophin gene is the largest in humans and expressed mainly in skeletal and cardiac muscles and in nerve cells to the lesser extent [7, 8]. Dystrophin acts in association of actin filament to the extracellular matrix which stabilizes the sarcolemma and prevents it from mechanical injuries and retain muscle strength [7, 9]. Thus DMD is characterized by the muscle weakness and muscle wasting [7].
The symptoms associated with the disease start to develop during early childhood and in most of the cases patient become wheelchair bound by the age of 10-12 years [2]. Deficiency of Dystrophin results in variation in cognition, behavioral functioning and sleep pattern. It also affects IQ and Verbal memory. Person suffering from DMD is known to have a high risk of Dyslexia, Dyscalculia, and Dysgraphia [3]. In the patients with DMD, the muscle mass become replaced by fatty and fibrous tissue. The patient often posses symptoms like delayed walking, frequent falls, and difficulty in running and climbing in the initial phases. With the progression of disease, muscle around calf, pelvis and thigh appear bulkier than normal at the same time other health complications such as scoliosis, muscular contractures, and cardiomyopathy arise [2, 10].
Assessment of the disease to ensure the severity is a pivotal aspect of the management of DMD. There are different parameters used for an assessment which primarily includes Manual Muscle Testing (MMT), Muscle biopsy, MRI, Gowers’ sign, serum creatine kinase (CK) levels etc [11]. High rate of mortality due to DMD accounts for unavailability of appropriate treatment option. In spite of medical advances, DMD remains an incurable physiological disorder. However to prolong the ambulation and prevent secondary complications, certain supportive treatment strategies have been tried and implemented. Until now corticosteroids are the only available drug per say for delaying the muscle degeneration. However, corticosteroids being an immune suppressor pose many other side effects that deteriorate the health of the patient [2, 12]. An aggressive physical treatment, rehabilitation, endocrine and gastrointestinal care is possible method to delay the muscle degeneration. However these methods do not cure the disease and also cannot be used for the longer period of time [13, 14].
Due to the inefficiency of the corticosteroids and other treatments, medical communities started exploring the alternative treatment methods. With the emergence of the stem cells, especially mesenchymal stem cells and its effective use in various diseases, researchers have explored the usefulness of MSCs in DMD as well [15]. The MSCs and other stromal cells like fibroblasts showed the similar characteristics thus some scientists refer to the stromal cells as mesenchymal stromal cells [16, 17, 18, 19].
These MSCs were initially derived from Bone marrow but later on it was discovered that adipose tissue, placenta, skin, umbilical cord blood, umbilical cord perivascular cells, umbilical cord Wharton’s jelly, Dental pulp, Amniotic fluid, Synovial membrane, and Breast milk are also the rich source of MSCs [19, 20]. The unique characteristics that defines MSCs are plastic adherence, surface marker phenotype (CD105+, CD73+, CD90+, CD45−, CD34− CD14−, CD19−, CD3−, HLA DR−) and tri- lineage (osteocytes, chondrocytes and adipocytes) differentiation capacity [21].
Various pre-clinical studies with cord derived allogenic MSCs have provided an evidence that this population can be effectively used in small animal models for DMD without the risk of Graft Versus Host Disease (GVHD) which proves safety of this cells [22, 23]. These properties of MSCs make them a suitable candidate for their use in treatment of patients with DMD. In DMD, as mentioned earlier there is necrosis of muscle cells which leads to muscle degeneration. Local stem cell population which is termed as Satellites aids in repair and regeneration of the damaged tissue. However, the rate at which tissue is damaging in DMD is far way high to the rate at which local stem cells repairing the damaged tissue. Thus, leading to the muscle degeneration and wasting. Hence, efforts were made to replenish this local stem cell population to repair or reduce the damage. [2, 24, 25].
The present study was carried out with an objective of assessing the safety and efficacy of the combined therapy of autologous bone marrow derived MNCs (BM-MNCs) and umbilical cord derived MSCs (UC-MSCs) in DMD patients. Various studies have been carried out with these cells population individually and affirmative results were obtained. However, novelty of this study lies in the attempt of using combination of these two different cell types.
Materials and Methods
Patient Selection and Study
This study was a medium term retrospective analysis carried out from July 2015 to July 2017 in three different hospitals in India. About 30 patients were the part of this study after inclusion and exclusion criteria. Enrolled patients were divided in two groups. Group A and group B, Group A was the test group containing 18 patients and remaining 12 patients were part of control group B. Test group (group A) received the combination therapy (BM- MNCs+UC-MSCs) whereas control group did not receive any standard treatment procedures like steroids or rehabilitation and at the end of the study comparative analysis were done to assert an effectiveness of the therapy. An informed consent was taken from parents/relatives of enrolled patients after giving them complete information about trial procedures.
Before the study, a complete initial assessment of the patient was performed by the experienced doctors. After every session, participants received a physical therapy.
Inclusion Criteria
Patients within the age group of 5 to 21 years with known case of a DMD were included, with confirmed diagnosis by family history of DMD, by genetic testing, amount of functional Dystrophin protein in their muscle biopsies, and with higher CPK values higher than 1200 (U/L). Patients whose cytogenetic analysis showed exon deletion of dystrophin gene were also included in this study.
Exclusion Criteria
Patients who were undergoing corticosteroids treatment and those with any other complications or life threatening diseases such as HIV/HBV/T.B., Cancer etc. were excluded for this study. The patient who have undergone any stem cell procedures or any other cell transplantation for past 6 months were also excluded.
Clinical Assessment Parameters
The entire protocol session comprised of 4 interventions 1st was autologous bone marrow derived mononuclear cells and then 3 sessions of UC-MSCs. A complete neurological and physical evaluation was performed for all the patients. The clinical parameters included Muscle strength grading of the upper and lower limbs [26, 27], Functional Independence Measure (FIM) [28], Brooke and Vignos scale [28], Gowers’ sign, CPK values, along with Pulmonary function test (PFT), MRI of Pelvis/Calf, 2D Echo. These parameters were again assessed at different intervals of 1 month, 3 months, 6 month and 1 year. These clinical findings before and after the combination protocol were compared to evaluate the efficacy of the protocol.
Autologous Bone Marrow Derived Mononuclear Cells (BM−Mncs) Isolation
All patients underwent a bone marrow aspiration under local anesthesia; about 80–100 ml of bone marrow was collected from posterior iliac crest of donor in collection bag (Terumo Penpol) containing CPDA to prevent clotting. Collected bone marrow samples were transported to processing laboratory in proper temperature controlled conditions and samples were processed using previously stated procedures with some modifications by density gradient method [26]. The required volume of the BMMNCs was prepared and sent to the hospital for administration. The quality analysis like MNC count, viability and sterility testing of the isolated cell population was performed. The sterility testing was carried out for both bacterial and fungal contamination, Fluid Thioglycollate medium was used for bacterial contamination and Sodium Casein Digest Medium was used for fungal.
Allogenic Umbilical Cord Derived Mesenchymal Stem Cells Isolation (UC-Mscs)
Human Umbilical Cord derived mesenchymal stromal cells were cultured in the ReeLabs Pvt Ltd, Mumbai, India. The cells were cultured according to the standard operating procedure of the laboratory using tissue digestion method from Wharton’s jelly and cryopreserved in required cell doses. The umbilical cord tissues were minced into 1-2 mm3 fragments and incubated with 0.75% collagenase Type iv (Gibco), Dispase II (Sigma) for 45 minutes and followed by Trypsol-AOF (Biogenomics) for 30 minutes with gentle agitation at 370C. The digested mixture was filtered using 100 µm cell strainer (BD falcon) to obtain single cell suspension. The cells were plated at a ratio of 10000 cells per cm2 in T 75 culture flask using serum free Medium without phenol red (Promocell). The flasks were trypsinized and sub cultured upon confluency to get the required number of cells. Flow Cytometry (Becton Dickinson, USA) was used to assess the immunoprofile of cultured umbilical cord mesenchymal stem cells, using the standard for MSC described by the position paper of the International Society for Cellular Therapy (ISCT). One million cells of each population were used for flow cytometry. Cells were stained with conjugated FITC or PE or PerCp or APC antibodies against CD34, CD45, CD90, HLA-DR, CD105 (ImmunoTools, Germany), and CD73 (Becton Dickinson and Company, USA). An appropriate isotype-matched control antibody was used in all analyses. Cells were analysed on FACS scan flow cytometer using Cell Quest Software (Becton Dickinson, USA). The cryopreserved vials containing UC-MSCs were sent to the hospital for administration according to the mentioned cell dose.
BM-MNCs Therapy
All the therapeutic procedures were performed in operation theatres under absolute aseptic conditions. The Intrathecal and Intramuscular injections were carried out with BM-MNC as per the protocol. After first session the patients were advised to revisit for the next session after one month. Some patients complained of mild fever and body ache however, no major complications were observed after the first session.
Allogenic UC-MSCs Therapy
After one month of the BM-MNCs administration, intramuscular and intravenous injections of allogenic UC- MSCs were administered at the concentration of 2-3 million per kg body weight. The UC-MSC vials received were thawed according to the standard operating procedure given by ReeLabs Pvt Ltd and the thawed vials containing UC-MSCs were infused. UC-MSC sessions were repeated at the interval at 1,3 and 6 months. At each time, before the administration of cells, assessment based on above mentioned parameters were noted.
Both of these procedures were performed with the consent of patient as well as their families. After the end of each session patients were given the standard supportive care in the respective hospitals.
Statistical Analysis
All the statistical analysis was carried out by using paired t-test method in R software. The data is expressed in Mean±SD (standard deviation).
Results
The collected bone marrow samples were transported to laboratory and processed according to above mentioned procedure. The MNC count for isolated mononuclear cells was in between 600-900 million, with 97-99% viability. The sterility testing results showed no growth for all samples. The isolated cells were adjusted to the required volume after all the quality analysis and were sent to hospital for infusion. Similarly the UC-MSCs were cultured and cryopreserved in 20 million in 2 ml per cryovial. The frozen cryovials were sent to hospital for infusion based on the patient’s body weight at the ratio of 2-3 million per kg body weight. The cultured UC-MSCs showed a typical ‘fibroblast’ like morphology under the microscope for all cultures. The UC-MSCs expressed cell surface markers namely CD90, CD73 and CD105 and were negative for CD34, CD 45 and HLA-DR. The average viability of all MSCs was above 98% by flow cytometry. Our observations are in line with the ISCT guidelines on MSC identification. Regardless of the source of MSCs, they were found to be positive for cell surface markers CD90, CD73 and CD105 and negative for CD34, CD45 and HLA- DR. However the differentiation potential studies were not carried out for the cultured cells.
Clinically diagnosed DMD patients (n=18) were treated with a combination therapy of bone marrow derived mononuclear cells (BM-MNCs) and Umbilical Cord derived Mesenchymal stromal/stem cells (UC-MSCs) and followed up to 1 year. There were no adverse events documented after the therapy or during the follow up sessions. At the end of each session, all patients were given the physiotherapy.
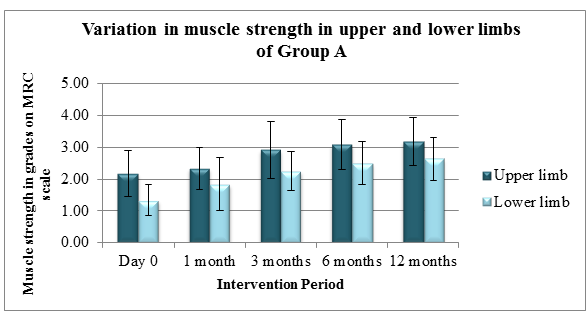
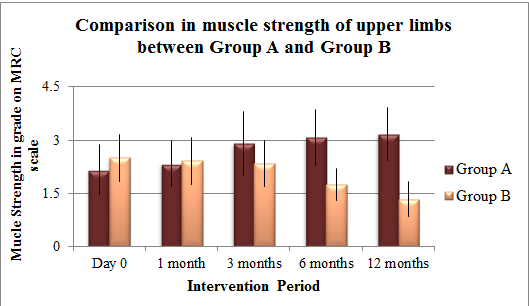
Muscle charting score of Group A (treatment) was compared with that of Group B (control) at all the interventions. The baseline muscle strength of group A (n = 18) was 2.17±0.72 in upper limbs while 1.33±0.49 in lower limbs. Group B (n = 12) on the other hand had baseline muscle strength as 2.50 ± 0.67 and 1.67 ± 0.65 in upper and lower limbs respectively (Tables 1 & 2).
| Duration | Group A | Group B | ||||||
|---|---|---|---|---|---|---|---|---|
| Day 0 | 2.17 (±0.72) | 2.50 (± 0.67) | ||||||
| 1 Month | 2.33 (±0.65) | 2.42 (± 0.67) | ||||||
| 3 Months | 2.98 (±0.90) | 2.33 (± 0.65) | ||||||
| 6 Months | 3.08 (± 0.79) | 1.75 (± 0.45) | ||||||
| 12 Months | 3.18 (± 0.75) | 1.33 (± 0.49) |
Table 1: Baseline Muscle strength in group A and group B in upper limbs.
| Duration | Group A | Group B | ||||||
|---|---|---|---|---|---|---|---|---|
| Day 0 | 1.33 (±0.49) | 1.67 (± 0.65) | ||||||
| 1 Month | 1.83 (±0.83) | 1.67 (± 0.65) | ||||||
| 3 Months | 2.25 (± 0.62) | 1.67 (±0.65) | ||||||
| 6 Months | 2.50 (± 0.67) | 1.50 (± 0.67) | ||||||
| 12 Months | 2.64 (± 0.67) | 1.25 (± 0.62) |
Table 2: Baseline Muscle strength in group A and group B in lower limbs.
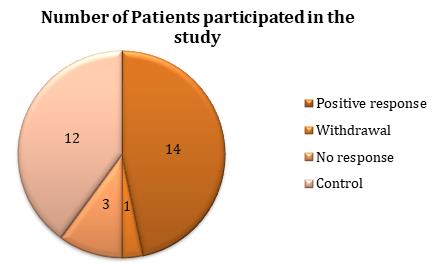
Out of 18 patients in group A (Figure 1), one of them had withdrawn from the study after the 1st session. Amongst the remaining candidates, 3 of them did not show any positive response but, there was no decline observed in their overall muscle strength, FIM scores and Brooke Vignos scores. Almost 77.7% of the patients showed a positive response and improvement in the assessed parameters over a time.
Out of 30 participants, 18 were the part of Group A and 12 were the part of Group B. out of 18, 14 showed a positive response to the treatment, 1 participant withdrawn from the study and 3 showed no response to the treatment.
Almost after a year, the muscle strengths in upper and lower limbs in 14 patients from group A were 3.18±0.75 and 2.64±0.67 respectively. Hence there was 63% and 50% rise in the muscle power of upper and lower limbs respectively of these patients (Figure 2). Statistically there was a significant difference in p values of upper limbs and lower limbs.
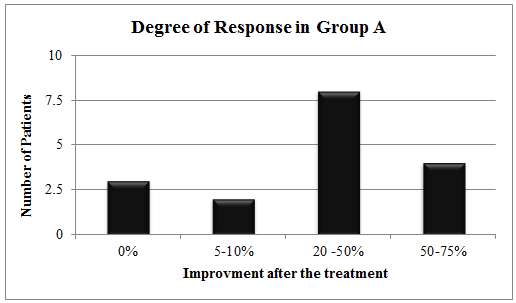
Muscle strength in upper and lower limbs was measured in DMD patients (n=14) over a period of time after each intervention. Medical Research Council (MRC) muscle grading scale (1-5) was used for an evaluation. Patients were also examined on the basis of the degree of improvement they showed after the therapy (Figure 3). Out of 17 patients, 3 showed no response, 8 patients showed mild improvement where only 1 unit increase was seen in the strength of either upper or lower limbs. 2 patients showed moderate improvement in which both the limbs showed 1 unit rise in the muscle strength and 4 patients showed significant improvement where in 2 unit rise was noted in either of the limbs.
Patients were categorized on the basis of 4 degrees of responses that they have shown. 0% response signifies no increase in the muscle power, 5-10% means increase in one unit in either of the limb’s muscle power, 20-50% indicates increase in 1 unit in both the limb’s muscle power, 50-75% signifies 2 unit increases in muscle power of either of the limbs at the end of the protocol.
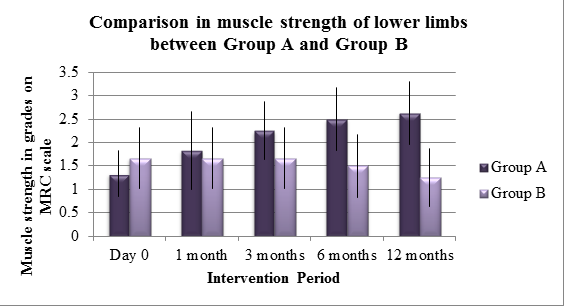
When muscle powers in upper and lower limbs amongst these two study groups were compared, it was seen that the control group showed a vast deterioration in their muscle power; whereas treatment group showed an improvement in the muscle power over a period of time. Upon statistical comparison, it can be stated that the muscle strength in upper and lower limbs amongst these two group differ significantly with the p values of 0.02979 and 0.1435 in upper and lower limbs respectively. The baseline in muscle strength for both the groups was almost similar. However, over a period of time control group showed a decline in the muscle strength. Upper limb power of control group showed 41% decline while, 47% decline was seen in lower limb strength (Figures 4 & 5).
The effectiveness of the treatment was determined by comparative study of the muscle strength between the control group B (n=12) and treatment group A (n=14). Medical Research Council (MRC) muscle grading scale (0- 5) was used for estimation.
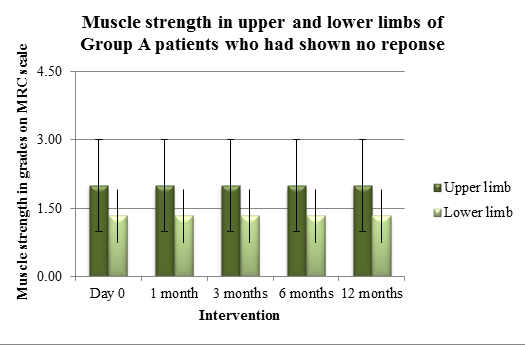
- The effectiveness of the treatment was determined by comparative study of the muscle strength between the control group B (n=12) and treatment group A (n=14).
- Medical Research Council (MRC) muscle grading scale (1-
- 5) was used for estimation.
- Duration Muscle strength in
- Muscle strength in upper limbs lower limbs
- Day 0
- 2.00±1
- 1.33±0.58
- 1 Month
- 2.00±1
- 1.33±0.58
- 3 Months
- 2.00±1
- 1.33±0.58
- 6 Months
- 2.00±1
- 1.33±0.58
- 12 Months
- 2.00±1
- 1.33±0.58
Table 3: Muscle strength in the patients who showed no
When the muscle power of 3 patients who showed no response were observed, it can be depicted that no deterioration was occurred and the muscle strength was maintained over a time. The baseline strengths in those patients were 2.00±1 in upper limbs and 1.33±0.58 in lower limbs were maintained throughout the study period (Table 3 & Figure 6).
Muscle strength in upper and lower limbs of the patients was used as an assessment parameter. The graph represents the data of the 3 patients who did not show any improvement at the end of the treatment.
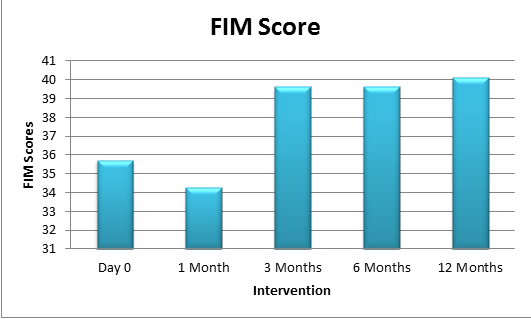
The patients were also assessed on the basis of their ability to daily activities i.e. (Functional Independence Measure) FIM and Brooke and Vignos scale. Increase in the FIM scores and decrease in the Brooke-Vignos scores signifies an improvement. The data obtained from the 14 patients from group A showed FIM mean scores of 35.71 before transplantation, which then increased to 40.14 at the end of 1 year (Table 4 & Figure 7). Functional measure score was examined for the assessment of the patients. Comparative analysis was done to ensure the efficiency of the treatment.
| Duration | FIM Score | ||||
|---|---|---|---|---|---|
| Day 0 | 35.71±12.00 | ||||
| 1 Month | 34.28±13.15 | ||||
| 3 Months | 39.64±14.39 | ||||
| 6 Months | 39.64±14.39 | ||||
| 12 Months | 40.14±14.93 |
Table 5: FIM score in Group patients.
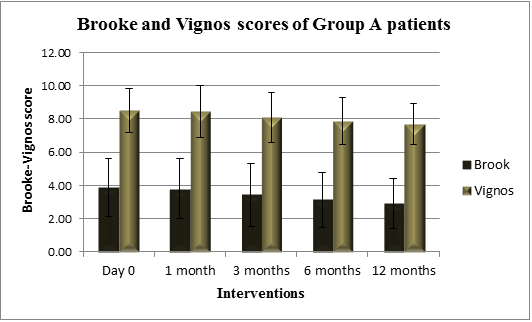
Upon comparing Brooke and Vignos scores before and after the treatment, it can be illustrated that there was a 75% and 90% decrease in Brooke and Vignos score respectively (Table 5 & Figure 8). Brooke score for upper limb strength and Vignos score for lower limb strength was analyzed to ensure the efficiency of the treatment.
| Duration | Brooke score | Vignos score | ||||||
|---|---|---|---|---|---|---|---|---|
| Day 0 | 3.86±1.75 | 8.50±1.34 | ||||||
| 1 Month | 3.79±1.81 | 8.43±1.55 | ||||||
| 3 Months | 3.43±1.91 | 8.07±1.49 | ||||||
| 6 Months | 3.14±1.66 | 7.86±1.41 | ||||||
| 12 Months | 2.92±1.50 | 7.69±1.25 |
Table 4: Brooke and Vignos score of Group patients.
Discussion
So far, there is no evidence of efficient DMD treatment protocol available to control the disease progression or to improve the symptoms of disease condition. Currently there are various therapeutic strategies available in management of DMD which are restricted to just prolonging the functional independence of the patient for as long as possible. The medical strategies concentrate on reducing the early inflammatory process and slowing the muscle loss [29, 30, 31, 32]. With new and advanced treatment strategies like exon skipping, gene therapy and Regenerative medicine have shown some hopes in altering the disease process and reducing disease progression thus increasing the survival chances of these patients. Exon skipping can be described as the process whereby a DNA analogue corrects the transcription of dystrophin, skipping the genetic abnormality that leads to incomplete but potentially better functioning protein sequence [33], and Gene therapy aims at introducing the absent dystrophin gene, because of several practical difficulties gene therapy restricted to be being a clinically feasible at present [34]. In Regenerative medicine or cellular therapies, mononuclear cell transplantation has been widely utilized for its myogenic and neurogenic properties [35, 36].
Many researchers have used stem cells isolated from many different sources for the treatment of DMD, but what type of cell is more effective in reducing the disease condition still remains the question. In our study this was one of the reasons why we choose the combination of two different cell types. Apart from this many studies have also suggested that human UC-MSCs were capable of differentiating in myogenic cell population and could limit the muscle degeneration [29].
In initial attempts with allogenic cell population investigators have utilized the myoblastic precursor cells and administered along with immunosuppressant agents. In spite of this combination, rejections were observed and no significant improvement in muscle strength was noted. However, Rajput, et al. [26] in their study with allogenic cell population and growth factor have proven the safety and efficacy of the method in DMD patients [2]. The overall muscle strength was boosted without any adverse effects after the transplantation therapy. On the other hand, autologous stem cell population has provided evidences of their effective usage in various neurological disorders. Sharma, et al. [30] in their study have documented that 85% of the cases of cerebral palsy and 88% cases of other neurological disorders have shown a significant improvement in their status without any adverse effect. Sharma, et al. [30] have also provided an evidence of effective use of autologous bone marrow derived mononuclear stem cells in 125 DMD patients. 86.67% of the patients showed a significant improvement in overall muscle strength [25].
The present study initiated with the aim of determining the safety first and related efficacy of combined therapy of autologous mononuclear cells and allogenic mesenchymal stromal cells (BM-MNCs, UC- MSCs). The changes in upper and lower limb muscle strength, ability to perform daily activities and Brook and Vignos scores have been examined for the assessment. Every patient had a higher strength in their upper limbs as compared to lower limbs. Out of 18 group’s patients, 77.7% cases showed increase muscle strength in both the limbs. Almost every patient showed 1 unit rise in either of the limbs within one month of the transplantation.
Control group B, on the other hand showed vast deterioration in the muscle strength over a period of time. However from our study group, 3 patients who did not show any improvement in their muscle power, no such deterioration were noted in them. This means that stem cell therapy helped them to stabilize their muscle power.
22.2% cases showed significant improvement, followed by 44.4 % cases with moderate improvement, 11.11% cases with mild improvement and 16.6% cases with no improvement were documented.
On comparing other parameters such as FIM, after a year, mean score increase of 4.43 unit was observed overall. Whereas, Brooke and Vignos mean scores showed 0.94 and 0.81 units drop from initial score, indicating a significant improvement in the patient’s muscle power. When the results obtained from present study were compared with previous studies it was noted that there was a 0.33 and 0.45 unit rise in upper and lower limb respectively in Sharma, et al. [30] studies. Rajput, et al. [26] on the other hand provided evidence that there was 0.32 and 1.02 unit rise in the muscle strength of upper and lower limbs respectively. On contrast to this, combination therapy showed that there was a 1.02 and 1.31 unit rises in the muscle power of upper and lower limbs respectively. This increase is way much higher than the results obtained in previous studies with individual cell population.
Thus, in comparison to the individual cell therapies, combination of the autologous and allogenic cell population provided excellent results. Therefore, consolidated therapy of autologous BM-MNCs and Umbilical cord derived MSCs is proven to be an efficient and safe therapy for DMD. Because of the increased muscle strength, the patients suffering from DMD could live a quality life without dependency on others. However, the exact mechanism of the mode of action of these cell populations is still obscure. We believe that the mononuclear cell population in 1st dosage may have homed in an appropriate muscle niche to ensure its effectiveness. Because of which in most of the cases we observed unit increase in muscle strength within a month. On the other hand remaining allogenic MSCs dosages would have acted as booster dosages which would have further provided a significant improvement in DMD patients. However, further research needs to carry out to identify the fate and the exact mechanism of action of the administered stem cells.
Conclusion
The objective of the present study is to prove that the combined cellular therapy using both autologous and allogenic stem cells is efficacious and safe in patients with DMD. This combination therapy successfully demonstrated that BM-MNCs and UC-MSCs treatment protocol may be more effective and safer when compared to other therapies utilized in the past. However, it was a retrospective study where patients were enrolled at different time points with small patient numbers. The further randomized double-blinded study with larger number of patients with different parameters is required to exactly assess and establish the efficacy of this combination therapy.
Data Availability
No additional data were used in this study apart from the mentioned references.
Conflicts of Interest
The author(s) declare(s) that there is no conflict of interest regarding the publication of this paper.
Funding Statement
Self-Funded
References
-
Craig M McDonald (2012) Clinical Approach to the Diagnostic Evaluation of Hereditary and Acquired Neuromuscular Diseases. Phys Med Rehabil Clin 23(3): 495-563.
-
Rajput BS, Chakrabarti SK, Dongare VS, Ramirez CM, Deb KD (2015) Human Umbilical Cord Mesenchymal Stem Cells in the Treatment of Duchenne Muscular Dystrophy: Safety and Feasibility Study in India. J Stem Cells 10(2): 141-156.
-
James Poysky (2007) Behavior patterns in Duchenne muscular dystrophy: Report on the Parent Project Muscular Dystrophy behavior workshop. Neuromuscul Disord 17(2-3): 986-994. _4._ Sarah Marsh, Alison Pittard (2011) Neuromuscular disorders and anaesthesia; Part 2: specific neuromuscular disorders. Oxford University Press on behalf of the British Journal of Anaesthesia 11(4): 119-123.
-
Freilinger M, Schmidt I, Dysek S, Seidl R, Schmidt WM, et al. (2013) Muscle-specific discordant skewing of X- chromosome inactivation leads to different clinical phenotypes of Duchenne muscular dystrophy in two monozygotic female twins. Neuropediatrics 44 - FV1604.
-
Dey S, Senapati AK, Pandit A, Biswas A, Guin DS, et al. (2015) Genetic and Clinical Profile of Patients of Duchenne Muscular Dystrophy: Experience from a Tertiary Care Center in Eastern India. Indian Pediatrics 52(6): 481-484.
-
(2018) DMD gene. Genetic Home Reference.
-
Quan Gao, Elizabeth M McNally (2015) The Dystrophin Complex: structure, function and implications for therapy. Compr Physiol 5(3): 1223- 1239.
-
Pasternak C, Wong S, Elson EL (1995) Mechanical function of dystrophin in muscle cells. J Cell Biol 128(3): 355-361.
-
Ryder S, Leadley RM, Armstrong N, Westwood M, de Kock S, et al. (2017) The burden, epidemiology, costs and treatment for Duchenne muscular dystrophy: an evidence review. Orphanet J Rare Dis 12(1): 79.
-
Elaine Scott (2006) Measurement in Duchenne muscular dystrophy: considerations in the development of a neuromuscular assessment tool. Developmental Medicine & Child Neurology 48(6): 540-544.
-
Angelini C (2007) The role of corticosteroids in muscular dystrophy: a critical appraisal. Muscle Nerve 36(4): 424-435.
-
Wagner KR, Lechtzin N, Judge DP (2007) Current treatment of adult Duchenne muscular dystrophy. Biochim Biophys Acta 1772(2): 229-237.
-
David J Birnkrant, Katharine Bushby, Carla M Bann, Apkon SD, Blackwell A, et al. (2018) Diagnosis and management of Duchenne muscular dystrophy, part 1: diagnosis, and neuromuscular, rehabilitation, endocrine, and gastrointestinal and nutritional management. Lancet Neurol 17(3): 251-267.
-
Nicholas W Marion, Jeremy J Mao (2006) Mesenchymal Stem Cells and Tissue Engineering. Methods Enzymol 420: 339-361.
-
Friedenstein AJ, Chailakhjan RK, Lalykina KS (1970) The development of fibroblast colonies in monolayer cultures of guinea-pig bone marrow and spleen cells. Cell Tissue Kinet 3(4): 393-403.
-
Owen M (1985) Lineage of osteogenic cells and their relationship to the stromal system. In: Peck WA (Eds.), Bone and Mineral Research, New York, Elsevier 3: 1-25.
-
Caplan AI (1991) Mesenchymal stem cells. J Orthop Res 9(5): 641-650. _19._ Urlich Lindner, Jan Kramer, Jurgen Rohwedel (2010) Mesenchymal stromal cells or stem cells: towards better understanding of their biology. Transfused Med Homether 37(2): 75-83. _20._ Keating A (2012) Mesenchymal stromal cells: New directions. Cell stem cells 10(6): 709-716.
-
Edwin M Horwitz, Michael Andreef, Francesco Frassoni (2006) Mesenchymal Stromal cells. Curr Opin Hematol 13(6): 419-425. _22._ Przepiorka D, Anderlini P, Saliba R, Cleary K, Mehra R, et al. (2001) Chronic graft-versus-host disease after allogenic blood stem cell transplantation. Blood 98(6): 1695-1700.
-
Komanduri KV, Couriel D, Champlin RE (2006) Graft- versus-Host Disease after Allogenic Stem Cell Transplantation: Evolving Concepts and Novel Therapies Including Photopheresis. Biol Blood Marrow Transplant 12(S2): 1-6.
-
Sharma A, Sane H, Paranjape, Bhagawanani K, Gokulchandran N, et al. (2014) Autologous bone marrow mononuclear cell transplantation in Duchenne muscular dystrophy a case report. Am J Case Rep 15: 128-134.
-
Sharma S, Sane H, Badhe P, Gokulchandran N, Kulkarni P, et al. (2013) A Clinical Study Shows Safety and Efficacy of Autologous Bone Marrow Mononuclear Cell Therapy to Improve Quality of Life in Muscular Dystrophy Patients. Cell Transplant 22(S1): 127-138.
-
Rajput B, Kulkarni R, Bopardikar A (2018) Retrospective analysis of role of autologous bone marrow derived mononuclear stem cells in the management of degenerative arthritis of knee. J Stem Cell Res Ther 4(2): 22-28.
-
(2018) Manual Muscle Testing Procedures.
-
Yen Mou Lu, Yi-Jing Lue (2012) Strength and Functional Measurement for Patients with Muscular Dystrophy, Muscular Dystrophy. pp: 321-330.
-
Bushby K, Finkel R, Birnkrant DJ, Case LE, Clemens PR, et. al. (2010) Diagnosis and management of Duchenne muscular dystrophy, part 1 diagnosis and pharmacological and psychosocial management. Lancet Neurol 9(1): 77-93.
-
Sharma A, Gokulchandran N, Chopra G, Kulkarni P, Lohia M, et. al. (2012) Administration of autologous bone marrow derived mononuclear cells in children with incurable neurological disorders and injury is safe and improves their quality of life. Cell Transplant 21(S1): 79-90.
-
Yang XF, Xu YF, Zhang YB, Wang HM, Lü NW, et al. (2009) Functional improvement of patients with progressive muscular dystrophy by bone marrow and umbilical cord blood mesenchymal stem cell transplantations. Zhonghua Yi Xue Za Zhi 89(36): 2552-2556.
-
Bushby K, Finkel R, Birnkrant DJ, Case LE, Clemens PR, et al. (2010) DMD Care Considerations Working Group. Diagnosis and management of Duchenne muscular dystrophy, part 2: implementation of multidisciplinary care. Lancet Neurol 9(2): 177-189.
-
Arechavala Gomeza V, Anthony K, Morgan J, Muntoni F (2012) Antisense oligonucleotide-mediated exon skipping for Duchenne muscular dystrophy: progress and challenges. Curr Gene Ther 12(3): 152-160.
-
Konieczny P, Swiderski K, Chamberlain JS (2013) Gene and cell-mediated therapies for muscular dystrophy. Muscle Nerve 47(5): 649-663.
-
Ferrari G, Mavilio F (2002) Myogenic stem cells from the bone marrow: a therapeutic alternative for muscular dystrophy?. Neuromuscul Disord 12(S1): S7-10.
-
Song S, Song S, Zhang H, Cuevas J, Sanchez-Ramos J (2007) Comparison of neuron-like cells derived from bone marrow stem cells to those differentiated from adult brain neural stem cells. Stem Cells Dev 16(5): 747-756.
- Research Progress of Induced Pluripotent Stem Cells and Their Clinical Application Prospects
- Nishan Al-Kamal is the Starting Point of A Feminist Scientist
- Current Concepts and Future Perspectives of Stem Cell Therapy in Peripheral Arterial Disease
- Stem Cell and Oxidative Stress-Inflammation Cycle
- Adipose Derived Mesenchymal Stem Cells Origin, Characteristics and Promises
- Mitochondria Targeted Antioxidants can Improve In Vitro Embryo Production in Buffalo