Use of Umbilical Cord Mesencymal Stem Cells in the Treatment of Severe COVID-19 Pneumonia
A proposed mechanism of severe Corona virus Disease-2019 (COVID-19) is a deregulated innate immune response to an infection with SARS-CoV-2 resulting in cytokine release syndrome (CRS). Mesencymal stem cells (MSC) have been shown to have immunomodulatory effects and may attenuate the CRS. We present 11 cases of severe COVID-19 pneumonia treated with umbilical cord-derived, non-HLA matched MSC administered as four separate intravenous doses, 5×105 cells/kg. Clinical symptoms, measurements of inflammatory mediators and cytokines (IL6, IL10, IFN-γ, TNF-α), and radiological results were recorded for each patient. Although there were large variations in baseline cytokine pattern elevation, all cytokine levels decreased in all patients after the 4 infusions of UC-MSC, albeit in different magnitudes. Seven patients eventually improved in terms of need for supplemental oxygen and/or mechanical ventilation, clinical symptoms, resolution of pneumonia on imaging, and were discharged. Three patients expired, 1 of whom expired before completing the full course of therapy. This limited series of patients showed that UC-MSC therapy down regulates the cytokine storm and may improve clinical status in patients hospitalized with severe COVID-19 pneumonia without any infusion related reaction.
Introduction
Worldwide more than 49 million individuals have been infected with severe acute respiratory syndrome corona virus 2 (SARS-CoV-2), the corona virus causing COVID-19. From the World Health Organization, as of November 6, 2020, a little over 1.2 million deaths have been reported globally [1] and yet to date, there are no current specific drugs or vaccines available to cure patients with COVID-19 infection. Hence, there is a large unmet need for a safe and effective treatment for COVID-19 infected patients, especially the severe cases.
Severe COVID-19 infection may be accompanied by an aggressive inflammatory response with rapid release of large amounts of pro-inflammatory cytokines described as a “cytokine storm” [2, 3, 4]. This cytokine storm is marked by a sudden increase in circulating levels of pro-inflammatory cytokines, particularly IL-6, TNF-α, interferon-γ and G-CSF, MCP-1, MIP1A, IP10, IL-18, and IL-1. In turn, this cytokine release results in an acute influx of various immune cells including neutrophils, macrophages and T cells from the circulations into the tissue sites of infection [5, 6]. This leads to a severe inflammatory process with impairment of the endothelial cell-cell interactions, disruption of vascular barriers, capillary damage and leakage, diffuse alveolar destruction, and acute lung injury that results in a severe form of ARDS, leading to low oxygen saturation levels [7, 8]. Left unchecked, this cascade of inflammatory reactions results in multi-organ failure and death [9].
Mesenchymal stem cell (MSC)-based therapies have attracted much attention because of their powerful self- renewal capability and pluripotency [10, 11]. One of the main functions of MSC is immune regulation, which can alleviate the inflammatory response in the body through immunosuppression [12, 13, 14]. MSC can inhibit the abnormal activation of T lymphocytes and macrophages, and induce their differentiation into regulatory T cell subsets and anti- inflammatory macrophages, respectively. It can also inhibit the secretion of pro-inflammatory cytokines, such as, IL-1, TNF-α, IL-6, IL-12, and IFN-γ, thereby reducing the occurrence of cytokine storms [15, 16]. Safety and effectiveness have been documented in many clinical trials using MSC [17] especially those dealing with immune-mediated inflammatory diseases including acute lung injury/acute respiratory distress syndrome (ARDS) [18, 19] associated with pro-inflammatory cytokine release similar to that of COVID-19. Furthermore, MSC-based therapies demonstrated promising effects in the experimental treatment of ARDS via inhibition of alveolar collapse and cell apoptosis in lung tissue, increased alveolar fluid clearance, regulation of pulmonary vascular endothelial permeability, and regeneration and repair of damaged lung tissues [20, 21, 22]. Those functions of MSC are expected to make it an effective method for the treatment of COVID-19. Recently, umbilical cord MSC were reported to be effective in the treatment of severe COVID-19 patients [2, 23].
Here, we report the use of umbilical cord MSC (UC- MSC) in patients with severe COVID-19, describing their clinical course, laboratory findings and response to UC-MSC treatment.
Materials and Methods
This case series was on 11 patients with COVID-19 infected pneumonia given UC-MSC treatment at The Medical City Hospital, Manila, Philippines from April 2020 to September 2020. All enrolled patients were confirmed by the real-time reverse transcription polymerase chain reaction (RTPCR) assay of HCoV-19 RNA done at The Medical City Hospital. Criteria for eligibility included age of 18 years and older, clinical findings consistent with severe COVID-19 defined by Clinical classification of COVID-19 released by the National Commission of China [24] and clinical diagnosis of cytokine storm/cytokine response syndrome Grade 2 or higher (ASTCT, CTCAE, or Lee criteria) [25]. We excluded patients who had known allergies to stem cell preparations and their components, had expected death within 48 hours, were diagnosed with HIV and active malignancy, and who were pregnant. Informed consents were secured from the patients and the treatment was approved by The Medical City Hospital Ethics Subcommittee on Cellular Therapy.
The source of MSC were isolated from human umbilical cord Wharton’s Jelly, minced into tiny fragments and digested with collagenase and trypsin. UC-MSC were expanded in vitro and characterized by flow cytometry and confocal microscopy, with the ISCT-recommended cell surface marker expression of CD105, CD73 and CD90, and lack of CD34, CD45, CD14, CD11b, CD79a, CD19 and HLA-DR [26, 27]. UC- MSC was screened for blood borne infectious agents such as HIV, hepatitis B and C, EBV, CMV and syphilis. Aliquots of MSC cells were also cultured to detect contamination by bacterial and fungal microorganisms. UC-MSC was not HLA-matched between donor and recipient.
UC-MSC was initially suspended in 100 ml D5LR before intravenous infusion. Dose was calculated at 0.5 x106 cells/ kg body weight per infusion and given on days 1, 3, 5 and 7, with duration of 40 minutes (40 drops/min).23 Patients were closely monitored during the entire time of infusion.
We observed the patients during their entire stay in the hospital after UC-MSC infusion. Clinical symptoms, laboratory tests including measurements of inflammatory mediators and cytokines (IL6, IL10, IFN-γ, TNF-α), and radiological results were recorded for each patient. Cytokine levels were measured by ELISA with each sample run in triplicate.
Description of Cases
We treated 11 patients with COVID-19 pneumonia with UC-MSC. The Median age was 58 years (range 37- 89). There were 8 males and 3 females. Table 1 shows the baseline characteristics, treatments and clinical outcomes of patients with COVID-19 treated with UC-MSC therapy. Two patients did not complete the 4 doses of MSC. One expired after the second dose, while the other patient developed arrhythmia after the second dose. Although it was unclear what the etiology of the arrhythmia was, the medical team decided to discontinue the remaining doses of MSC for this patient. In terms of other treatments given, the proportion of treatment with oxygen was the highest (100%), followed by dexamethasone (10/11 patients) and remdesivir (9/11 patients). All patients also received different kinds of antimicrobials depending on the decision of their medical team.
| Patient | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Age | 57 | 49 | 37 | 70 | 64 | 70 | 52 | 58 | 58 | 64 | 89 |
| Sex | M | F | M | M | F | M | M | M | M | M | F |
| Co- morbidities | Dys- lipidemia, BPH | Myasthenia gravis, hyper- tension | Type 2 DM | Type 2 DM; Renal Cell Carcinoma (S/P Nephrec- tomy, Right) | Type 2 DM, Non Obstructing Coronary Artery Disease | Type 2 DM, Dys- lipidemia, History of Renal Cell CA (2005) | Essential Thrombo- cytosis Hyper- tension | Hyper- tension COPD | |||
| Treatments given | |||||||||||
| 1. Oxygen | High flow O2 | Mechanical ventilation 4th HD | High flow O2 | Mechanical ventilation 4th HD then BIPAP by 25th HD | O2 by nasal cannula | O2 by nasal cannula | O2 by nasal cannula | Mechanical ventilation 1st HD | O2 by nasal cannula | Mechanical ventilation 15th HD | Mechanical ventilation 1st HD |
| 2. Anti- virals: Remde-sivir | No | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes |
| 3. Anti- microbials | Meropenem | Ceftriaxone | Ceftriaxone | Ceftriaxone Azithro- mycin Piperacillin- tazobactam Meropenem Levofloxacin | Azithro- mycin | Meropenem | Azithro- mycin | Piperacillin- Tazobactam Meropenem Ceftazidime Avibactam Vancomycin Levofloxacin Ampicillin Polymixin B | Piperacillin- Tazobactam Meropenem Ceftazidime Avibactam Vancomycin Levofloxacin Ampicillin Polymixin B | Azithro- mycin Ceftriaxone Piperacillin- Tazobactam Levofloxain Meropenem Amikacin Fluconazole Cotri- moxazole | Piperacillin- Tazobactam Clindamycin Vancomycin Meropenem |
| Azithro- mycin Levofloxacin | Meropenem | Piperacillin- Tazobactam | Cefixime Clindamycin | Piperacillin- Tazobactam | Ceftriaxone | Ceftriaxone | Fluconazole Anidula- fungin Amikacin Tigecycline | ||||
| Aztreonam | Fluconazole | Piperacillin- tazobactam | |||||||||
| 4. Steroids dexame- thasone | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| 10 days | 5 days | 10 days | 10 days | 10 days | 10 days | 10 days | 10 days | 10 days | 10 days | ||
| 5. Hydroxy- chloroquine | Yes | No | No | No | No | No | No | No | No | No | No |
| 6. CRRT | No | No | No | No | No | No | No | Yes | Yes | No | Yes |
| 7. Others | IVIG | ||||||||||
| UC-MSC | |||||||||||
| Timing | 6th HD | 6th HD | 5th HD | 31st HD | 1st HD | 8th HD | 3rd HD | 4th HD | 2nd HD | 9th HD | 2nd HD |
| Doses given | 4 | 4 | 4 | 4 | 4 | 2 | 4 | 4 | 4 | 2 | 4 |
| Chest x-ray findings |
Pneumonia, bilateral, with interval increase
Pre-MSC New onset pneumonia, bilateral
Consider bilateral pneumonia
Pneumonia, bilateral Bilateral pneumonia bilateral infiltrates Bilateral pneumonia with consolida- tion; regressing in the right and unchanged in the left Post-MSC Unchanged bilateral pneumonia Regressing bilateral pneumonia Resolving pneumonia, bilateral PaO2/FiO2 Pre-MSC 94 195.4 121.25 125.58 289 105 427 234 125 97.5 227.2 Post-MSC 308.75 166.2 ND ND 465 ND ND 252 178.8 54 214 Inflammatory markers
- CRP Pre-MSC 66.73 336 270 85.94 1.47 94.95 41.37 251.7 66.5 381 57.21 Post-MSC 2.07 119.3 4.9 ND 0.47 ND 2.23 109.5 12.64 53.51 46.59
- Ferritin Pre-MSC 3770 864 3079 2310 3102 845 1090 1380 3970 1400 1350 Post-MSC 789 776 979 ND 773 ND 718 22000 1500 867 388
- D Dimer Pre-MSC 0.25 1.77 0.14 ND ND 2.37 0.19 0.71 0.46 0.77 2.51 Post-MSC 0.82 3.3 0.59 ND ND ND ND ND ND 1.62 ND
- LDH ND Pre-MSC 738 543 381 579 451 1482 210 468 598 299 481 Post-MSC 218 784 193 ND 335 ND 207 1379 396 249 312 Other Outcomes: Days from MSC infusion to:
Consider pulmonary edema with interval regression in the RIGHT and interval progression in the LEFT.
Consider interval develop- ment of bibasal pneumonia Consider pneumonia, left Consider bilateral pneumonia Bilateral pneumonia Pneumonia, bilateral, with decrease on the left and onset on the right No significant change in the bilateral pneumonia Pneumonia, bilateral, with interval regression Regressing bilateraL pneumonia Regressing pneumo- thorax, left Resolving pneumonia, bilateral
- 1. Off mech ventilation
- NA
- 34
- NA
- NA
- NA
- Expired
- NA
- Expired
- NA
- Still on mechanical ventilation
- Expired
- 2. Off oxygen
- 14
- On O2 until discharge
- 7
- 9
- 8
- Expired
- 6
- Expired
- 9
- NA
- Expired
- 3. Improved chest imaging
- 16
- 11
- 11
- 7
- 9
- Expired
- 5
- Expired
- 7
- NA
- 7
- 4. Negative
- COVID RT-
- PCR
- 27
- Positive until discharge
- 10
- ND
- 12
- Expired
- 10
- Expired
- ND
- ND
- Expired
- 5. Discharge
- 23
- 49
- 13
- 13
- 14
- Expired
- 8
- Expired
- 13
- Still admitted
- Expired
- Mortality
- No
- No
- No
- No
- No
- Yes
- No
- Yes
- No
- No
- Yes
- 12th HD
- 51st HD
- 23rd HD
Table 2: Patient Characteristics and Outcomes Measures.
Eight patients were not receiving invasive mechanical ventilation when US-MSC was administered; with 1 eventually needing mechanical ventilation and 1 expiring. Of the 3 patients who were already on mechanical ventilation before UC-MSC treatment, 2 eventually expired, while the third patient did not finish the complete course of treatment and is still admitted in the hospital.
Seven patients eventually improved in terms of need for supplemental oxygen and/or mechanical ventilation, clinical symptoms, resolution of pneumonia on imaging, and were discharged. C-reactive protein (CRP) and ferritin levels were the most consistent inflammatory markers measured for all the patients. In all patients, CRP decreased after UC- MSC treatment. Likewise for ferritin, except for 1 patient whose ferritin levels increased even more after UC-MSC.
This patient later expired. Three patients expired, 1 of whom expired before completing the full course of therapy.
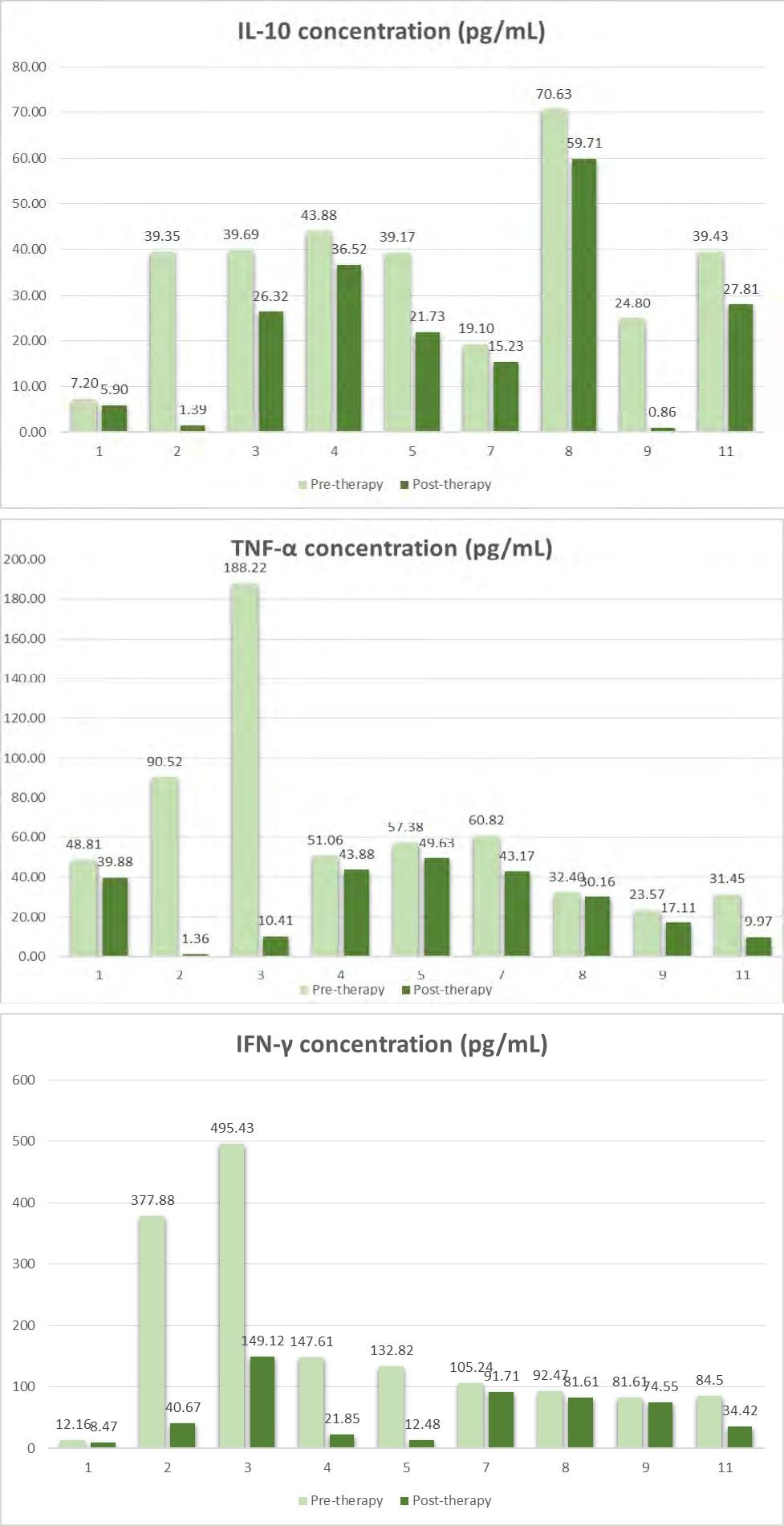
Figure 1 shows cytokine levels measured pre- and post-UC-MSC treatment. We were not able to do cytokine measurements on the 2 patients who did not complete the full course of therapy. The specific cytokine that were mainly elevated in each patient were either IL-6 (5 patients) or IFN-γ (4 patients). Regardless, all cytokine levels decreased for all patients after the 4 infusions of UC-MSC, albeit in different magnitudes.
All patients who received the UC-MSC treatment had no adverse reactions such as rash, allergic reaction, or febrile reaction during or after infusion.
Discussion
MSC has a positive impact in its use in cytokine release syndromes (CRS) from various etiologies because it has been shown to suppress excessive immune system activation by reducing the release of inflammatory factors mediated by immunomodulation [28, 29, 30, 31, 32]. As CRS plays a prominent role in the pathophysiology of COVID-19, using MSC to attenuate this syndrome makes it a promising candidate as a treatment of severe disease.
In this case series, we showed that although there were large variations in baseline cytokine pattern elevation all cytokines measured decreased rapidly after UC-MSC infusion. The extent of reduction of specific cytokines also differed, but in general, the higher the pre-MSC level of a specific cytokine, the greater the reduction of that cytokine; with reductions post-MSC treatment of up to > 90% compared to pre-MSC treatment levels in some patients. With this decrease in cytokine levels, there was likewise a decrease in other inflammatory markers, such as CRP and ferritin.
With the cytokine storm noted in patients with late- stage COVID-19 infection typically implicated as the primary cause of death [33] recognition of inflammatory markers or other cytokine-directed treatments obviously have important implications for treatment selection. Tocilizumab, a recombinant monoclonal antibody against the IL-6 receptor, which has been shown to mitigate the CRS associated with chimeric antigen receptor (CAR) T-cell therapy, has been used as a potential therapy for the cytokine storm associated with severe COVID-19 pneumonia [34, 35]. However, it is important to emphasize the difference in cytokine profiles of the patients. Our series clearly shows that cytokines other than IL-6, such as IFN-γ and TNF-α are also strongly associated with the inflammatory reaction and CRS in severe COVID-19 patients. Patients, in which case tocilizumab might not be expected to completely control the CRS in these patients. And so alternatives for dampening the overwhelming cytokine release are required, and the need for cytokine assays might be critical in personalized care and planning for future therapeutic options for COVID-19.
Similar to results from other centers, we also found that after UC-MSC infusions, there were no obvious side effects observed, indicating that the MSC were very well tolerated, even in severely ill patients.
As this is a case series, there are obvious limitations. We definitely cannot draw causal inferences because of inherent known and unknown confounders. The consequence of the decrease in cytokine levels to the clinical course of the patients is difficult to determine. The course of each patient was extremely varied. Although the majority of patients improved and were eventually discharged, the time for an individual patient to achieve these milestones were very different. We were unable to determine if there was an association on when and which cytokines decreased with the timing of clinical improvements for each patient. Even those patients who expired had marked decreases in the cytokine levels. We could also not observe a pattern in terms of effects on the timing on UC-MSC administration with noted decreases in cytokine levels, clinical improvement or mortality.
Our patients were a very heterogeneous group, especially in the other therapies that they received. Aside from MSC, these patients also received other off-label medications for COVID-19 pneumonia, such as antibiotics, remdesivir, dexamethasone, and hydroxychloroquine. Therefore, specific contributions of each therapy to the clinical improvement of the patients would be difficult to ascertain. However, unlike these other agents, MSC has been shown to have an immunomodulatory effect which could directly attenuate CRS. The cytokine data seen in our patients is therefore crucial.
Conclusion
Our experience showed that UC-MSC therapy down regulates the cytokine storm and may improve the clinical status in patients hospitalized with severe COVID-19 pneumonia without any infusion related reaction. Other current multiple center, prospective trials that are on- going will hopefully further elucidate the role of MSC in the treatment of COVID-19.
References
-
WHO (2020) WHO Coronavirus Disease (COVID-19) Dashboard.
-
Liang B, Chen J, Li T, Haiying Wu, Wenjie Yang, et al. (2020) Clinical remission of a critically ill COVID-19 patient treated by human umbilical cord mesenchymal stem cells: A case report. Medicine (Baltimore) 99(31): e21429.
-
Cheung CY, Poon LL, Ng IH, Winsie Luk, Sin-Fun Sia, et al. (2005) Cytokine responses in severe acute respiratory syndrome coronavirus-infected macrophages in vitro: possible relevance to pathogenesis. J Virol 79(12): 7819- 7826.
-
Yang K, Sheng Y, Huang C, Yang Jin, Nian Xiong, et al. (2020) Clinical characteristics, outcomes, and risk factors for mortality in patients with cancer and COVID-19 in Hubei, China: a multicentre, retrospective, cohort study. Lancet Oncol 21(7): 904-913.
-
Huang C, Wang Y, Li X, Lili Ren, Jianping Zhao, et al. (2020) Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 395(10223): 497-506.
-
Wang D, Hu B, Hu C, Fangfang Zhu, Xing Liu, et al. (2020) Clinical Characteristics of 138 Hospitalized Patients With 2019 Novel Coronavirus-Infected Pneumonia in Wuhan, China. JAMA 323(11):1061-1069.
-
Chousterman BG, Swirski FK, Weber G (2017) Cytokine storm and sepsis disease pathogenesis. Semin Immunopathol 39(5): 517-528.
-
Shimabukuro-Vornhagen A, Gödel P, Subklewe M, Hans Joachim Stemmler, Hans Anton Schlößer, et al. (2018) Cytokine release syndrome. J Immunother Cancer 6(1): 56.
-
Xu X, Han M, Li T, Wei Sun, Dongsheng Wang, et al. (2020) Effective treatment of severe COVID-19 patients with tocilizumab. Proc Natl Acad Sci U S A 117(20): 10970- 10975.
-
Han Y, Li X, Zhang Y, Chang F, Ding J, et al. (2019) Mesenchymal Stem Cells for Regenerative Medicine. Cells. 08 8(8): 886.
-
Le Blanc K, Davies LC (2018) MSCs-cells with many sides. Cytotherapy 20(3): 273-278.
-
Gao F, Chiu SM, Motan DA, Zhang Z, Chen L, et al. (2016) Mesenchymal stem cells and immunomodulation: current status and future prospects. Cell Death Dis 7(1): e2062.
-
de Castro LL, Lopes-Pacheco M, Weiss DJ, Cruz FF, Rocco PRM, et al. (2019) Current understanding of the immunosuppressive properties of mesenchymal stromal cells. J Mol Med (Berl) 97(5): 605-618.
-
Saldaña L, Bensiamar F, Vallés G, Mancebo FJ, García- Rey E, et al. (2019) Immunoregulatory potential of mesenchymal stem cells following activation by macrophage-derived soluble factors. Stem Cell Res Ther 10(1): 58.
-
Uccelli A, de Rosbo NK (2015) The immunomodulatory function of mesenchymal stem cells: mode of action and pathways. Ann N Y Acad Sci 1351(1): 114-126.
-
Ben-Mordechai T, Palevski D, Glucksam-Galnoy Y, Elron- Gross I, Margalit R, et al. (2015) Targeting macrophage subsets for infarct repair. J Cardiovasc Pharmacol Ther 20(1): 36-51.
-
Squillaro T, Peluso G, Galderisi U (2016) Clinical Trials With Mesenchymal Stem Cells: An Update. Cell Transplant 25(5): 829-848.
-
Fujita Y, Kadota T, Araya J, Ochiya T, Kuwano K, et al. (2018) Clinical Application of Mesenchymal Stem Cell- Derived Extracellular Vesicle-Based Therapeutics for Inflammatory Lung Diseases. J Clin Med 7(10): 355.
-
Horie S, McNicholas B, Rezoagli E, Tài Pham, Ger Curley, et al. (2020) Emerging pharmacological therapies for ARDS: COVID-19 and beyond. Intensive Care Med 46(12): 2265-2283.
-
Lee JW, Fang X, Krasnodembskaya A, Howard JP, Matthay MA, et al. (2011) Concise review: Mesenchymal stem cells for acute lung injury: role of paracrine soluble factors. Stem Cells 29(6): 913-919.
-
Walter J, Ware LB, Matthay MA (2014) Mesenchymal stem cells: mechanisms of potential therapeutic benefit in ARDS and sepsis. Lancet Respir Med 2(12): 1016- 1026.
-
Wilson JG, Liu KD, Zhuo H, Lizette Caballero, Melanie McMillan, et al. (2015) Mesenchymal stem (stromal) cells for treatment of ARDS: a phase 1 clinical trial. Lancet Respir Med 3(1): 24-32.
-
Leng Z, Zhu R, Hou W, Yingmei Feng, Yanlei Yang, et al. (2020) Transplantation of ACE2- Mesenchymal Stem Cells Improves the Outcome of Patients with COVID-19 Pneumonia. Aging Dis 11(2): 216-228.
-
Released by National Health Commission & National Administration of Traditional Chinese Medicine on March 3 (2020) Diagnosis and Treatment Protocol for Novel Coronavirus Pneumonia (Trial Version 7). Chin Med J (Engl) 133(9): 1087-1095.
-
Lee DW, Santomasso BD, Locke FL, Armin Ghobadi, Cameron J Turtle, et al. (2019) ASTCT Consensus Grading for Cytokine Release Syndrome and Neurologic Toxicity Associated with Immune Effector Cells. Biol Blood Marrow Transplant 25(4): 625-638.
-
Dominici M, Le Blanc K, Mueller I, I Slaper-Cortenbach, FC Marini, DS Krause, et al. (2006) Minimal criteria for defining multipotent mesenchymal stromal cells. The International Society for Cellular Therapy position statement. Cytotherapy 8(4): 315-317.
-
Alma Reyes-Calavera, Vasiliki E Kalodimou (2020) A proposed protocol of derived mesenchymal stem cells for the treatment of COVID-19. Cell & Gene Therapy Insights 6(6): 807-811.
-
Galipeau J, Sensébé L (2018) Mesenchymal Stromal Cells: Clinical Challenges and Therapeutic Opportunities. Cell Stem Cell 22(6): 824-833.
-
Bernardo ME, Fibbe WE (2013) Mesenchymal stromal cells: sensors and switchers of inflammation. Cell Stem Cell 13(4): 392-402.
-
Harrell CR, Sadikot R, Pascual J, Crissy Fellabaum, Marina Gazdic Jankovic, et al. (2019) Mesenchymal Stem Cell- Based Therapy of Inflammatory Lung Diseases: Current Understanding and Future Perspectives. Stem Cells Int 2019: 4236973.
-
Yan X, Fu X, Jia Y, Xiaona Ma, Jin Tao, et al. (2019) Nrf2/Keap1/ARE Signaling Mediated an Antioxidative Protection of Human Placental Mesenchymal Stem Cells of Fetal Origin in Alveolar Epithelial Cells. Oxid Med Cell Longev 2019: 2654910.
-
Sinclair KA, Yerkovich ST, Chen T, McQualter JL, Hopkins PMA, et al. (2016) Mesenchymal Stromal Cells are Readily Recoverable from Lung Tissue, but not the Alveolar Space, in Healthy Humans. Stem Cells 34(10): 2548-2558.
-
Fu B, Xu X, Wei H (2020) Why tocilizumab could be an effective treatment for severe COVID-19? J Transl Med 18(1): 164.
-
Biran N, Andrew IP, Ahn J, Ronaldo C Go, Shuqi Wang, et al. (2020) Tocilizumab among patients with COVID-19 in the intensive care unit: a multicentre observational study. Lancet Rheumatol 2(10): e603-e612.
-
Campochiaro C, Della-Torre E, Cavalli G, Giacomo De Luca, Marco Ripa, et al. (2020) Efficacy and safety of tocilizumab in severe COVID-19 patients: a single-centre retrospective cohort study. Eur J Intern Med 76: 43-49.
- Research Progress of Induced Pluripotent Stem Cells and Their Clinical Application Prospects
- Nishan Al-Kamal is the Starting Point of A Feminist Scientist
- Current Concepts and Future Perspectives of Stem Cell Therapy in Peripheral Arterial Disease
- Stem Cell and Oxidative Stress-Inflammation Cycle
- Adipose Derived Mesenchymal Stem Cells Origin, Characteristics and Promises
- Mitochondria Targeted Antioxidants can Improve In Vitro Embryo Production in Buffalo