Progressive Multifocal Leukoencephalopathy in AIDS Patients: A Report on 15 Cases
Progressive Multifocal Leukoencephalopathy (PML) is a degenerative disease of the central nervous system (CNS) caused by a polyoma virus called JC polyoma virus (JCPyV). It affects patients with some diseases like lymphoproliferative diseases and patients with advanced AIDS usually with a CD4 count of less than 100 cells/L and carries a poor prognosis. Its clinical and radiological features are suggestive but could be similar to other diseases like toxoplasmosis and tuberculosis that can affect the CNS in AIDS patients. Here we report on 15 cases of PML, attended and managed in Tripoli University Hospital in Tripoli, Libya. All of the patients were in advanced stages of HIV infection, and were not using medications at presentation. All the patients except one died within a period of 2 days- 2 months of presentation possibly due to associated opportunistic infections (OI). PML has not been reported in the Libyan medical literature and here we report its clinical and radiological features and the prognosis of its course.
Introduction
Progressive Multifocal Leukoencephalopathy (PML) is a severe demyelinating disease of the central nervous system (CNS) caused by a polyoma virus called JCyV virus after the initials of the first patient, from which this simple DNA virus was first isolated in 1971 [1]. The disease can occur as an activation of a latent infection in patients with lymphoproliferative disorders, sarcoidosis, immunosuppressive treatment, pregnancy, diabetes, after treatment with monoclonal antibodies like natalizumab and in old age [2].
Among AIDS patients it affects around 4% of them, usually with CD4 cell count less than 50/mm3 [3, 4] or in some of these cases, it can present as an immune reconstitution syndrome (IRIS) after starting effective antiretroviral treatment (ART) [5].
Epidemiologically, 50% of normal children at 6 years of age and 80% of the general population have a serum positive antibody test against the virus without having any clinical manifestations, with the virus staying dormant in the lymphoid tissue, kidneys and bone marrow. Its mode of transmission is not well known but its widespread distribution suggests the inhalation route as the probable route of transmission. With immunosuppression the virus may become active and cause disease affecting usually the CNS [6].
Clinically, in AIDS patients, PML presents very insidiously with patients presenting after weeks to months of CNS
symptoms like loss of vision, clumsiness, difficulty in walking, loss of coordination, facial drooping, seizures, muscle weakness, personality changes and speech trouble [7].
In Libya, only one report was found about this disease [8] and since such cases can be seen in the medical ward especially in countries where ART is not always available for AIDS patients, we present these 15 cases to highlight the importance of this disease in the differential diagnosis of CNS problems.
Objective
To describe the clinical course/outcome, laboratory and radiological features of PML in 15 Libyan patients with AIDS.
Patients and Methods
The study was a retrospective study where we examined the files of 15 patients attended at the Infectious Disease Department (IDD) of Tripoli University Hospital (TUH) (formerly known as Tripoli Medical Center) between 2004 and 2008. The personal data of the patients (age, sex) together with some clinical data were noted. The available CD4 count and the PCR of HIV results, were registered together with the results of the CT-scan and/or MRI. Simple statistical analysis was used to verify frequencies.
Results
We included 15 patients with PML. All of them, except one, were males. Intravenous drug abuse was the risk factor for HIV in all of them except in the woman included in this study who got infection from her husband. All of them denied homosexual behaviour. Their ages ranged between 16 to 45 years (mean: 34,7y). Most of them (77%) were in their 4th decade of age. The mean duration of symptoms was 3.5 months (range: one week- 12 months). The disease was of slow onset in all of the cases taking few weeks to 3 months.
Cognitive, motor and visual symptoms were found in 60%, 46% and 27% of the patients, respectively. Expressive dysphasia was common affecting 30% of them. Focal and/ or generalized fits were observed in 26% of the patients. Cerebellar symptoms/signs were found in four patients (27%), in two of them they were the only neurological symptoms.
Other opportunistic infections like toxoplasma encephalitis, pulmonary tuberculosis and oral candidiasis were found in one, two, and seven patients, respectively.
All the patients had severe lymphopenia. In patients with available results, the CD4 count was below 200 cells/µL in all of them except one who has a CD4 count of 205. It was less than 100 cells/µL in 9 of them (75%). In those with available PCR the HIV viral load ranged from 37.000-1.700.000 c/mm3.
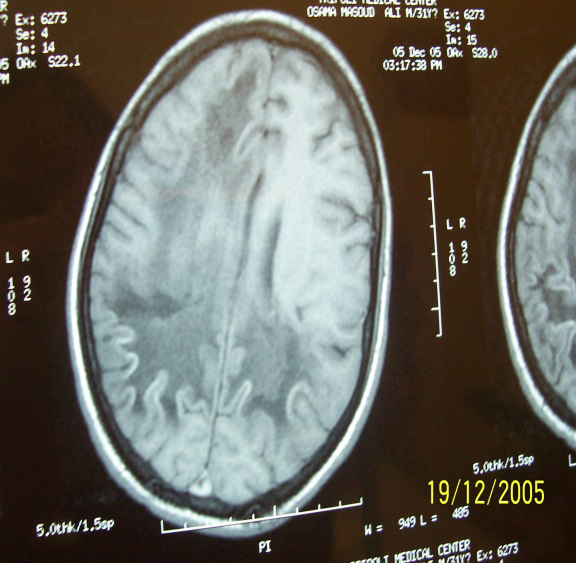
All the patients had typical MRI findings of PML (hypodense white matter in T1 weighted and hyperdense areas in T2 weighted MRI without a mass effect). In the CT scan the PML lesions appeared as hypodense confluent lesions without mass effect affecting the white matter only. The lesions affected the cerebral hemispheres only in 11 patients being bilateral in 4 patients. They affected the cerebral and cerebellar hemispheres in 4 patients (Figures 1 & 2). Isolated cerebellar involvement was found in 2 patients (Figure 3).
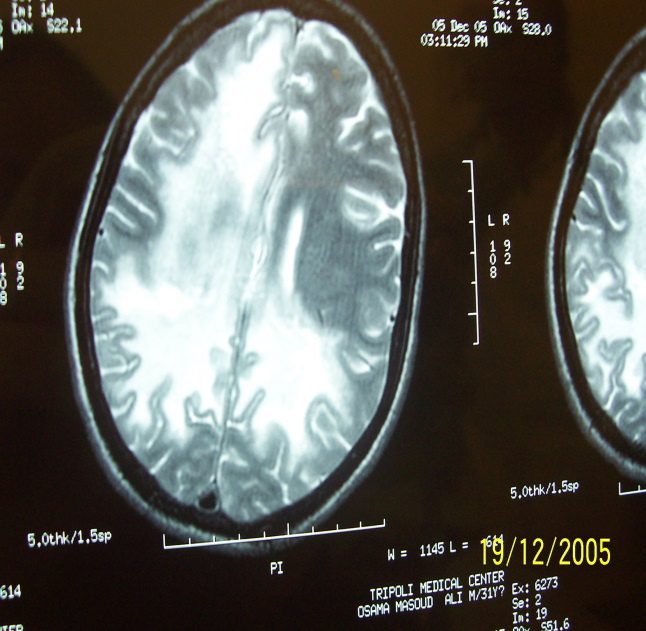
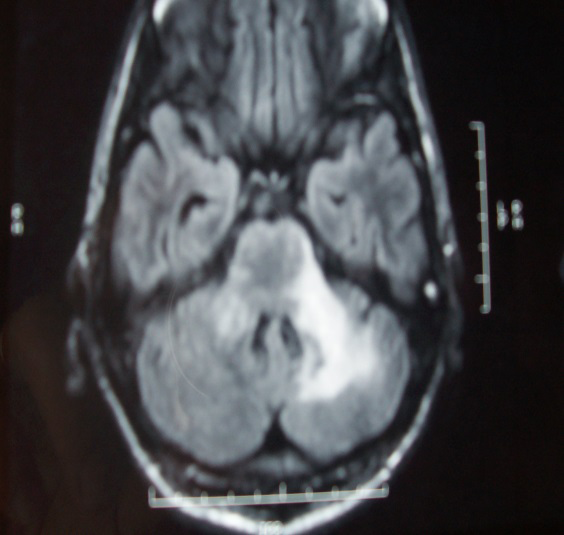
In spite of the initiation of the highly active antiretroviral therapy (HAART) all the patients except one died within 2 days to 2 months of their diagnosis. The only one surviving patient had isolated cerebellar involvement and this could explain his better prognosis.
Discussion
The JCPyV virus infects the oligodendrocytes that produce the myelin nerve sheaths which cover the nerves, leading to destruction of the white matter of the brain with possible consequent atrophy and shrinkage of the brain without affecting the gray matter [9]. The disease affects patients with low CD4 count usually less than 100 cells/mm3 [2] although it can affect also patients with higher CD4 count, a fact that was shown here in one of our cases.
The mean survival time of the untreated patients with PML is 2 months but it is around 20 months with HAART [6]. In our cases, one patient survived for 2 years, most likely because his PML was restricted to the cerebellum and did not involve more vital structures, the other patients died due to the more extensive cerebral disease and possibly due to more serious associated opportunistic diseases like tuberculosis.
The diagnosis of PML is usually made by a suggestive clinical picture and compatible CT/MRI findings, but a definitive diagnosis is made with brain biopsy. Cognitive, motor and visual problems are common but fever, headache and sensory problems are rare being more common in patients with cerebral toxoplasmosis. These findings were clearly found in our cases and have been reported by others [9, 10]. By CT-scan the lesions show decreased attenuation of the affected white matter which appears as intense areas on proton-density and T2-weighted MRI. Subtle lesions are common especially with CT-scan that is less sensitive than the MRI to diagnose such lesions. Mass effect is usually absent and the lesions do not show uptake of contrast. These features were clear and suggestive in our patients (Figures 1-3). In the late stages ipsilateral atrophic changes could be seen [10].
Although the MRI findings are quite typical for PML, many times they are not enough to differentiate it from HIV-associated leukoencephalopathy or HHV-6 infection. So definitive diagnosis relies on a brain biopsy [11, 12].
The differential diagnosis of PML also includes cerebral toxoplasmosis (CT), which has a more rapid clinical course, CNS lymphoma, tuberculoma, and cryptococcoma but all these lesions produce mass effect and/or show contrast uptake [13].
CSF examination is not helpful but a pleocytosis of more than 100 cells excludes PML. Looking for the virus in the CSF by the PCR technique has a sensitivity of 80% and specificity over 90% but is not always positive as it is in the urine and plasma [14, 15].
The treatment of PML relies mainly on the early use of HAART which looks to be effective in changing the course of the disease in some cases [16, 17] but may not prevent its development since many cases developed PML in spite of having undetectable viral load [18]. Worsening of the symptoms after starting HAART, can happen also and could be related to the JCPyV-related immune reconstitution syndrome (IRIS) [19, 20, 21].
Antiviral treatment options like foscarnet and cytarabine and immune modulating agents like immune stimulants, steroids, interferon were found to be in-effective in the treatment of PML [22, 23, 24].
Cidofovir and camptothecin were tested in some case studies with little or no significant efficacy and are not recommended and there is no effective secondary prophylaxis against PML for patients with low CD4 count [25, 26].
More recently, drugs targeting JCPyV infection and spread including inhibitors of viral attachment, viral entry, viral signaling, viral trafficking, viral uncoating, all proved ineffective [27].
PML was a fairly common OI among our patients with AIDS due to the non-availability of ART, and nowadays we see much less cases because ART is more available, better adherence of the patients to the treatment and due to less stigma against these patients [28].
Conclusions
PML is a rare but serious disease in AIDS patients and it should be included in the differential diagnosis during evaluation of any AIDS patient presenting with CNS manifestations in any patient with CNS manifestations not on ART or being started on these medications. Because of the non-availability of any effective treatment and hence its poor prognosis, HIV-infected patients should be started on ART as early as possible to avoid severe immunosuppression and its consequences of severe OIs like PML.
Acknowledgement
Special thanks to our staff in the IDD, TUC, TUH for their dedication and care for these patients. The study was approved by the committee of medical ethics of the hospital.
Funding
No funding of any type was received.
References
-
Major EO, Amemiya K, Tornatore CS, Houff SA, Berger JR, et al. (1992) Pathogenesis and molecular biology of progressive multifocal leukoencephalopathy, the JC virus-induced demyelinating disease of the human brain. Clin Microbi Rev 5(1): 49-73.
-
Kleinschmidt-DeMasters BK, Tyler KL (2005) Progressive multifocal leukoencephalopathy complicating treatment with natalizumab and interferon beta-1a for multiple sclerosis. N Engl J Med 353(4): 369-374.
-
Berger JR, Kaszovita, B, Post JD, Dickinson G (1987) Progressive multifocal Leukoencephalopathy associated with human immunodeficiency virus infection. Ann Inter Med 107: 78-87.
-
Gildenberg PL, Gathe JC, Kim JH (2000) Stereotactic biopsy of cerebral lesions in AIDS. Clin Infect Dis 30(3): 491-499.
-
Rtan K, Roda R, Ostrow L, McArthur J, Nath A, et al. (2009) PML-IRIS in patients with HIV infection: clinical manifestations and treatment with steroids. Neurology 72(17): 1458-1464.
-
Taguchi F, Kajioka J, Miyamura T (1982) Prevlance rate and age of acquisition of antibodies against JC and BK virus in human sera. Microbio Immunol 26(11): 1057- 1064.
-
Saji AM, Gupta V (2023) Progressive multifocal leukoencephalopathy. StatPearls Publishing, National Librarary of Medicine.
-
Rayes AA, Khalil I (2008) Progressive multifocal leukoencephalopathy in AIDS patients: a report on 15 cases. 44th Congress of the Brazilian Society of Tropical Medicine, Porto Alegre.
-
Shah KV (1990) Polyomaviruses. In: Chanock RM, et al. (Eds.), Virology. 2nd(Edn.), Raven Press, New York, pp: 1609-1623.
-
Mark AS, Atlas SW (1989) Progressive multifocal leukoencephalopathy in patients with AIDS: appearance on MR images. Radiology 173(2): 517-520.
-
Caserta MT (2004) Human Herpesvirus 6 Infection of the Central Nervous System. Curr Infect Dis Rep 6: 316- 321.
-
Langford TD, Letendre SL, Marcotte TD, Ellis RJ, Grant I, et al. (2002) Severe, demyelinating leukoencephalopathy in AIDS patients on antiretroviral therapy. AIDS 16(7): 1019-1029.
-
Elkin CM, Leon E, Grenell SL, Leeds NE (1985) Intracranial lesions in the acquired immune deficiency syndrome: radiological CT features. JAMA 253(3): 393-396.
-
Hou J, Major EO (2000) Progressive multifocal leukoencephalopathy: JC virus induced demyelination in the immune compromised host. Journal of Neurovirology 6(2): 98-100.
-
Whiley DM, Mackay IM, Sloots TP (2001) Detection and differentiation of human polyomaviruses JC and BK by LightCycler PCR. Journal of Clinical Microbiology 39(12): 4357-4361.
-
Antinori A, Ammassari A, Giancola ML, Cingolani A, Grisetti S, et al. (2001) Epidemiology and prognosis of AIDS- associated progressive multifocal leukoencephalopathy in the HAART era. Journal of Neurovirology 7(4): 323- 328.
-
Albrecht H, Hoffmann C, Degen O, Stoehr A, Plettenberg A, et al. (1998) Highly active antiretroviral therapy significantly improves the prognosis of patients with HIV- associated progressive multifocal leukoencephalopathy. AIDS 12(10): 1149-1154.
-
Clifford DB, Yiannoutsos C, Glicksman M, Simpson DM, Singer EJ, et al. (1999) HAART improves prognosis of HIV- associated progressive multifocal leukoencephalopathy. Neurology 52(3): 623-625.
-
Martinez AC, Lopez GA, Garcia IG (2000) Successful resolution of progressive multifocal leukoencephalopathy after combination therapy with cidofovir and cytosine arabinoside. Clinical Infectious Diseases 30(1): 234.
-
Pasquier RA, Koralnik IJ (2003) Inflammatory reaction in progressive multifocal leukoencephalopathy: harmful or beneficial. J Neurovirol 9(1): 25-31.
-
Hoffmann C, Horst HA, Albrecht H, Schlote W (2003) Progressive multifocal leucoencephalopathy with unusual inflammatory response during antiretroviral treatment. J Neurol Neurosurg Psychiatry 74(8): 1142- 1144.
-
Hall CD, Dafni U, Simpson D, Clifford D, Wetherill PE, et al. (1998) Failure of cytarabine in Progressive Multifocal Leukoencephalopathy associated with Human Immunodeficiency Virus infection. New England Journal of Medicine 338(19): 1345-1351.
-
Berenguer J, Miralles P, Arrizabalaga J, Ribera E, Dronda F, et al. (2003) Clinical course and prognostic factors of progressive multifocal leukoencephalopathy in patients treated with highly active antiretroviral therapy. Clinical Infectious Diseases 36(8): 1047-1052.
-
Geschwind MD, Skolasky RI, Royal WS, McArthur JC (2001) The relative contributions of HAART and alpha-interferon for therapy of progressive multifocal leukoencephalopathy in AIDS. Journal of Neurovirology 7(4): 353-357.
-
Royal W, Dupont B, McGuire D, Chang L, Goodkin K, et al. (2003) Topotecan in the treatment of acquired immunodeficiency syndrome-related progressive multifocal leukoencephalopathy. J Neurovirol 9(3): 411- 419.
-
Wyen C, Hoffmann C, Schmeier N, Wöhrmann A, Qurishi N, et al. (2004) Progressive Multifocal Leukencephalopathy in Patients on Highly Active Antiretroviral Therapy: Survival and Risk Factors of Death. J AIDS 37(2): 1263- 1268.
-
Kaiserman J, O’Hara BA, Haley SA, Atwood WJ (2023) An Elusive Target: Inhibitors of JC Polyomavirus Infection and Their Development as Therapeutics for the Treatment of Progressive Multifocal Leukoencephalopathy. Int J Mol Sci 24(10): 8580.
-
Asensi V (1999) Prolonged survival after HAART in AIDS- associated progressive multifocal leukoencephalopathy (PML). 39th Interscience Conference on Antimicrobial Agents and Chemotherapy, San Francisco, USA.
- Epidemiological and Clinical Aspects of Intestinal Parasitoses Among Students in the City of Bocaranga, Central African Republic
- Artificial Intelligence Empowers Global Infectious Disease Prevention and Control: Opportunities and Challenges
- Factors that Affect the Incidence of Babesia and Blood Donor Testing in Select States: A Regression Analysis
- Neuro-TB: The Battle between Tuberculosis and the Nervous System
- The Biological and Health Implications of Cat Fleas (Ctenocephalides felis): Assessing Zoonotic Risks and Hygiene Strategies
- Biostatistical Analysis of Medicinal Plants for Treating Schizophrenia