Vortex and Crater-Squamous Cell Carcinoma Lung
Editorial
Squamous cell carcinoma lung manifests as a malignant tumefaction emerging from epithelial cells demonstrating squamous differentiation. Squamous epithelial differentiation within the neoplasm is represented by morphological features as variable proportion of intercellular bridges, focal intracellular or extracellular keratinization and configuration of keratin pearls, cogent immunohistochemistry may be advantageously applied for diagnostic confirmation. Squamous cell carcinoma lung may appear as keratinizing or non-keratinizing neoplasm. Additionally, diverse subtypes as solid, cystic, papillary, pseudo-glandular, alveolar- filling or sarcomatoid with spindle shaped cells may be observed. In contrast, poorly differentiated neoplasms appear devoid of cogent morphological features indicative of squamous differentiation. Precise immunohistochemistry is necessitated to segregate the neoplasm from diverse non- small cell pulmonary neoplasms. Besides, immune reactivity to p40 appears beneficial for appropriate categorization. Primary and metastatic pulmonary neoplasms may demonstrate concurrent morphological features and immunohistochemistry. Thus, ascertainment of emergence of primary site of squamous cell carcinoma may be challenging. The terminology of epidermoid carcinoma lung appears obsolete. History of cigarette smoking is intensely concurrent with occurrence of squamous cell carcinoma and is encountered in ~80% males and ~90% of incriminated females [1, 2].
Neoplasm commonly arises within subjects ≥ 50 years. Majority (~ 85%) of primary pulmonary carcinomas emerge as non-small cell carcinomas. Squamous cell carcinoma lung configures ~30% of non-small cell pulmonary carcinomas [1, 2].
Squamous epithelial cells layering the respiratory tract may metamorphose due to exposure to carcinogens which are frequently accumulated due to cigarette smoking. Besides, occupational exposure to heavy metals may engender the neoplasm. Notwithstanding, squamous cell carcinoma lung may manifest with extra-pulmonary variants [1, 2].
Squamous cell carcinoma lung expounds genomic variants of EGFR and ALK, a feature which may be concurrent in neoplasms arising within young or non smoking subjects [1, 2]. Squamous cell carcinoma lung frequently configures as a centric neoplasm although no site of pulmonary parenchyma or bronchus is exempt from disease emergence [1, 2]. Metastasis is preponderantly confined to mediastinal lymph nodes. Distant metastasis is frequently exemplified. Haematogenous neoplastic dissemination into distant organs may ensue wherein bone or hepatic parenchyma is commonly incriminated [1, 2].
Squamous cell carcinoma lung is associated with several nonspecific pulmonary symptoms as cough, chest pain, dyspnoea, haemoptysis, wheezing or repetitive pulmonary infections. Besides, loss of appetite, loss of weight and fatigue may ensue. Compression of recurrent laryngeal nerve may be associated with hoarseness [1, 2].
Cytological examination exhibits atypical squamous epithelial cells. Well differentiated neoplasms delineate focal extracellular or intracellular keratinization. Lesions of advanced grade appear reminiscent of pulmonary adenocarcinoma. Neoplastic cells may demonstrate cytoplasmic stretching, a feature denominated as ‘tadpole cells’ Cogent immunohistochemistry may be beneficially adopted to segregate squamous cell carcinoma from pulmonary adenocarcinoma [3, 4]. Grossly, squamous cell carcinoma lung represents as a cavity confined within the pulmonary parenchyma. Tumefaction represents as a grey/ white mass. Cut surface is smooth with frequently discerned foci of haemorrhage and necrosis. Centric tumefaction infiltrating the bronchus is commonly enunciated, in contrast to peripheral location of the neoplasm [3, 4].
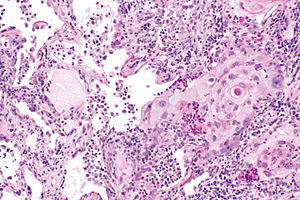
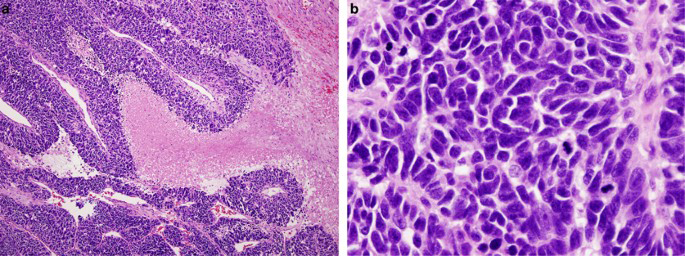
Upon microscopy, neoplastic cells demonstrate features such as focal keratinization with configuration of keratin pearls. Intercellular bridges adhering adjacent polygonal squamous epithelial cells appear variable. Tumour cells are incorporated with abundant eosinophilic cytoplasm and enlarged, vesicular nuclei with prominent nucleoli and elevated nucleocytoplasmic ratio. Foci of abundant acute and chronic inflammatory cell exudate and tumour necrosis are exemplified [5, 6]. Squamous cell carcinoma lung is graded contingent to perceived proportionate differentiation. Cellular and nuclear atypia appears concurrent to grade of neoplasm [5, 6].
Poorly differentiated squamous cell carcinoma lung exemplifies significant cellular and nuclear atypia. Mitotic figures are abundant. Precise immunohistochemistry is necessitated to differentiate the neoplasm from various poorly differentiated neoplastic lesions [5, 6]. Upon ultrastructural examination, tumour cells are incorporated with abundant tonofilaments, complex desmosomes or basal lamina [5, 6] (Figures 1 & 2).
| Immune marker | Squamous cell carcinoma | Adenocarcinoma |
|---|---|---|
| p40 | + | +/- |
| p63 | + | +/- |
| CK5/6 | + | - |
| CK7 | - | + |
| Chromogranin A | - | - |
| Synaptophysin | - | - |
| TTF-1 | - | + |
Table 1: Immunohistochemistry of non-small cell lung carcinoma [4].
Squamous cell carcinoma lung is intensely and diffusely immune reactive to p40, p63, CK7, high molecular weight keratin, pan-cytokeratin, CK5/6 or PDL1(7,8). Tumour cells appear immune non reactive to various neuroendocrine markers, thyroid transcription factor-1(TTF-1) or CK20. Squamous cell carcinoma lung requires segregation from neoplasms such as adenocarcinoma lung with a predominant solid pattern, high grade small cell carcinoma, malignant melanoma, adenosquamous carcinoma, NUT pulmonary carcinoma, squamous cell metaplasia, large cell neuroendocrine carcinoma lung, mucoepidermoid carcinoma, lymphoepithelial carcinoma, large cell carcinoma, pleomorphic pulmonary carcinoma or SMARCA4 deficient undifferentiated tumour [7, 8]. Squamous cell carcinoma lung can be appropriately discerned with cytological examination or histological examination of surgical tissue samples. Poorly differentiated areas exhibit lack of keratinization and may be analysed with precise immunohistochemistry. Biochemical assay exemplifies humoral hypercalcemia induced due to malignant metamorphosis, representing as a feature arising subsequent to paraneoplastic syndrome. Aforesaid anomaly appears within 10% instances and is associated with inferior prognostic outcomes [7, 8]. Computerized tomography (CT) is recommended in order to appropriately evaluate carcinoma lung. Squamous cell carcinoma lung manifests as a nonspecific tumour mass with an irregular perimeter. Centric cavitation is commonly encountered. Pulmonary neoplasms frequently confined to centric zones delineate airway obstruction and may be associated with pneumonitis or pulmonary collapse. Distinction of squamous cell carcinoma from diverse pulmonary carcinomas or benign lesions may be challenging upon radiography as radiological features appear identical [7, 8]. Surgical extermination emerges as a primary, optimal therapeutic modality for alleviating squamous cell carcinoma lung. Nevertheless, surgical manoeuvers as wedge resection, lobectomy or pneumonectomy may be beneficially adopted as efficacious therapeutic strategies. Systemic chemotherapy or PDL1 immunotherapy and radiation therapy may be alternatively employed [7, 8]. Tumour stage upon initial neoplastic determination is an appropriate indicator of prognostic outcomes [7, 8].
References
-
Sabbula BR, Gasalberti DP, Anjum F (2023) Squamous Cell Lung Cancer. Stat Pearls International Treasure Island, Florida, USA.
-
Javed N, Lee S, Bojja S, Tiwari U, Khaja M (2023) Liquefied Lung Cancer: An Uncommon Form of Squamous Cell Carcinoma of the Lung. Cureus 15(7): e41848.
-
Vicidomini G (2023) Current Challenges and Future Advances in Lung Cancer: Genetics, Instrumental Diagnosis and Treatment. Cancers (Basel) 15(14): 3710.
-
Grodzka A, Knopik-Skrocka A, Kowalska K, Kurzawa P, Krzyzaniak, et al. (2023) Molecular alterations of driver genes in non-small cell lung cancer: from diagnostics to targeted therapy. EXCLI J 22: 415-432.
-
Wang D, Ye W, Chen D, Shi Q, Ma D (2023) Transformation of Lung Squamous Cell Carcinoma to Small Cell Lung Cancer After Immunotherapy Resistance: A Case Report. Cancer Manag Res 15: 803-808.
-
De Toro M, Pangua C, Serrano-Montero G, Lara MA, Rogado J (2023) New potential targeted strategies in small cell lung cancer. Transl Lung Cancer Res 12(4): 661-664.
-
De Jong D, Das JP, Ma H, Valiplackal, Prendergast C, at al. (2023) Novel Targets, Novel Treatments: The Changing Landscape of Non-Small Cell Lung Cancer. Cancers (Basel) 15(10): 2855.
-
Xiao Y, Liu P, Wei J, Zhang X, Guo J, et al. (2023) Recent progress in targeted therapy for non-small cell lung cancer. Front Pharmacol 14: 1125547.
- Ramsay Hunt Syndrome Presenting as Gait Imbalance without Facial Paralysis: A Case Report
- Unveiling Hidden Culprits: An Observational Study of Upper Gastrointestinal Endoscopy Findings in Symptomatic Cholelithiasis Patients
- Assessing Health Care Providers’ Proficiency in International Patient Safety Goals: A Study to Assess the Knowledge &Practice on Patient Safety in a Tertiary Care Teaching Hospital in Gujarat
- Challenges in Diagnosing Child Language Disorders
- Stunting Service Management Model in the South-Central Timor Region, East Nusa Tenggara, Indonesia
- Acute Small Bowel Obstruction Presenting as Gangrenous Jejunal Loop Secondary to Intestinal Endometriosis – A Rare Case Report