Clinical Case Reports 1983 - 87
In this article five case reports were reviewed and include chylopericardium that developed after performing a Blalock-Taussig shunt, successful surgical repair of syndrome absent pulmonary valve with pulmonary arterioplasty but without replacement of the pulmonary valve, simultaneous occurrence of transient eosinophilic pulmonary infiltration secondary to intestinal schistosomiasis and mitral stenosis and their effective management, description of a rare variant of tricuspid atresia with atrioventricular canal, and successful drug therapy of congestive cardiomyopathy that developed due to chronic tachycardia. Discussion of uniqueness of these findings and management options were reviewed.
Introduction
During the academic practice of the author during a five-decade period, a number of clinical cases have been encountered and reported. The cases documented from 1970 to 1984 were reviewed previously [1, 2, 3, 4]. This report covers the period between 1983 and 1987.
Chylopericardium Following Blalock-Taussig Anastomosis
Introduction: Chylopericardium following Blalock-Taussig (BT) shunt is extremely rare, especially in those patients in whom the pericardial cavity is not opened during surgery. The purpose of our report was to document a case of chylopericardium which developed after a BT shunt, to point out its rarity, and to discuss management strategies [5].
fluid and therefore, pericardial window via left lateral thoracotomy was performed and drainage tubes were placed. The infant was started on medium-chain triglyceride (MCT) formula (Portagen, Mead Johnson, Evansville, IN). Within a few days, the pericardial drainage ceased and the chest tubes were removed. The infant was continued on MCT formula. Revaluation in the outpatient department a month later did not show evidence for recurrence of pericardial effusion and there was a functioning BT shunt with satisfactory O2 saturations. Discussion: Our thorough literature search indicated that post-operative chylopericardium was first reported in early 1970s [6] following surgical repair of pulmonary atresia with VSD. Subsequently, a number of other investigators reported chylopericardium following a number of other surgical procedures, as reviewed, and referenced in our publication [5]. The causation of chylopericardium was not well understood and several hypotheses have been advanced and include obstruction of thoracic duct secondary to thrombosis of the jugular and/or subclavian veins, transection of cardiac lymphatics in the pericardial cavity, injury to the thoracic duct, obstruction to normal flow through the thoracic duct, and/or a combination thereof. High prevalence of variations of the thoracic duct system was pointed out which may predispose to inadvertent injury to the thoracic duct system during surgery [5].
We have also suggested that this complication, though rare, should be added to the list of complications associated with BT shunts [5].
Extensive literature search with the help of an experienced librarian in 1983 prior to submitting the paper for publication did not reveal any reports of chylopericardium following BT shunt without violating the pericardium. Consequently, we stated that chylopericardium following surgery was first reported in early 1970s [6]. Unfortunately, this was incorrect, as pointed out by Dr. Louchimo. These authors from Helsinki, Finland were indeed the first to report chylopericardium following BT shunt in a 21-month-old in German literature (Z Kinderchurgie) in 1966. We did convey our regret for this oversight [7], but PubMed search even in 2019 did not show this citation.
The management of patients with postoperative chylopericardium consists of performing pericardiocentesis to relieve cardiac tamponade and then starting a MCT diet [5, 8]. Repeat echocardiograms to detect any fluid in the pericardial sac should be performed. If need for repeated pericardiocentesis arises, tube pericardiostomy (or per- catheter drainage) should be undertaken. The MCT diet should be followed for at least four weeks and then switched to a normal, fat-containing diet. Again, the patient should be monitored to ensure that no re-accumulation of pericardial fluid ensues. We think that this regimen is likely to be successful in most cases of postoperative chylopericardium. In the uncommon patient resistant to this type of therapy, thoracic duct ligation may have to be performed. We are somewhat opposed [8] to the approach of partial pericardiectomy with or without ligation of the thoracic duct in all patients as advocated by Rose, et al. [9] and associates.
In summary, we reported a rare case of chylopericardium following BT shunt, reviewed the possible causation and offered management strategies. We suggested that this complication should not deter performing BT shunt in babies requiring palliation for cyanotic congenital heart defects (CHDs) with pulmonary oligemia [5, 8].
Surgical Correction of Syndrome Absent Pulmonary Valve With Pulmonary Arterioplasty
Introduction: Syndrome of absent pulmonary valve (SAPV) with tetralogy of Fallot (TOF) is rare variant of TOF. The classic features of this syndrome are rudimentary pulmonary valve cusps, resulting in pulmonary insufficiency; hypoplasia of the pulmonary valve ring, producing pulmonary stenosis; and aneurysmal dilatation of the main and major branch pulmonary arteries, causing varying degrees of tracheobronchial tree compression [10]. These features can easily be demonstrated by echo-Doppler studies (Figure 1 through 3). In this paper, we report successful surgical correction in an infant with this syndrome [11].
![Figure 1: Selected video frame from a 2-D echocardiogram in a parasternal short axis view demonstrating rudimentary pulmonary valve leaflets (arrows) and dilated main and proximal portions of the right and left pulmonary arteries. Ao, aorta; PA, pulmonary artery; RV, right ventricle. Reproduced from Alapti S, et al. [10].](/fulltextimages/11819/fig_1.png)
![Figure 2: Selected video frames from color flow mapping in a parasternal short axis view demonstrating turbulence originating at the pulmonary valve ring level (arrow in A) and pulmonary insufficiency (PI; arrow) in B. MPA, main pulmonary artery; RV, right ventricle. Reproduced from Alapati S, et al. [10].](/fulltextimages/11819/fig_2.png)
![Figure 3: Continuous wave Doppler recording across the right ventricular outflow tract in the same neonate as shown in Figures 1 & 2 demonstrates a severe gradient across the pulmonary outflow tract (87 mmHg – see insert) and pulmonary insufficiency (PI). PS, pulmonary stenosis. Reproduced from Alapati S, et al. [10].](/fulltextimages/11819/fig_3.png)
Case Report: A 13-month old baby with classic features of SAPV (Figures 4A & 5A) with TOF had successful surgical repair by closure of the VSD and relief of the pulmonary valve obstruction. At the same time partial resection and plastic repair of the aneurysmally dilated main and branch PAs was performed by Rao PS, et al. [11]. Clinical, chest x-ray (Figure 4B), cardiac catheterization [11] and angiographic (Figure 5B) data following surgery suggested excellent results.
![Figure 4: A. Chest x-ray in posterio-anterior view performed prior to surgery demonstrating moderate cardiomegaly with dilated right pulmonary artery (arrows). B. Repeat chest x-ray 12 months following surgery showing near normal sized heart and no prominent pulmonary arteries. Reproduced from Rao PS, et al. [11].](/fulltextimages/11819/fig_4.png)
![Figure 5: A. Selected cine frame from right ventricular (RV) cine-angiogram demonstrating markedly dilated main, right (RPA) and left (LPA) pulmonary arteries prior to surgery. B. Repeat cine-angiogram performed following surgery demonstrating marked improvement of the branch pulmonary arteries. Modified from Rao PS, et al. [11].](/fulltextimages/11819/fig_5.png)
Discussion: Two types of clinical presentations of SAVP are known: Group I, neonates with severe respiratory distress and Group II, patients presenting beyond six months of life with no significant respiratory symptoms [10]. Our patent belongs to Group II. It is recommended that plastic repair of the aneurysmal dilated pulmonary arteries (PAs) and closure of the VSD, and surgical relief of right ventricular outflow tract obstruction should be performed early, probably at the age of 1 to 2 years for the group II patients. While some surgeons recommend prosthetic replacement of the pulmonary valve at the time of primary repair [12], our view [11] is that valve replacement is not needed in all cases at the time of primary surgery.
Subsequently, we reviewed our experience with ten patients with SAPV [13, 14]. This presentation reviews our experience with the SAPV and suggests that total surgical correction with PA plication but without pulmonary valve replacement is the method of choice for the correction of this anomaly [13, 14]. Ten infants and children with SAPV seen between 1979 and 1984 were analyzed. Their mean age was 11 months, with a range of one day to three years. Nine children had an associated VSD and pulmonary valve ring stenosis while the remaining infant had an isolated VSD. Five Group I patients (< 6 months) presented with severe tracheobronchial obstruction, cyanosis, and heart failure; five Group II patients (> 6 mo.) presented with a history of recurrent respiratory tract infection and a cardiac murmur. The clinical, x-ray, and echo findings were classic for this anomaly. The two-dimensional echocardiographic features included an enlarged right ventricle and aorta, aortic override, a narrowed pulmonary valve ring with rudimentary pulmonary valve leaflets, and markedly dilated main, right and/or left PAs. Nine patients underwent closure of VSDs and relief of pulmonary valve ring stenosis; four of these also had PA plication and two additionally had a pulmonary valve replacement. Two children died after surgery. Plication of the PAs was performed as the sole procedure in a five-day-old respirator-dependent infant. The follow-up of the remaining eight patients ranged between 1.5 and 3.5 years, and all of them underwent echocardiographic and catheterization studies. The symptomatic relief and normalization of cardiac structure and function were greatest in the patients who had plication of the PAs as an integral part of the total repair, as compared with those who had other types of surgical correction. Based on this experience, we recommend total surgical correction with PA plication but without pulmonary valve replacement as the procedure of choice in symptomatic patients with SAPV [13, 14].
Transient Eosinophilic Pulmonary Infiltration With Intestinal Schistosomiasis and Mitral Stenosis
Introduction: Pulmonary infiltration with eosinophelia (PIE) is rare, but well recognized entity [15]. The association of PIE is even less common with Schistosomia Mansoni infestation [16]. We reported [16]. The association of PIE in a child with mitral stenosis and its successful management [16].
Case Report: A ten-year-old child presented with history of cough and moderate dyspnea. Pertinent clinical findings were palpable liver and spleen and widespread rhonchi and wheezes in both lungs. He also had soft ejection systolic murmur at the left sternal border and a mid-diastolic murmur at the apex with presystolic accentuation. Chest roentgenogram revealed mild cardiomegaly, left atrial enlargement, prominent main PA segment and widespread fluffy pulmonary infiltrates (Figure 6A). Differential count: eosinophils - 19%, neutrophils - 64%, lymphocytes - 11%. Erythrocyte sedimentation rate - 35 mm/hr. Sputum - 40% eosinophils. Bone marrow - marked eosinophilic hyperplasia. Stool - positive for ova of Schistosomia Mansoni and occult blood. Serum immunoglobulins: IgG - 1420 mg/dl, IgA - 205 mg/dl, IgM - 220 mg//dl, and IgD - 1 mg/dl. M-mode echocardiogram showed severely decreased E-F slope of the mitral valve consistent with mitral stenosis. Cardiac catheterization and selective cine-angiography revealed moderate elevation of PA (56/27 mmHg) and PA wedge (mean of 20 mmHg) pressures indicative of significant mitral stenosis. Anti-congestive measures were instituted and treatment with anti-bilharzias (Ambilhar) medication was started. However, the respiratory distress and pulmonary infiltrates (Figure 6B) improved prior to initiation of antibilharzia (Ambilhar) treatment. Three months later, he had successful open mitral commisurotomy.
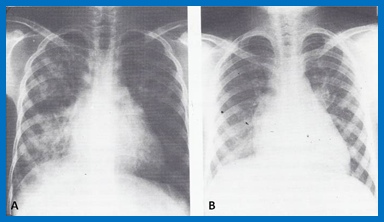
Figure 6A: Chest x-ray in posterio-anterior view at the time of initial presentation showing puffy infiltrations, particularly noticeable in the right lung. B. Repeat chest x-ray five days later demonstrating almost complete clearance of the lung. Reproduced from Rao PS, et al. [16].
Discussion: The pulmonary infiltrates appear to be due to hyper-eosinophilia of Schistosomia Mansoni and not secondary to mitral stenosis in that there were no kerly B lines, cephalization of pulmonary flow or symmetric central haziness, typical for mitral stenosis. The unusual association of PIE and mitral stenosis was recognized and both were treated successfully [16].
Atrioventricular Canal Mimicking Tricuspid Atresia
Introduction: The author encountered a rare case of the common atrioventricular canal (currently called atrioventricular septal defect) mimicking tricuspid atresia (TA) which will be detailed below [17].
Case Report: An eight year old child was seen with a history of cyanosis since birth and decreased exercise tolerance during the preceding year. Physical examination revealed weight and height below 5th percentile, cyanosis, clubbing, prominent left ventricular impulse, a thrill at the left upper sternal border, a single second heart sound, a loud holosystolic murmur at the left lower sternal border, a loud ejection systolic murmur at the left upper sternal border, and no signs of congestive heart failure.
![Figure 7: Selected two-dimensional, subcostal, four- chamber echocardiographic frames with an open (a) and closed (b) atrioventricular valve. Line drawings on the right of a and b are made for greater clarity and for labeling. A large ostium primum atrial septal defect (10 ASD) is shown in a. When the large atrioventricular valve leaflet is open (a), it completely closes the right ventricle (RV) from the right atrium (RA) and the ventricular septal defect (VSD) and allows the emptying of blood from both atria into the left ventricle (LV). When the atrioventricular valve leaflet is closed (b), it continues to occlude the RV from the RA while allowing the VSD to freely communicate between the RV and LV. Ap, Apex; AtTV, atretic tricuspid valve; Ba, base; L, left; LA, left atrium; R, right. Reproduced from Rao PS [17].](/fulltextimages/11819/fig_7.png)
Figure 7: Selected two-dimensional, subcostal, four- chamber echocardiographic frames with an open (a) and closed (b) atrioventricular valve. Line drawings on the right of a and b are made for greater clarity and for labeling. A large ostium primum atrial septal defect (10 ASD) is shown in a. When the large atrioventricular valve leaflet is open (a), it completely closes the right ventricle (RV) from the right atrium (RA) and the ventricular septal defect (VSD) and allows the emptying of blood from both atria into the left ventricle (LV). When the atrioventricular valve leaflet is closed (b), it continues to occlude the RV from the RA while allowing the VSD to freely communicate between the RV and LV. Ap, Apex; AtTV, atretic tricuspid valve; Ba, base; L, left; LA, left atrium; R, right. Reproduced from Rao PS [17].
Chest x-ray revealed mild cardiomegaly and decreased pulmonary vascular markings. Electrocardiogram (ECG) showed left axis deviation and left ventricular hypertrophy. M-mode echocardiogram revealed enlarged left atrium and left ventricle with normal left ventricular systolic function, and a small right ventricle. No tricuspid or pulmonary valve echoes could be recorded; these findings were thought to be consistent with a diagnosis of TA. Two-dimensional echocardiogram demonstrated an ostium primum atrial septal defect, a common atrioventricular valve, and a small right ventricle (Figure 7). Hemodynamic data secured by catheterization were consistent with a diagnosis of TA. Left ventricular angiogram revealed enlarged left ventricle with normal systolic function and prompt opacification of the right ventricle via a VSD, goose-neck deformity of the left ventricular outflow tract, and valvar and sub-valvar pulmonary stenosis. Right atrial cine-angiogram (Figure 8) demonstrated emptying of the contrast material into the left ventricle via an ostium primum atrial septal defect. No direct opacification of the right ventricle was seen. The child had a BT shunt resulting in improved O2 saturation (84%).
![Figure 8: Selected right atrial (RA) angiographic frame in postero-anterior view demonstrating that the floor of the right atrium is formed by one of the leaflets of the atrioventricular valve; this is marked by a large arrow. The contrast material exited the RA via an ostium primum atrial septal defect, shown by small arrows, with subsequent opacification of the left ventricle (LV). LA, left atrium. Reproduced from Rao PS [17].](/fulltextimages/11819/fig_8.png)
Figure 8: Selected right atrial (RA) angiographic frame in postero-anterior view demonstrating that the floor of the right atrium is formed by one of the leaflets of the atrioventricular valve; this is marked by a large arrow. The contrast material exited the RA via an ostium primum atrial septal defect, shown by small arrows, with subsequent opacification of the left ventricle (LV). LA, left atrium. Reproduced from Rao PS [17].
Discussion: The author reported the clinical, radiographic, ECG, echocardiographic, and hemodynamic features of a rare case of the common atrioventricular canal (currently called atrioventricular septal defect) mimicking TA in an eight-year-old child [17]. The clinical, radiographic, and ECG characteristics were similar to those of classic TA. Hemodynamic data secured at cardiac catheterization were also similar to those seen with TA. A two-dimensional echocardiogram demonstrated an ostium primum atrial septal defect with a common atrioventricular valve and a small right ventricle (Figures 7a & 7b); the entry into the right ventricle appeared to be occluded by a leaflet of the common atrioventricular valve. A left ventricular cine-angiogram in posteroanterior view demonstrated a “gooseneck” deformity, similar to that seen in atrioventricular canal defects [17]. However, right atrial angiography resulted in the direct emptying of the contrast material into the left ventricle via an ostium primum atrial septal defect (Figure 8). The floor of the right atrium seems to be formed by a leaflet of the common atrioventricular valve (Figure 8). Thus, the two-dimensional echocardiographic and right atrial cine- angiographic features appear to be distinctive, and may be utilized to distinguish this anomaly from other varieties of TA.
![Figure 9: Line drawings demonstrating two-dimensional echocardiographic appearances in a subcostal four- chamber view of the muscular (A), membranous (B), and atrioventricular canal (C) variants of tricuspid atresia. A. The atretic tricuspid valve is represented by a thick band of echoes between the right atrium (RA) and the small right ventricle (RV) in the muscular type. B. The tricuspid valve is represented by a thin line in the membranous type. Note that crux of the heart (arrows in A and B) is clearly seen in both these types (A and B). The attachment of the anterior leaflet of the detectable atrioventricular valve to the left side of the interatrial septum is evident. C. In the atrioventricular canal type of tricuspid atresia, the anterior leaflet of the detectable atrioventricular canal is attached to the anterior wall of the heart, occluding the right ventricle from the right atrium, and allows the exit of blood from both atria into the left ventricle (LV). The crux cordis and the atrioventricular portion of the inter- ventricular septum are not seen. Reproduced from Rao PS [19].](/fulltextimages/11819/fig_9.png)
Figure 9: Line drawings demonstrating two-dimensional echocardiographic appearances in a subcostal four- chamber view of the muscular (A), membranous (B), and atrioventricular canal (C) variants of tricuspid atresia. A. The atretic tricuspid valve is represented by a thick band of echoes between the right atrium (RA) and the small right ventricle (RV) in the muscular type. B. The tricuspid valve is represented by a thin line in the membranous type. Note that crux of the heart (arrows in A and B) is clearly seen in both these types (A and B). The attachment of the anterior leaflet of the detectable atrioventricular valve to the left side of the interatrial septum is evident. C. In the atrioventricular canal type of tricuspid atresia, the anterior leaflet of the detectable atrioventricular canal is attached to the anterior wall of the heart, occluding the right ventricle from the right atrium, and allows the exit of blood from both atria into the left ventricle (LV). The crux cordis and the atrioventricular portion of the inter- ventricular septum are not seen. Reproduced from Rao PS [19].
The reported anomaly is definitely different from classic TA, but has similar physiologic effects. A detailed review of the literature at the time of that study suggested that this anomaly is extremely rare, with only one brief mention of similar cases by Van Praagh by that time [18]. Evaluation of the crux cordis (Figure 9) on a two dimensional echocardiogram (subcostal four-chamber view) may help to distinguish these anomalies from each other. In the muscular type of TA, a dense band of echoes is seen where the normal tricuspid valve should be (Figure 9A). In membranous types of TA, a thin membrane is seen instead (Figure 9B). In both these types, the anterior leaflet of the detectable atrioventricular valve is attached to the left side of the interatrial septum (Figures 9A & 9B). In the atrioventricular canal type of tricuspid atresia, the crux cordis is abnormal and cannot be identified, and a large atrioventricular valve leaflet occludes the entry of the right atrium into the right ventricle (Figure 9C). It is concluded that two-dimensional echocardiographic and angiographic features help to differentiate the atrioventricular canal type of TA from classic TA cases [17].
Congestive Cardiomyopathy due to Chronic Tachycardia
Introduction: As of the mid-1980s, the importance of treatment of tachycardia by surgical or catheter-based ablation was emphasized to prevent arrhythmia-induced cardiomyopathy. We hypothesized that the reduction of the ventricular rate to normal by drug therapy would result in the regression of arrhythmia-induced cardiomyopathy [20].
Case Report: A three-year-old boy was first evaluated by us in November 1981 because of difficulty in breathing, rapid neck pulsations and tachycardia of one month duration. Similar symptoms occurred repeatedly over a one-year period and were treated elsewhere with digoxin and furosemide with only transient improvement. Physical examination revealed tachycardia (200/min), tachypnea, hepatomegaly, hyperdynamic right and left ventricular impulses, and a grade III/VI holosystolic murmur at the apex with radiation into the anterior axillary line. Chest roentgenogram revealed cardiomegaly and pulmonary venous congestion. ECG revealed supraventricular tachycardia (Figure 10). Echocardiogram revealed enlarged left atrium and left ventricle with markedly diminished left ventricular systolic function (Figure 11A, Table 1)
![Figure 10: Electrocardiogram at presentation showing supraventricular tachycardia (200 beats per minute). Reproduced from Rao PS, et al. [20].](/fulltextimages/11819/fig_10.png)
Further increases in digitalis dosage and carotid massage did not change the cardiac rhythm. Addition of phenytoin did not affect the rhythm. Because of poor left ventricular function, propranolol was not tried. Intravenous verapamil (0.15 mg/kg) produced improvement of the rhythm and the child was started on oral verapamil, 20 mg by mouth three times a day. The dose was gradually increased to 40 mg three times a day. With this regimen of digoxin and verapamil, 2: 1 atrioventricular block developed and resulted in abatement of symptomatology. The patient was discharged home on oral digoxin and verapamil and was followed on an outpatient basis. The child remained asymptomatic and the mitral insufficiency murmur disappeared. Roentgenographic cardiac size and echocardiographic left ventricular size as well as left ventricular function indices, returned to normal within one year and remained normal over the 5.5year follow-up period (Figure 11B and Table 1). ECG continues to show 2: 1 atrioventricular block (Figure 12). Discontinuation of verapamil after two years of treatment resulted in a recurrence of rapid ventricular rate. The verapamil was resumed and the child improved. Electrophysiologic studies to localize the atria1 automatic focus and surgical/ablation therapy were planned for the near future.
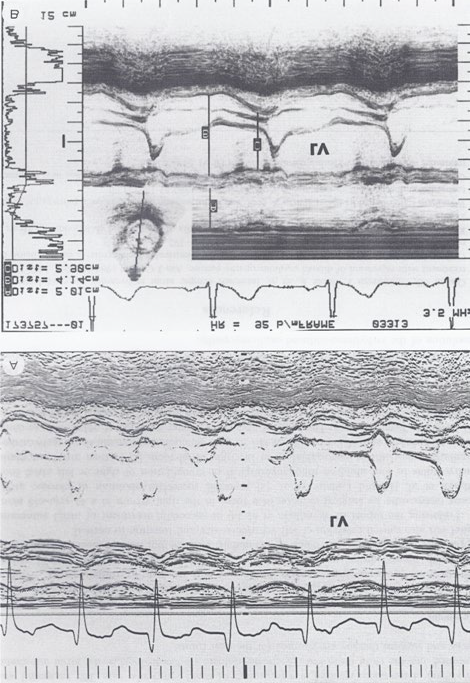
Figure 11A: M-mode echocardiogram of a 3-year-old child who developed arrhythmia-induced cardiomyopathy; note the markedly dilated left ventricle (LV) with poor function (calculated shortening fraction was 13%). B. M-mode echocardiogram of the same patient following successful drug therapy (5.5 years later); note the normal-sized LV with normal function (calculated shortening fraction was 29%). Reproduced from Rao PS, et al. [20].
| At Initial Presentation | After Conversion | One-Year Follow-up | Two-Year Follow-up | Last Follow-up (5.5 years) | |
|---|---|---|---|---|---|
| Ventricular rate, ECG | 200 | 67 | 85 | 96 | 69 |
| CT ratio, X-ray | 0.6 | 0.58 | 0.51 | 0.45 | 0.43 |
| LVEDD, mm, echo | 48 | 50 | 41 | 40 | 41 |
| LVEDD/m2, mm, echo | 87 | 91 | 65 | 53 | 54 |
| LV shortening fraction, % | 13 | 24 | 24 | 32 | 29 |
| PEP/LVET ratio | 0.74 | 0.51 | 0.39 | 0.24 | 0.24 |
| LA/Ao ratio, echo | 1.5 | 1.4 | 1.3 | 1 | 1.1 |
Table 1: Cardiac Rate, Size and Function Prior to and Following Drug Treatment. Ao, aorta; CT, cardiothoracic; echo, echocardiogr
![Figure 12: Electrocardiogram at 5.5 years of treatment showing 2: 1 atrioventricular block with a ventricular rate of 66 beats per minute. Reproduced from Rao PS, et al. [20].](/fulltextimages/11819/fig_12.png)
Discussion: To support our hypothesis that the reduction of the ventricular rate to normal by drug therapy would result in the regression of arrhythmia-induced cardiomyopathy, we presented the case of a three-year-old child who developed arrhythmia-induced cardiomyopathy (Figure 11A) which improved (Figure 11B) with drug therapy [20]. Treatment with medications (Digoxin and Verapamil) resulted in the immediate relief of symptoms, and was followed by a gradual improvement in cardiac size and function (Table 1) with a subsequent return of normal cardiac size and function (Figure 11).
This case demonstrated that reducing the ventricular rate by medication may result in resolving arrhythmia-induced cardiomyopathy and that the surgical excision or catheter ablation of the atrial automatic focus is not necessary in all cases, at least as of the late 1980s. However, it should be noted that enormous advances in pediatric electrophysiology and catheter-based ablation techniques have taken place since the time of our publication [20] and catheter-based ablation of the inciting focus may be an excellent choice at the present time, once the acute symptoms have been controlled by drug therapy [20].
Summary and Conclusion
In this paper, several cases were submitted. The first case describes development of chylopericardium following Blalock-Taussig operation in which the pericardium was not opened. The uniqueness of this complication, possible etiology, and management options were reviewed with the recommendation that this complication should not discourage BT shunts in infants needing palliation of pulmonary oligemia. In the second case, pulmonary arterioplasty was used to treat syndrome absent pulmonary valve without pulmonary valve replacement; based on this case and additional experience in ten other cases, it was suggested that pulmonary valve replacement may not be necessary in infancy to address this scenario. We have observed simultaneous existence of transient eosinophilic pulmonary infiltration secondary to intestinal schistosomiasis and mitral stenosis. The uncommon association of both these entities was pointed out and successful management was documented. A detailed echocardiographic and angiocardiographic pictures of a rare variant of tricuspid atresia with atrioventricular canal was presented. Development of cardiomyopathy secondary to chronic tachycardia and successful reversal of cardiomyopathy with drug treatment was documented in the final case.
References
-
Rao PS (2023) Clinical Case Reports – 1970. Jour of Clin Cas Rep, Med Imag and Heal Sci 5(5): 1-6.
-
Rao PS (2023) Clinical Case Reports 1971-1974. Jour of Med Case Stud 1(1): 1-11.
-
Rao PS (2023) Clinical Case Reports 1976-1979. Jour of Med Case Stud 1(1): 1-8.
-
Rao PS (2024) Clinical Case Reports 1980 - 84 (Contrast Echocardiography). Jour of Med Case Stud 2(1).
-
Feteih W, Rao PS, Whisennand HW, Mardini MK, Lawrie GM (1983) Chylopericardium: A new complication of Blalock-Taussig anastomosis. J Thorac Cardiovasc Surg 85(5): 791-794.
-
Thomas CS, McGoon DC (1971) Isolated massive chylopericardium following cardiopulmonary bypass. J Thorac Cardiovasc Surg 61(6): 945-948.
-
Rao PS (1984) Chylopericardium following Blalock- Taussig anastomosis (Letter). J Thorac Cardiovasc Surg 87: 642.
-
Rao PS, Whisennand HW (1983) Chylopericardium (Letter). Ann Thorac Surg 36: 494.
-
Rose DM, Colvin SB, Danilowicz D, Isom OW (1982) Cardiac tamponade secondary to chylopericardium following cardiac surgery: Case report and review of the literature. Ann Thorac Surg 34(3): 333-336.
-
Alapati S, Rao PS (2021) Tetralogy of Fallot. In: Rao PS, Vidyasagar D (Eds.), A Multidisciplinary Approach to Perinatal Cardiology Volume 2. Cambridge Scholars Publishing, New Castle upon Tyne, UK pp: 1-30.
-
Rao PS, Lawrie GM (1983) Syndrome of absent pulmonary valve: Surgical correction with pulmonary arterioplasty. Brit Heart J 50(6): 586-589.
-
Ilbawi MN, Idriss FS, Muster AJ, Wessel HU, Paul MH, et al. (1981) Tetralogy of Fallot with absent pulmonary valve. Should valve insertion be part of the intracardiac repair. J Thorac Cardiovasc Surg 81(6): 906-915.
-
Rao PS, Mardini MK, Feteih W (1985) Syndrome of absent pulmonary valve. Abstracts of the International Symposium on Cardiovascular Surgery 14: 141.
-
Rao PS, Mardini MK, Feteih W (1986) Syndrome of absent pulmonary valve. Abstracts of the X World Congress of Cardiology 19: 475.
-
Chusid MJ, Dale DC, West BC, Wolff SM (1975) The hyper- eosinophilic syndrome: Analysis of fourteen cases with review of the literature. Medicine (Baltimore) 54(1): 1-27.
-
Rao PS, Harfi HA, Shebib SM, Guinn G (1984) Transient eosinophilic pulmonary infiltration with intestinal schistosomiasis and mitral stenosis. King Faisal Specialist Hospital Med J 4(4): 355-358.
-
Rao PS (1987) Atrioventricular canal mimicking tricuspid atresia: echocardiographic & angiographic features. Brit Heart J 58(4): 409-412.
-
Van Praagh R, Alido M, Dungan WT (1971) Anatomic types of tricuspid atresia: clinical and developmental implications (abstract). Circulation 44(Suppl 2): 115.
-
Rao PS (1997) Tricuspid atresia: anatomy, imaging, and natural history. In: Freedom R (Eds.), Atlas of Heart Disease: Congenital Heart Disease. Philadelphia: Current Medicine 4.0-4.17.
-
Rao PS, Najjar HN (1987) Congestive cardiomyopathy due to chronic tachycardia: Resolution of cardiomyopathy with antiarrhythmic drugs. International J Cardiol 17(2): 216-220.
- Ramsay Hunt Syndrome Presenting as Gait Imbalance without Facial Paralysis: A Case Report
- Unveiling Hidden Culprits: An Observational Study of Upper Gastrointestinal Endoscopy Findings in Symptomatic Cholelithiasis Patients
- Assessing Health Care Providers’ Proficiency in International Patient Safety Goals: A Study to Assess the Knowledge &Practice on Patient Safety in a Tertiary Care Teaching Hospital in Gujarat
- Challenges in Diagnosing Child Language Disorders
- Stunting Service Management Model in the South-Central Timor Region, East Nusa Tenggara, Indonesia
- Acute Small Bowel Obstruction Presenting as Gangrenous Jejunal Loop Secondary to Intestinal Endometriosis – A Rare Case Report