Mortality and Morbidity Associated with Periprosthetic Fracture after Total Knee Replacement
Background: Periprosthetic fractures following total knee arthroplasty are a devastating consequence of an otherwise successful procedure. With an ageing population and extension of total knee arthroplasty to older patients, the rate of these fractures will continue to rise. The purpose of this study was to observe the mortality and morbidity associated with surgical treatment after periprosthetic fracture of total knee replacement. Methods: We retrospectively identified all patients that were admitted to two institutes with a periprosthetic fracture of total knee arthroplasty over a period of five years. Forty five patients underwent operative stabilization (23males and 22 females): by retrograde nailing (n=9), plate fixation (n=32) and 4 revision total knee arthroplasties. Results: Of the 45 patients, there were 20 fractures united within one year of surgery (average 4.8 range 2 to 11months), there was 3 required further surgery for non union (1 following plating and 2 following retrograde nailing). 9 patients died within 6 months of surgery (7 with 4 weeks of surgery). Conclusion: There is a high mortality associated with periprosthetic surgery in the elderly. There was a higher non union rate with retrograde nailing then plating in this group of patients.
Introduction
The number of patients requiring Total knee replacement has increased over the last ten years [1, 2, 3, 4]. With increasing aging population and increased physical demand in older population there is an increased need for joint arthroplasty. This has reflected in a steady increase in the incidence of periprosthetic fractures over last two decades [4]. The management of periprosthetic fractures in the elderly is quite complex. The increased comorbidity associated with elderly patients in combination with poor bone quality makes this a surgical and technical challenge. Various surgical options have been described depending on the site of fracture and fixation of prosthesis. Management of these fracture still remain controversial. The purpose of this study was to observe the mortality and morbidity associated with surgical fixation of periprosthetic fractures of total knee arthroplasty in elderly patients.
Patients and Methods
We retrospectively identified all patients who were admitted to two hospitals - Royal Derby Hospital, Derby, UK and Queens Medical Centre, Nottingham, UK with a periprosthetic fracture following total knee arthroplasty over a period of 5 years. Patients were identified using coding system and each patient’s notes and x-rays were analyzed and data collected. Inclusion criteria: All patients sustaining periprosthetic fractures after total knee replacement (within 5cm from tip of the prosthesis) above the age of 70years. Exclusion criteria: Patients with mid-shaft femoral fractures and periprosthetic fracture of the above hip replacement. Data was collected on patient demographics, co- morbidities, mechanism of injury, pre-operative mobility, ASA grade, grade of surgeon, fixation method, complications, weight bearing status post-operatively and rate of union. Fractures were classified using Rorabeck- Taylor classification [5]. Fracture union was defined as radiographic evidence of bridging callus at the fracture site in both views (4 cortices) combined being non tender on clinically stressing the fracture site and ability to weight bear. Individual medical records and post-operative radiographs were reviewed.
Results
There were 53 patients admitted with periprosthetic fractures during this period: 45 patients (23 males and 22 females) required surgical treatment and 8 patients were treated conservatively as they were stable fractures. In the surgical group, fractures were classified as per RT classification (Rorabeck-Taylor); Type I - 9, Type II – 40 and Type III – 4. 32 patients were treated with open reduction and internal fixation using locking plate – ORIF Group (1 patient only circulage wires) and 9 patients were treated with intramedullary nailing – rIMN Group (retro grade nailing) and 4 patients had revision knee replacement – TKR Group (1patient femoral component only). At the time of injury the mean age was 82.4 years (range 49-95). The most common mechanism of injury was fall from a standing height. There was significant co morbidity in this group of patients, ASA – Grade 2 – 17, Grade 3 – 27 and ASA Grade 4 -1. Pre-injury 8 patients were independent community walkers whilst 26 patients required walking aids, 6 patients were mostly bed bound and 5 unknown mobility statuses. There were 16 medical complications: 9major complications which include 9 deaths within 4 weeks of surgery (4 deaths secondary to Myocardial infraction, 2 congestive cardiac failure and 1 pneumonia) and 2 within 3 months of surgery 1 patient died before discharge from hospital whilst 1 other patient died in the community. There was 5 minor complications which included 1 foot drop, 1 sacral ulcer, 1 DVT, 1 superficial infection and 1 pneumonia. Of 41 patients treated with fixation (either plating or nailing) only 34 survived beyond 3 months (Graph 1). Of these patients, 13 patients had bony union within 3 months of surgery (average 2.8 months range 2-3months) whilst 20 showed delayed-union but united within 11 months (average 6.2months range 4-11). 3 patients had non union or failed fixation required further surgery intervention. Two patient initially treated with IMN was revised to plating and one patients initially treated with plating was converted to IMN for failed fixation. 2 of these patients died before union. At the time of this study, 14 remained alive whilst 20 had died for causes other then surgical. 22 patients returned to their previous mobility status by 3 months of surgery.
Discussion
There are many risk factors associated with periprosthetic fractures after total knee arthroplasty. These include the presence of mechanical stress risers at or around the knee such as anterior femoral notching and screw holes component mal- alignment and poor bone quality – osteoporosis [6, 7]. Adequate surgical technique reduces the chances of early periprosthetic fractures Supracondylar fractures proximal to the femoral knee component are usually better amenable by intramedullary nail fixation, whereas in fractures closer to the knee joint plate fixation by a fixed-angle device might be the method of choice [8]. Some authors favor plate fixation for the treatment of all periprosthetic fractures of the distal femur and have showed excellent results in their studies, whereas other surgeons have reported on a superior outcome by using intramedullary nails [9, 10]. The incidence of non union after periprosthetic fracture is high especially after ORIF compared to intrameduallary nailing [1, 2, 11, 12, 13]. In this surgical group, there were 41 patients requiring fracture fixation; 9 Intrameduallary nailing and 32 ORIF. There was 3 failed fixation or non union requiring further surgical intervention. These results are comparable to previous studies [1, 2]. Intramedullary nailing has higher union rate compared to ORIF. The available evidence shows it is simple, safe and minimally invasive procedure with high success rate by using supracondylar nail. There is minimal soft tissue dissection, allows early weight bearing mobilization with resulting in high union rate surgery [14]. Cadaveric study has reported higher stability compared to LISS Plating system [15]. However there are limitations to this technique as it is not suitable for very low fractures (Type III) and not to be used in previous THR. In recent times, the use of locking plates has shown more promising results with a better union rate [16, 17, 18]. They are particular useful in the presence of periprosthetic fractures with a hip replacement above, as it safely allows stable unicortical fixation overlapping the distal part of the proximal implant, thus avoiding a stress riser between the two implants. Biomedical studies have shown locked plate fixation are superior to non locked plate (dynamic and blade plate) due to the increased torsional forces and pull out strength resulting in better clinical results [19, 20]. All patients in this study treated with ORIF had a locking plate system. Closed technique has its own advantage, the fracture not been exposed and there is limited dissection to soft tissue preventing further trauma. However not all fractures are suitable to be treated with rIMN due to the smaller size of the distal fragment resulting poor purchase. ORIF in a very distal fragment with a previous TKR in situ maybe of significant compromise to the vascularity of the bone leading to non union. However this has not been shown any study models. Three patients had total revision knee replacement and 1 patient had only femoral component revised due to loose components without grafts. In patients with a loose femoral or tibial component, revision arthroplasty with a long-stem prosthesis is usually required, possibly with autografts or allografts, depending on the amount of bone loss [21, 22]. In certain cases, some surgeons might favor management of the fracture first and revision of the components after successful fracture healing, to avoid the necessity of using larger bone grafts [2]. There is a high incidence of morbidity and mortality associated in this group of patients, 9 patients (20%) died within 3 months of surgery. The average age of patients admitted with periprosthetic fractures was above 82 years of age and most patients had associated comorbidity prior to surgery. The surgical outcome is usually associated with higher morbidity23 similar to fracture neck of femurs (Graph 1).
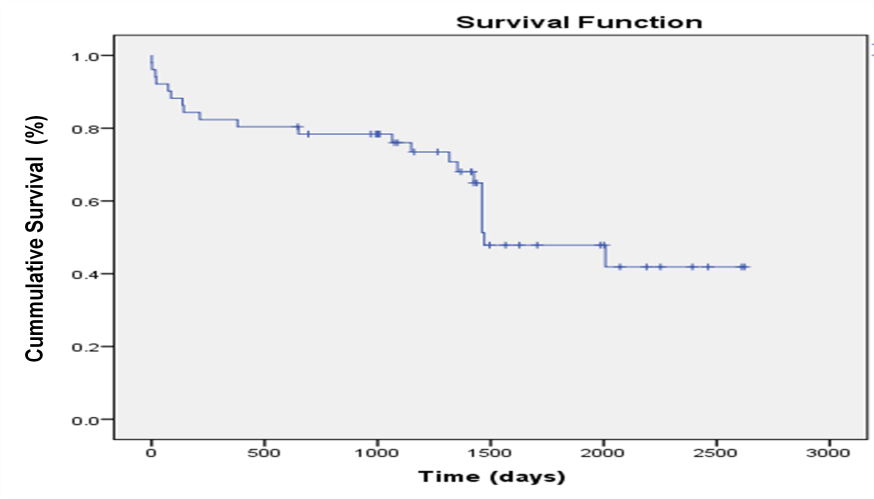
Graph 1: Survival analysis of patients undergoing surgical fixation for periprosthetic fracture.
There was no difference between the groups of different treatments (Table 1). We experience only one superficial infection in this cohort group of patients. Some authors have reported a higher number of infection rates in open fixation compared to IM nailing [14]. Elderly patients usually have associated peripheral vascular disease have a higher chance of would complication leading to higher infection rate [24]. However we did not see any difference in this small group of patients.
| Total | 45 (M 23, F 22) | ||||||
|---|---|---|---|---|---|---|---|
| Average age | 82.4 (range 49-95) | ||||||
| Type of surgery | Nail (9) | ORIF (32) | Revision TKR (4) | ||||
| Union rate at one year | 71% (5/7) 5 (7.4 average 2 to 9mths) | 96% (25/26) 25 (4.58 range 2 to 11mths) | NA | ||||
| Non union | 2 revised | 1 revised | NA | ||||
| Mortality at 3 months | 2 (22%) | 6 (18%) | 1 (25%) | ||||
| Minor | 5 |
Table 1: Patients undergoing surgical management after periprosthetic fracture. This study has a small cohort group, and the conc
Table 1: Patients undergoing surgical management after periprosthetic fracture. This study has a small cohort group, and the conclusions drawn are limited. Surgical option has to be balanced against complications and risks. Given the fact most of these fractures are unstable and require internal fixation for stabilization in order to get patients mobile sooner to prevent complications secondary to bed rest, and allowing stabilization of the fracture to allow early mobilizing of the knee. Fracture fixation also enables a better mean of pain control and easy nursing justifying surgery even in the elderly.
Conclusion
Surgical treatment of periprosthetic fractures in the elderly is associated with significant mortality. There is a higher non union rate of rIMN group demonstrate in this study.
References
-
Kim KI, Egol KA, Hozack WJ, Parvizi J (2006) Periprosthetic fractures after total knee arthroplasties. Clin Orthop Relat Res 446: 167-175.
-
Su ET, Hargovind D, Di Cesare P (2004) Periprosthetic femoral fractures above total knee replacements. J Am Acad Orthop Surg 12(1): 12-20.
-
Felix NA, Stuart MJ, Hanssen AD (1997) Periprosthetic fractures of the tibia associated with total knee arthroplasty. Clin Orthop Relat Res 345: 113-124.
-
Berry DJ (1990) Periprosthetic fractures after major joint replacement. Epidemiology: hip and knee. Orthop Clin North Am 30(2): 183-190.
-
Rorabeck CH, Taylor JW (1999) Classification of periprosthetic fractures complicating total knee arthroplasty. Orthop Clin North Am 30(2): 209-214.
-
Lesh ML, Schneider DJ, Deol G, Davis B, Jacobs CR, et al. (2000) The consequences of anterior femoral notching in total knee arthroplasty: a biomechanical study. J Bone Joint Surg Am 82A: 1096-1101.
-
Shawen SB, Belmont PJ, Klemme WR, Topoleski LDT, Xenos JS, et al. (2003) Osteoporosis and anterior femoral notching in periprosthetic supracondylar fractures. A biomechanical study. J Bone Joint Surg Am 85A: 115-121.
-
McGraw P, Kumar A (2010) Periprosthetic fractures of the femur after total knee arthroplasty. J Orthopaed Traumatol 11(3): 135-141.
-
McLaren AC, Dupont JA, Schroeber DC (1994) Open reduction internal fixation of supracondylar fractures above total knee arthroplasties using the intramedullary supracondylar rod. Clin Orthop Relat Res 302: 194-198.
-
Figgie MP, Goldberg VM, Figgie HE, Sobel M (1990) The results of treatment of supracondylar fracture above total knee arthroplasty. J Arthroplasty 5(3): 267-276.
-
Healy WL, Siliski JM, Incavo SJ (1993) Operative treatment of distal femoral fractures proximal to total knee replacements. J Bone Joint Surg Am 75(1): 27- 34.
-
Culp RW, Schmidt RG, Hanks G, Mak A, Esterhai JL, et al. (1987) Supracondylar fracture of the femur following prosthetic knee arthroplasty. Clin Orthop Relat Res 222: 212-222.
-
Nielsen BF, Petersen VS, Varmarken JE (1988) Fracture of the femur after knee arthroplasty. Acta Orthop 59(2): 155-157.
-
Herrera DA, Kregor PJ, Cole PA, Levy BA, Jonsson A, et al. (2008) Treatment of acute distal femur fractures above a total knee arthroplasty: systematic review of 415 cases (1981-2006). Acta Orthop 79(1): 22-27.
-
Bong MR, Egol KA, Koval KJ, Kummer FJ, Su ET, et al. (2002) Comparison of the LISS and a retrograde- inserted supracondylar intramedullary nail for fixation of a periprosthetic distal femur fracture proximal to a total knee arthroplasty. J Arthroplasty 17(7): 876-881.
-
Althausen PL, Lee MA, Finkemeier CG, Meehan JP, Rodrigo JJ (2003) Operative stabilization of supracondylar femur fractures above total knee arthroplasty: a comparison of four treatment methods. J Arthroplasty 18(7): 834-839.
-
Raab GE, Davis CM (2005) Early healing with locked condylar plating of periprosthetic fractures around the knee. J Arthroplasty 20(8): 984-989.
-
Ricci WM, Loftus T, Cox C, Borrelli J (2006) Locked plates combined with minimally invasive insertion technique for the treatment of periprosthetic supracondylar femur fractures above a total knee arthroplasty. J Orthop Trauma 20(3): 190-196.
-
Koval KJ, Hoehl JJ, Kummer FJ, Simon JA (1997) Distal femoral fixation: a biomechanical comparison of the standard condylar buttress plate, a locked buttress plate and the 95 degree blade plate. J Orthop Trauma 11(7): 521-524.
-
Marti A, Fankhauser C, Frenk A, Cordey J, Gasser B (2001) Biomechanical evaluation of the less invasive stabilization system for the internal fixation of distal femur fractures. J Orthop Trauma 15(7): 482-487.
-
Cordeiro EN, Costa RC, Carazzato JG, Silva JDS (1990) Periprosthetic fractures in patients with total knee arthroplasties. Clin Orthop 252: 182-189.
-
Kumar A, Chambers I, Maistrelli G, Wong P (2008) Management of periprosthethic fracture above total knee arthroplasty using intramedullary fibular allograft and plate fixation. J Arthroplasty 23(4): 554- 558.
-
Clement ND, Aitken SA, Duckworth AD, McQueen MM, Court-Brown CM (2011) The outcome of fractures in very elderly patients. Journal of Bone & Joint Surgery - British Volume. 93(6): 806-810.
-
Boettcher WG (1992) Total hip arthroplasties in the elderly. Mortality, morbidity and cost effectiveness. Clinical orthopaedics and related research 274: 30- 34.
- Return to Work Among Manual Workers After the Latarjet Procedure: A Cohort Study of 43 Patients
- Refractory Pelvic Collection Following Modified Stoppa Approach for Both-Column Acetabular Fracture Fixation: A Case Report
- Comparative Study of Dynamic Knee Phenotypes Under Loaded and Unloaded Conditions: Clinical Impact
- Locked Intramedullary Nailing of the Tibia Using a Humeral Nail: A Care Case Report
- Subtalar Dislocation: About a Case Report
- Surgical Site Infection in Orthopedics in a Country with LimitedResources: Indications, Treatment and Results