“Cubital Tunnel Syndrome Due to Ganglion Associated with Ulnar Neuropathy”: A Case Report
We report a case of ulnar neuropathy by a ganglion in the cubital tunnel. A 52 year old male presented in our OPD with tingling and numbness over medial side of left hand and left 4th and 5th fingers since 2 months which increased on prolonged flexion and during night time. On clinical examination there was wasting of both ulnar forearm and hypothenar muscles with thickening of ulnar nerve and tenderness at medial aspect of elbow and decreased hand grip .CARD test and EGAWA test positive and FROMENT sign present. X-ray of left elbow (AP and Lateral View) showed osteophytes at ulno-humeral joint. During surgery a 2-cm diameter ganglion arising from ulno-humeral joint compressing the ulnar nerve was identified. Ganglion cyst excised and ulnar nerve was transposed anteriorly. Biopsy of the material confirmed it as a ganglion. Patient recovered satisfactorily 3 months after the surgery.
Introduction
Ganglia can occur anywhere in the body but they are common in hand and foot region. Ganglions are filled with synovial fluid but over time it becomes jelly in consistency and they arise from synovium of joints, tendon sheaths and also from nerves [1]. Although they are benign they can cause problem when they compress the nerves giving rise to pain, numbness and atrophy of the muscles. Medial elbow ganglion is the 3rd commonest cause of cubital syndrome and its prevalence is around 8 % [2]. We present a case of cubital syndrome due to ganglion at ulnohumeral joint associated with ulnar neuropathy and its surgical management with excision and ulnar nerve anterior transposition.
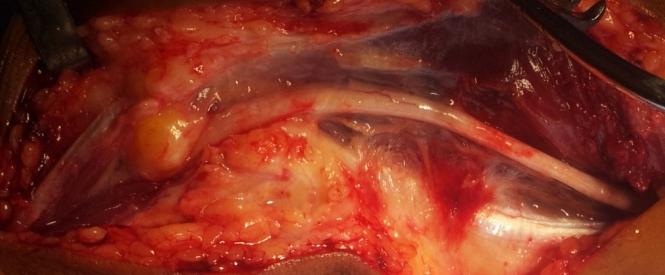
52 years old male presented at our outpatient department with 2 months history of tingling and numbness over medial side of left hand and left 4th and 5th fingers .The pain was gradual in onset and progressive in nature. Pain increased on prolonged flexion of elbow and was more during night. There was no previous history of elbow or neck injuries or other medical disease. On examination, wasting of ulnar forearm and hypothenar muscles was present. On palpation, tenderness below medial epicondyle and thickening of ulnar nerve was noted. In addition, he had weakness of the left hand with decreased grip strength, positive CARD test, EGAWA test and FROMENT sign positive. Sensory disturbance over medial one and a half fingers of left hand was present Except restriction of 10 degree flexion at elbow all other movements within normal range .Signs of elbow instability were absent. Using a anteromedial approach through a medial incision, ulnar nerve identified and delineated from middle third arm to proximal forearm and cubital tunnel was released. Ganglion cyst (Figure 1) around 2 cm diameter originating from ulnohumeral joint was excised (Figure 2) and sent for biopsy. Constriction of ulnar nerve (Figure 3) at compression site was noticed. Excision of osteophytes at ulnohumeral joint was performed (Figure 4) and cubital tunnel was resutured. Ulnar nerve was transposed anteriorly (Figure 5) and wound closure was done. On the 2nd post operative day, physiotherapy in the form of elbow, finger and wrist mobilization started. After three months patient showed satisfactory improvement.




Discussion
Ganglions may arise from joint synovium or may communicate with tendon sheaths, tendons, nerves, or joints [3]. In addition, most ganglion cysts involving nerves originate from the adjacent joints [4, 5]. In the largest series of 38 cases of ganglion cysts compressing the ulnar nerve in the cubital tunnel, all cysts originated from the medial aspect of the ulnohumeral joint [2]. Ulnar nerve entrapment is the 2nd most common nerve entrapment syndrome of the upper extremity. It can occur anywhere along the course of ulnar nerve but cubital tunnel is the most common site. The symptoms involve pain, numbness, sensory impairment in the medial border of the forearm and hand which is the area of distribution of the ulnar nerve, reduced grip strength, and wasting of the intrinsic hand muscles [5]. Treatment is decided by the site of pathology. It can be treated conservatively but when it fails or sensory or motor impairment increases then surgical intervention in the form of decompression and anterior transposition should be done.
Conclusion
Hippocrates described ganglion cysts as “knots of tissue containing mucoid flesh” [6]. Although uncommon, medial elbow ganglia have a strong association with osteoarthritis of the elbow and can cause a relatively acute onset of cubital tunnel syndrome. A patient with cubital tunnel syndrome associated with elbow osteoarthritis who complains of medial elbow pain or severe numbness within two months after the onset of the syndrome should be strongly suspected of having a ganglion. Careful excision of the ganglion performed concurrently with subcutaneous anterior transposition of the ulnar nerve can produce satisfactory results.
References
-
Feldman MD (2000) Arthroscopic excision of a ganglion cyst from the elbow. Arthroscopy 16(6): 661-664.
-
Kato H, Hirayama T, Minami A, Iwasaki N, Hirachi K (2002) Cubital tunnel syndrome associated with medial elbow ganglia and osteoarthritis of elbow. J bone joint surg Am Aug 84-A(8): 1413-1419.
-
Athanasian EA (2005) Bone and soft tissue tumors. In: Green DP, ed. Operative Hand Surgery. 5th (Edn.), New York, NY: Churchill Livingstone 2221-2239.
-
Harbaugh KS, Tiel RL, Kline DG (1997) Ganglion cyst involvement of peripheral nerves. J Neurosurg 87(3): 403-408.
-
Sharma RR, Pawar SJ, Delemndo A, Mahapatra AK (2000) Symptomatic epineural ganglion cyst of the ulnar nerve in the cubital tunnel: a case report and a brief review of the literature. J Clin Neurosci 7(6): 542-543.
-
Teh J, Whiteley G (2007) MRI of soft tissue masses of the hand and wrist. Br J Radiol 80(949): 47-63.
- Return to Work Among Manual Workers After the Latarjet Procedure: A Cohort Study of 43 Patients
- Refractory Pelvic Collection Following Modified Stoppa Approach for Both-Column Acetabular Fracture Fixation: A Case Report
- Comparative Study of Dynamic Knee Phenotypes Under Loaded and Unloaded Conditions: Clinical Impact
- Locked Intramedullary Nailing of the Tibia Using a Humeral Nail: A Care Case Report
- Subtalar Dislocation: About a Case Report
- Surgical Site Infection in Orthopedics in a Country with LimitedResources: Indications, Treatment and Results