Have Countries Ignored Infertility for Too Long? - India Case Study
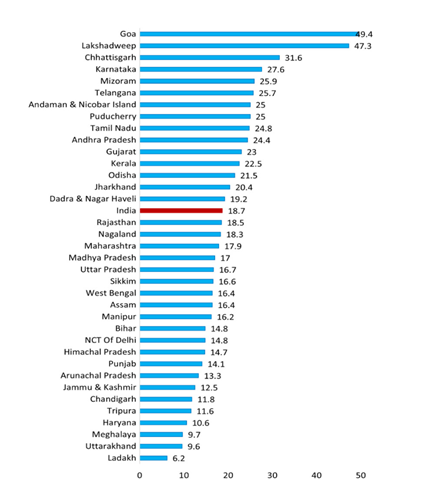
Fertility has been one of man’s desired attributes since the beginning of recorded history and remains a driving need for young couples to prove their fertility as soon as possible after marriage. Though this trend is changing a bit over a decade, due to some people with higher education, getting married late, working couple and some who are intentionally delaying parenthood. In India, pregnancy is usually viewed as a normal physiologic phenomenon, that does not require any intervention by professionals, unless there is some problem in conceiving, or pregnancy going to full term or in birthing. Most Indian families believe that they have little or no control over their pregnancies or outcomes. The importance of motherhood in traditional patriarchal cultures is rooted in the teachings of all the religions. The World Health Organisation (WHO) has recognised infertility as a public health issue. Although biological factors are the primary cause, factors like social, health, and lifestyle factors do have an adverse effect on a couple’s ability to reproduce. The current fertility rate for India in 2024 is 2.122 births per woman, in 2023 it was 2.139 births per woman, in 2022 it was 2.159, in 2021 = 2.179 births per woman, and 2.159 in 2020, witnessing a reduction of 0.95% each year. Replacement level fertility needed to maintain a stable population size, is estimated to be 2.1. below which the population starts declining as we see in China (1.705 in 2023) today. High levels of infertility will generate low desire for contraception. Fertility and infertility are social conditions which are intricately connected. Where fertility is highly valued, infertility will conversely be devalued. Infertile across Indian women in 2019-21 (NFHS-5) by duration of marriage varied from i) women married for ≥1 year = 42.9%, ii) married for ≥2 years =30.7% Married for ≥3 years =24.1%, married duration ≥4 years =20.7% and married for ≥5 years = 18.7%. Age at marriage, biological factors, and lifestyle factors are strongly linked to infertility. People with higher education levels, late marriages, working couple and those intentionally delaying parenthood are more likely to experience primary infertility. Materials and Methods: This article is based on authors experience of guiding four cases of primary sterility in last 5 years. For different reasons first case has succeeded, second is progressing towards success, third is 30% hopeful as the cause is not necessarily associated with infertility and in the fourth all efforts have failed except IVF which the couple could not afford. The case studies suggest that Infertility in India needs to be Public Health Concern!
Introduction
Fertility has been one of man’s desired attributes since the beginning of recorded history and remains a driving need for young couples to prove their fertility as soon as possible after marriage. Though this trend is changing a bit over a decade, due to some people with higher education, getting married late, working couple and some who are intentionally delaying parenthood. In India, pregnancy is usually viewed as a normal physiologic phenomenon, that does not require any intervention by professionals, unless there is some problem in conceiving, or pregnancy going to full term or in birthing. Most Indian families believe that they have little or no control over their pregnancies or outcomes. The importance of motherhood in traditional patriarchal cultures is rooted in the teachings of all the religions. Infertility is viewed as a curse, having significant negative social impacts on the lives of the couples. While women, experience violence, divorce, social stigma, emotional stress, depression, anxiety and low self-esteem, men too if they are found to be oligospermia [1]!
When India launched its first national family planning programme in 1952, the best reproductive outcomes for women and concerns about policies on families and reproductive health were paramount. Seventy-two years later, despite a rights-based approach to population planning, those questions continue to haunt the nation. Most importantly Infertility remains ignored in Indian population policy and its absence, understood as a technique of reproductive governance, offers insights on potential solutions [2].
The World Health Organisation (WHO) has recognised infertility as a public health issue. Although biological factors are the primary cause, factors like social, health, and lifestyle factors do have an adverse effect on a couple’s ability to reproduce. A male factor is thought to contribute to roughly half of cases, as a sole contributor in about 20% of infertile couples, in conjunction with a female infertility factor in 30% of infertile couples [3].
A multivariate logistic regression Of NFHS data (NFHS 1-4) among Indian couples indicated that the prevalence of primary infertility at national, regional levels has decreased from 1992-93 to 2005-06 but it showed a remarkable increase in 2015–16 compared to 2005–06, largely in the Southern states. Age at marriage, biological factors, and lifestyle factors were all strongly linked to infertility. The urban women are more prone to experience infertility due to the differentials in environment and lifestyles. The findings of a recent study suggest that moderate solar radiation exposure benefits women in their 30s while trying to conceive and the lack of the same in urban lifestyle may contributorily factor among couples who opt delayed choice of parenthood [4]. An inverse relationship exhibited between the level of educational attainment, standard of living and primary infertility among the women. The other plausible reasons could be the greater awareness of infertility treatments among highly educated women and increased access to expensive treatments by the richest. Moreover, factors like vegetarian diet, overweight, obese, thyroid patient were strongly associated with primary infertility [3]. India has a large population, but population growth has reached below replacement level especially in Urban India. Current estimates of the Total Fertility Rate or TFR is at 2.1 in rural areas and 1.6 in urban areas. The Total Fertility Rate (TFR) further declined to 2.0 children per woman in 2019-21 (NFHS-5) from 2.2 [1].
Public Health Action Plan for the Detection, Prevention, and Management of Infertility, need to understand and address issues at a population level that contribute to and are caused by infertility in women and men and that may affect the health of the pregnancy by Promoting healthy behaviours that can help maintain and preserve fertility and Promoting prevention, early detection, and treatment of medical conditions that can threaten fertility.
Case Reports
Vani a Successful Conception after 3 Courses of Hormone Therapy: Vani an M.Sc. scholar aged 28 years now working as scientist in private sector, was married in May 2021, in a small function due to Covid 19 Pandemic. As a traditional woman head single parent family after 1 year of Marriage, expectations increased from both girl and the boy’s side. She underwent her first Gynaecological check-up in June 2022 in a private Nursing Home in Bengaluru. As expected, she was put on a hormonal therapy for 3 months. Wait for another 3months did not result in pregnancy. The consultant Gynaecologist got a Follicular Study and Transvaginal Scan (TSV) The scan report of 22 October 2023 read: Retroverted Uterus, Normal size (5.3x2.9x3.5 cms) with homogenous endometrial echoes, both ovaries were normal in size, both adnexa were also normal.
On 1 November she got a battery of test done including anti-Mullerian hormone, Thyroid hormones, Random Blood sugar, Serum Creatinine, PAP smear, Rubella antibodies, HIV 1&2, HbsAg, Hepatitis C antibody, VDRL, CBC, Hb1Ac and Varicella IGG, and KUB (kidney ureter bladder) and Pelvic scan, all of them were normal except the Right ovary showing a dominant follicle measuring (1.4x1.4x14 mm). She was put on Normoz (used to treat PCOS and Conceiving issue) Tablet twice a day and multiple nutritive supplements for 3 months from early November 2022, by February 2023 her periods got regularised but with no success until April 2023. Her husband’s sperm analysis was got done, which was normal. She then changed her Gynaecologist in June 2023. Again, she was put on hormonal therapy which continued for 4 months till September 2023. She missed her periods in December 2023 cycle. An Obstetric first Trimester scan, Doppler and other routine tests on 23 February 2024 confirmed her pregnancy with a single intrauterine gestation of 12 weeks and 2 days with an adjusted risk of downs syndrome of 1:6371 and called to return for ruling out foetal anomalies in 20th week. Has been advised not to travel, lift weights etc with standard nutritional supplements. This couple have spent about INR 100,000 (US $ 1200) so far for the treatment.
| Day of Cycle | Endometrial Thickness (mm) | Right ovarian Follicles (mm) | Left ovarian Follicles (mm) | Remarks | |
|---|---|---|---|---|---|
| 20-09-2022 | 11 | 4.7 | Irregular follicle | 13x11, 14x9 | Follow up on 22/09 |
| 22-09-2022 | 13 | 6 | “ | 16x14, 14x10 | Follow up on 24/09 |
| 24-09-2022 | 15 | 8 | “ | 19x19, 14x16 | Follow up on 26/09 |
| 26-09-2022 | 17 | 9 | “ | 24x20, 13x7 | Follow up on 28/09 |
| 28-09-2022 | 19 | 11 | “ small | 31x27, 13x7 | With minimal lacy echoes s/o haemorrhagic Cyst |
| 22-10-2022 | 11 | 6 | 1.4x1.4x1.4 | Small | Rescan on 24th |
| 24-10-2022 | 14 | 8 | 23x9 | Small | Rescan on 24th |
| 27-10-2022 | 16 | 10 | 27x20 | Small | Rescan on 29th |
| 29-10-2022 | 18 | 13 | 29x22 | Small |
Table 1: The Scan Report Results.
Deepa’s Case of Gobbled Foetus in First Gravida & Efforts in Progress: Deepa got married in 2018, but desired delay the first pregnancy as she was just 24 years old then and was very leanly build. She tried to put on weight and succeeded over period of 1 year to add about 23 kgs to her original weight of 52 Kg. Looking at her bloating she was advised diet and reduce the weight to around 60kg which she achieved. The Covid 19 Pandemic in 2020 and 2021 and father-in- law diabetic food ulcer, recommended amputation (in 2022 and early 2023), further delayed their plan of conceiving. After having sorted out his father’s problem by conservative management and saving the foot, the couple were ready for parenthood. Finally, they gave a happy news of conception on 24 October 2023, The Ultrasonography report read “Single pregnancy, gestational sac of 21.X1.1 cms and yolk sac of 4 mm, inferring 8 weeks pregnancy. Next week they reported with c/o spotting. Though general condition was fine with BP= 130/80, weight 64 Kg, a transvaginal scanning showed Blighted ovum, for which her Gynaecologist a medical or surgical MTP. At this juncture I was consulted. I got her a second obstetric consultancy with close friend, who confirmed the gobbled status of the foetus and tried medical termination with hormone therapy. After 4 week she did a D&C and cleaned the uterus completely and advised the couple to abstain for sex for 3 months. After another course of hormonal therapy for 3 months, having got checked by the Gynaecologist last week she is ready to conceive this month. This couple have spent so far INR 150,000 for consultations, investigations, medicines, and intervention (D&C).
Shilpa a Primigravida case of Septate Uterus ending in MTP: Shilpa aged 27 years is a Homeopathy graduate and one of My MPH scholars between 2020-2022. She got married to one of her MPH classmates on 26th January 2023. On 29th October 2023 she happily informed about her first pregnancy, what was short-lived happiness as Her First Trimester Scan (OFTS) identified her as having Septate uterus, Low lying placenta, her Blood group was O negative, thus diagnosed as very risky pregnancy. On an anomaly scanning around 20th week on 22 November 2023 noting cervical incompetence and single umbilical artery she underwent a Cervical stitch. During the process itself the gynaecologist found membrane tear and mild leakage of amniotic fluid, gave her only 50% chance of continued pregnancy. On 24th November another scan to assess the status due to continued leakage, found no amniotic fluid in the uterus, and placenta previa and babies’ heartbeat. With no hope of baby’s survival, she was advised and underwent an MTP. There ended a happy dream! The couple spent almost INR 300,000 (US $ 3500). Suma’s Unsuccessful Story: Suma a twenty-eight-year-old lady then married for 5 years was investigated for infertility in a private Nursing home in 2018-19. After a Scan and D&C was done and put on hormone therapy for three months. After about 6 months as there was no conception husband went through a thorough examination and semen analysis. After ascertaining time of the puberty, current sexual function, and frequency of sexual intercourse, a history of sexually transmitted infections and investigations, testicular trauma, prostatitis, and mumps orchitis and any medications was obtained. Physical examination and Semen analysis was got done to learn that he had oligospermia and reduced mobility of the few sperms. FSH and LH, and testosterone were also investigated, but no inference could be drawn on the cause of oligospermia. He was put on human chorionic gonadotropin (hCG) 2500 IU Subcutaneous on alternate days for three months along with Isotretinoin (active form of Vit. A) supplementation, which did not improve much either the sperm count or mobility. An in vitro fertilization with or intracytoplasmic sperm injection was recommended, clearly spelling that only 40-50% chances of success and costing around INR 500,000 (US$6000). Having spent about INR 200,000 (US $ 2500) over a year the couple decided to continue to be childless.
Discussions
There is much confusion between falling TFR and increasing infertility. TFR is suggestive of the willingness to procreate whereas fertility is the ability to procreate. All India Institute of Medical Science (AIIMS) New Delhi, and many other academic institutes estimate the current infertility to be in the range of 10-15% in India. These studies point to the fact that although infertility is a result of underlying medical conditions, it is multifactorial condition. Along with the underlying medical reasons, an overlap of other common factors like stressful lifestyles, pollution, obesity, high intake of junk food, smoking, alcoholism, drug addiction, or substance abuse, and the tendency of couple to opt for late parenthood. Age has a definite negative relationship with fertility, particularly with a woman’s ability to become a mother. The findings of a recent study suggest that moderate solar radiation exposure benefits women in their 30s while trying to conceive and the lack of the same in urban lifestyle may contributorily factor among couples who opt for delayed choice of parenthood [3]. The critical use of pesticides and fertilizers are incremental contributory factors, as endocrine disrupting chemicals like automobile exhaust diesel particulate matter, Bisphosphenol, and phthalates in plastics also contribute for infertility especially in cities.
The Total Fertility Rate (TFR) further declined to 2.0 children per woman in 2019-21 (NFHS-5) from 2.2 children per woman as per NFHS-4 conducted during the year 2015-16, resulting in the achievement of the replacement. Infertility defined as a couple not able to achieve a pregnancy after 12 months or more of regular unprotected sexual intercourse, the WHO estimates the prevalence of infertility in India to be between 3.9% and 16.8%. While the reported number is around 30 million couples, but it may be around 50 million [3]. The data of 491,484 currently married women in the age group of 15–49 years, extracted from the National Family Health Survey of NFHS 5 showed that the prevalence of infertility is 18.7 per 1,000 women among those married for at least five years and currently in union. This prevalence increases as the duration of marriage decreases. Infertile across 491484 Indian women by duration of marriage varied from i) women married for ≥1 year (N=21089, IF-21089) was 42.9%, ii) Married for ≥2 years (N=473697, IF-14530=30.7% Married for ≥3 years (N=454714, IF= 10958=24.1%, married duration ≥4 years (N=436803, IF= 9044 =20.7% and Married for ≥5 years (N=419293, IF=7853 = 18.7%.) [5]. Goa, and Chhattisgarh and UT Lakshadweep, exhibit the highest burdens [1]
Infertility is increasing amongst eligible Indian couples. In India probably across the world, existing culture considers for practical purposes only live or surviving birth to count fertility. For example, cases of Deepa and Shilpa technically are not infertility, but of the family and community they are infertile.
Magnitude of the Problem (Prevalence of Primary Infertility)
The prevalence rate of primary infertility in urban population of Central India is lower than reported trends of infertility from southern states and developing countries. The overall prevalence of primary infertility among reproductive age group women was 8.9% (51/570). Most of the Infertile women (39.3%) belonged to 25–29 years of age group. Age at marriage more than 25 years (P < 0.05), nuclear family (P < 0.05), higher education level (P = 0.04), employed women (P < 0.05), high socioeconomic status (P = 0.01), and family history of infertility (P < 0.05) were the sociodemographic factors that had statistically significant association with infertility. Physiological factors that had statistically significant association with infertility were obesity (P = 0.03), age at menarche more than 14 years (P < 0.05) and irregular menstruation pattern -PCOD (P < 0.05). The psychological factors significantly associated with infertility were Depression (P = 0.01) and stress (P < 0.05) [6].
Causes of Infertility
• Common Causes for both Male & Female: One of the most common causes of infertility is obesity, which affects both men and women. Tobacco abuse, excessive alcohol, or use of marijuana, heroin, or cocaine affect negatively. Fast foods not rich in nutrition and contain harmful preservatives contribute to infertility in both men and women in urban areas.
• Female Infertility Causes: Underweight is an equal risk, for women, as it can lead to ovarian dysfunction and infertility. Recent research suggests that an inadequate exposure to sunlight reduces the ovarian reserve again an urban additional risk. AMH plays a crucial role in the development of a baby’s sex organs during gestation. A study involving 2,235 women aged 20-40 in Israel examined the levels of anti-Müllerian hormone (AMH) in women aged 20-40 and how these levels fluctuated throughout different seasons. The results found no association between AMH levels, seasons, or solar radiation intensity in the younger group. However, for those aged 30-40, AMH levels increased in spring and autumn with moderate solar radiation, compared to winter with low radiation. This phenomenon was more evident in women with 36-40 subset showing higher AMH levels during months of moderate solar intensity and in summer compared to winter. The findings suggest that moderate solar radiation exposure benefits women in their 30s while trying to conceive [7].
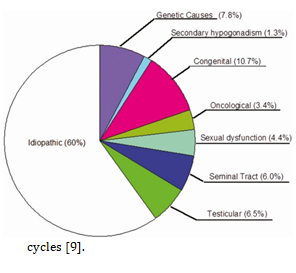
• Male Infertility: Male infertility secondary to oligozoospermia is common in India. Most of these cases are idiopathic, sometimes oligozoospermia can be caused by endocrine dysfunction, anatomic abnormalities, or medications. For men, strenuous work, and medication that affect sexual function and the use of body-building medications, androgens, reduce fertility. The work-up includes excluding reversible factors such as hormonal deficiency, medication effects, and retrograde ejaculation and identifying any underlying genetic syndrome and treating reversible medical causes. If no reversible cause is found, assisted reproductive technology need to be initiated [8]. Unfortunately, even with a comprehensive work-up, two thirds to three quarters of men will not receive a clear diagnosis to explain their oligozoospermia. Though deficiency of GnRH secretion is most often a congenital condition. Intrauterine insemination is considered as initial therapy; but most Andrologist advise directly to in vitro fertilization with or without Intracytoplasmic sperm injection. Fertilization rates in the 50% to 75% range are reported, and the clinical pregnancy rate per cycle is around 20%, with an overall cumulative live birth rate of around 50% after 3 cycles [8].
• Outcome of Pregnancy in Women with Septate Uterus & Infertility: A septate uterus is rare, but it’s one of the more common uterine anomalies. It accounts for approximately 35% to 90% of congenital uterine irregularities. Congenital uterine anomalies occur in 4% of all people who have a uterus. In India Septate Uterus has a prevalence of 2-3% in women of reproductive age and is associated with a higher risk of perinatal complications and lower clinical pregnancy rates, like an increase in the risk of miscarriage, premature delivery, and malpresentation. Among the primary infertile woman, the success rate of conception after spectrum resection is around 30% and live birth in less than 20%.
A study of after Hysteroscopic septum resection (AHSR) in 19 primary infertile patients, 6 (32%) patients conceived which resulted in live birth rates of 67% (n=4). Similarly, AHSR on seven patients with the history of secondary infertility, post-operative, pregnancy rate was 86% (n=6), and the live birth rate was 67% (n=4). Hysteroscopic septum resection using bipolar versa point system is an effective and safe approach for the removal of septum. Therefore, our case Shilpa can hope to conceive soon [4, 9].
Treatment Seeking Behaviour of Infertility Women: A cross-sectional study from the two high infertility prevalence districts after complete mapping and listing to identify the eligible respondents. A total of 159 ever-married women (20–49 years) out of 172 identified women were interviewed. Among 159 interviewed women, only three did not seek any kind of treatment. Of the 156 women, 63, 65, and 28 women (mutually exclusive) received first, second and third-order treatment, respectively. The number of women decreased in the succeeding phases of infertility. Women aged above 35 years, were significantly less (OR = 0.310, p < 0.05) compared to women aged below 30 years to receive allopathic treatment. The use of allopathic treatment was significantly three times higher among women who were educated (OR = 3.712, p < 0.01) and two times higher among those who were exposed (OR = 2.217, p < 0.5) to media. Further, for those who had felt the treatment was necessary, 30% quoted unaffordability, 44% inaccessibility, and 19% inconveniences as the reasons mentioned for not seeking consult allopathic treatment [10].
Infertility Diagnosis & Management
• For Women: There are several advanced diagnostics to help the couple to understand the underlying cause since a decade in India. The tests include simple blood tests to assess hormone levels, some X-Ray or ultrasound imaging to visualize the uterine cavity or condition of the fallopian tubes, the uterine lining, or sometimes an endoscopy through the cervix to check for potential abnormalities of the uterus. In some cases, an MRI may be used to identify scarring, blockages, or other abnormalities of the uterus, fallopian tubes, or ovaries. A Sono- hysterogram (A saline solution with radiopaque dye is infused into the uterus), and an ultrasound done, which helps to visualize the details of the uterus better.
• For Men: The most common test is semen analysis. It is used to evaluate the quality of sperm, the shape or form of the sperm, or the quantity of the sperms and to assess the motility of sperms. Other tests include assessment of hormonal levels particularly testosterone, and other hormones that impact fertility. Certain genetic tests or testicular biopsy may be undertaken. MRI, ultrasound, help visualizing the sperm duct.
Management of Infertility in Private Sector in India
Infertility management tertiary care facilities are mostly available at state and revenue divisional headquarters both in Private Medical Colleges and IVF Centres. Many surgeries, D&Cs and assisted reproductive technology (ART) which involves procedures like handling human eggs and embryos are being performed. However, despite ICMRs regulations, a few deviations do occur. Female fertility treatment is growing fast. Same is not true for men’s infertility as in most cases the cause of oligospermia is not recognizable. There are some ethical, legal, and societal controversies, for administration of Gonadotropin, transparency in pregnancy data, and addressing cost issues. Based on our case studies consultation and investigation itself would cost about ₹100,000 to 200,000, D&C a common procedure done for women will cost about 50,000. Further treatment will be suggested for Low sperm count, Low egg count, Blocked fallopian tubes, Unexplained infertility, and Endometriosis & other ovulation problems. The lowest rates for some interventions will be Intrauterine insemination (IUI) UI= ₹5,000, IVF - 1 cycle= ₹95,000, IVF - 2 cycle= ₹1,45,000. There are many services listed like IUI - Intrauterine insemination, IVF/ICSI - Invitro fertilization & intra cytoplasmic sperm injection, ERA test -Endometrial receptivity array, PGT- Preimplantation genetic testing, Donor programs (Sperm & egg), Surrogacy services, Fertility enhancing hysteroscopy & laparoscopy surgeries, Ultrasonography – Advanced, Treatment for repeated IVF failures & abortions, Regenerative medicine (Endometrium & Ovarian) and Male infertility, treatment (TESA / PESA). It is difficult for general population and chance of exploitations can’t be ruled out [11].
Management of Infertility in Public Sector in India
The role of the public sector in infertility management is weak as even basic investigations and services are limited or incomplete. Inadequate infrastructure, inappropriate management including time management, lack of information and training, absence of clear protocols at all levels, private practice by public health doctors, pre-occupation with other health issues and lack of regulation are the main problems.
Conclusion
Worldwide about 8–12 % of couple suffer from infertility, with varying rates around the world. The prevalence rate of infertility has increased from 3.5% to 16.7% in more developed nations and from 6.9% to 9.3% in less-developed ones!
The countries with highest infertility among females are North America (16%), Australia & Oceania, Asai 5.87% and Africa 3.18%. The regions with the highest Age-standardised prevalence rates (ASPR) and Age-standardized YLD {(ASYR) YLD=years lived with disability)} for male infertility in 2019 were Western Sub-Saharan Africa, Eastern Europe, and East Asia.
More than 180 million couples in developing countries suffer from primary or secondary infertility, After a fascinating period of more than 40 years of IVF, only a small part of the world population benefits from these new technologies. Time has come to give equitable access to effective and safe infertility care in resource-poor countries, Rural and Poor couples as well!
India has a large population, but population growth has reached below replacement level especially in Urban India and infertility is growing due to various factors. Although reproductive health education and prevention of infertility are top priority, the need for accessible diagnostic procedures & new reproductive technologies is very high.
The success and sustainability of ART in resource-poor settings will depend to a large extend on our ability to optimise these techniques in terms of availability, affordability, and effectiveness which currently are low and affordability in private sector is the beyond the reach of even middle-income families apart for Low Socio-economic families.
Accessible infertility treatment in developing countries depends on socio-cultural & economic prerequisites and will succeed if the Governments support their introduction. Most importantly Infertility remains ignored in Indian population policy and its absence, understood as a technique of reproductive governance.
Infertility Clinicians need to expand service beyond technological interventions, to respond to the psychological and general health ramifications of a diagnosis of oligozoospermia as part of the comprehensive care of men and couples struggling with a diagnosis of infertility.
Sound knowledge about various factors related to infertility, available services and accessibility including the costs in private sector will help health-care providers and policymakers to design and implement various policies.
A realistic and low-cost management, streamlining and regulating services, counselling of couples, providing information and raising awareness of patients, health personnel and policy makers is the need of the time.
References
-
Agiwal V, Madhuri RS, Sirshendu C (2023) Infertility Burden across Indian States: Insights from NFHS 2019– 21. J Reprod Infertility 24(4): 287-292.
-
Sampurna K, Ali B, Dhillon P (2023) Surging trends of infertility and its behavioural determinants in India. PLoS One 18(7): e0289096.
-
Purkayastha N, Sharma H (2021) Prevalence and potential determinants of primary infertility in India: Evidence from Indian demographic health survey. Clinical Epidemiology and Global Health 9: 162-170.
-
Priya S, Kamala S (2010) Reproductive outcome of septate uterus following hysteroscopic septum resection. J Hum Reprod Sci 3(3): 143-145.
-
Human Fatemi (2022) Rising infertility: Detectable, treatable, and preventable. ETHealthWorld.
-
Ashwini K, Saoji AV (2019) Prevalence of Primary Infertility and its Associated Risk Factors in Urban Population of Central India: A Community-Based Cross- Sectional Study. Indian J Community Med. 44(4): 337- 341.
-
Suneeta S (2024) Sunlight Affects Female Fertility? Study Says Moderate Exposure Improves Ovarian Reserve After 30. Healthy Living.
-
Choy JT, Amory JK (2020) Nonsurgical Management of Oligozoospermia. J Clin Endocrinol Metab 105(12): e4194-e4207.
-
(2016) Uterine Septum a guideline. Practice Committee of the American Society for Reproductive Medicine 106(3): 530-540.
-
Shraboni P, Unisa S (2022) An exploration of treatment seeking behaviour of Infertile and need for services in rural India. Front Reprod Health 4: 978085.
-
Indira IVF. Fertility & IVF Centre.
- Capacity Constraints in Pediatric Inpatient Psychiatric Care: A Cross-Sectional Analysis of Bed Availability and Geographic Access in North Carolina
- Why Healthcare Analytics Still Optimizes the Wrong Things
- Coding, Coverage, and Care: The Infrastructure of Transgender Health Inequities
- The Effect of Classroom Attendance on Academic Achievement of Management and Leadership Discipline of Nursing Students at Instituto Superior Cristal and Universidade de Dili, Timor-Leste, 2024: A Case Study
- The Role of Social Bonds in Facilitating Shared Investments and Resource Allocation: Addressing the “Wrong Pocket Problem” in Public Health and Healthcare
- Social-Cultural Factors Contributing to Antimicrobial Resistance in Livestock Farmers and Community Households in Kayonza District, Rwanda