Spectrum of Findings of COVID-19 Associated Pneumonia on Initial Computed Tomography Chest and their association with duration of Hospital Stay and 30 days Mortality
Purpose: Objective of our study is to evaluate the spectrum of pulmonary findings on CT chest in patients with COVID-19 associated pneumonia on initial CT chest and its association with duration of hospital stay and 30 days mortality. Methodology: A retrospective cross sectional study was conducted from 1/1/2021 to 12/11/2021. Patients with positive PCR test were included in our study. CT chest features at initial presentation and CT severity score were evaluated and association was assessed with duration of hospital stay and 30 days mortality. Results: Out of total of 203 confirmed PCR positive bilateral lung involvement was observed in 201(99%) patients? In 145 patients (71.4%) the distribution of disease in axial plane was peripheral. Mean total score of lung severity was 13.04 with 5.332 standard deviation. 51 patients (25.1%) had mild disease, 90(44.3%) had moderate disease and 62(30.5%) had severe disease. 32(15.8%) had ground glass opacities, 151(74.4%) had ground glass opacities and consolidation and 16(7.9%) had consolidations only. Mean of hospital stay was 10.94 days with 8.994 standard deviation. One month mortality was observed in 3 patients with mild disease, 30 patients with moderate disease and 27 patients with severe disease (p<0.001) on initial CT chest. Conclusion: Patients with COVID-19 associated pneumonia have certain typical features on CT chest, knowledge of which can help in rapid screening of such patients. CT severity score can aid in determining the extent and severity of disease. It can be used as a predicting factor for assessing the duration of hospital stay and mortality
Introduction
Novel coronavirus infection emerged as pneumonia of unknown cause from Wuhan city of Hubei province of China [1, 2]. It caused a new type of corona virus named as severe acute respiratory syndrome corona virus 2(SARS-CoV-1) and labelled as COVID-19 by World Health Organization [3]. WHO declared this outbreak as global health emergency on 30th January 2020 [4].
Standard testing for SARS-CoV-2 is Real-time reverse transcription polymerase chain reaction (RT-PCR) [5]. Some patients with COVID-19 infection may not be detected by RT-PCR [6]. Two of the main reasons indicated in literature are inadequate cellular content and improper separation of nucleic acid from clinical material [7]. Also the RT-PCR test might not be readily available in emergency and their results may not be available immediately.
Ai T, et al. in their study showed CT chest to have 97% sensitivity for detecting COVID-19 associated pneumonia. Also they revealed the mean interval between negative RT-PCR test and subsequent positive RT-PCR test to be approximately 5 days [8]. For this reason high resolution CT chest has been indicated as main modality for diagnosis and screening of COVID-19 pneumonia. This is true for patients who have been symptomatic for more than 3 days [9]. Furthermore it is also the main tool for assessment of disease severity [10].
Specific imaging features of COVID-19 associated pneumonia has been observed on chest X-ray and computed tomography (CT) chest [11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22]. Most common presentation of COVID-19 associated pneumonia on CT chest is ground glass haze with right and left lower lobe involvement (40- 83%). Unilateral lung involvement may be manifested in early disease stages of COVID-19 associated pneumonia [23]. A review published by expert panel published in March 2020, most common CT chest finding of COVID-19 associated pneumonia was organizing pneumonia pattern [24, 25]. A study by Shirani et al revealed reverse halo sign (atoll sign) to be reported in many COVID-19 cases. Reverse halo sign is defined as rounded area of ground glass haze surrounded by consolidation [26].
RSNA has proposed four categories for standardized reporting of COVID-19 associated pneumonia [27]. Typical appearances include: Bilateral, peripheral ground glass opacities; associated with/without consolidation or crazy paving pattern. Multifocal ground glass opacities associated with/without consolidation or crazy paving pattern. Atoll sign (reverse halo sign) or organizing pneumonia. Indeterminate appearance include absence of the typical appearances with presence of multifocal, diffuse, unilateral or perihilar ground glass opacities, with/without consolidation that are lacking any specific distribution pattern. Few small ground glass opacities which are not rounded with distribution that is not peripheral. Atypical appearances include absence of the typical or indeterminate features with presence of isolated consolidation in lobar or segmental distribution and absence of ground glass opacities. Other atypical features include pulmonary nodules, lung cavities, and pleural effusion with smooth interlobular septal thickening. Negative for pneumonia means no features of pneumonia on CT chest.
Kwee and Kwee in their publication revealed the CT chest abnormalities with >70% incidence include: ground glass opacity, vascular enlargement, bilateral and lower lobe involvement. The CT chest abnormalities with 10-70% incidence include consolidation, linear opacities, reticulation, crazy paving pattern, air bronchogram, pleural thickening, halo sign, bronchiectasis, nodules, thickening of the bronchial wall and atoll sign. CT chest findings with <10% incidence include central distribution, pleural effusion, pericardial effusion, lung cavity and lymphadenopathy [28]detection of complications, and prognostication of coronavirus disease 2019 (COVID-19. Salehi, et al. mentioned the frequencies of COVID-19 associated CT chest findings as follows: ground glass opacity (88%), consolidation (31.8%), bilateral lung involvement (87.5%) and peripheral distribution (76%) [29]. Early diagnosis of the disease is indispensable for timely management, early patient isolation; thus preventing the spread of this communicable disease. Most studies and reports of CT manifestations of COVID-19 pneumonia are from China followed by European countries. It is not evidently clear if their CT findings of COVID-19 associated pneumonia are similar to findings of our Pakistani population. Thus the objective of our study is to evaluate the spectrum of lung pattern on CT chest in patients with COVID-19 associated pneumonia on initial CT chest. Also we will assess the association of duration of hospital stay and 30 days mortality with initial CT chest findings.
Materials and Methods
A retrospective cross sectional study was conducted from 1/4/2020 to 3/12/2020. Ethical Committee approval was obtained. Patient sampling was consecutive. A total of 203 patients with clinical features of COVID-19 infection and positive PCR test were included in the study. Our inclusion criteria include: 1. Positive RT-PCR for corona virus 2. CT chest showing evidence of COVID-19 associated pneumonia. Patient underwent CT scan chest with 1mm slice thickness using 128 slice multidetector CT scanner. Follow up scans were not analyzed in our study. All CT images were reviewed by at least 2 consultant Radiologists with at least 5 years’ experience. CT chest findings were evaluated for: a. Lobar location b. Distribution (Central- involvement of 2/3rd of lung, predominantly perihilar. Peripheral-involvement of peripheral 1/3rd of lung predominantly subpleural) c. Type of opacity (ground glass opacity(GGO), consolidation) d. Parenchymal bands, reticulations, interlobular septal thickening e. Cavitation f. Pleural effusion g. Mediastenal or hilar lymphadenopathy h. Underlying lung disease i. Others (air bronchogram, pleural thickening, reverse halo, dilated bronchi, and thickened vessels). Involvement of lung was assessed by assigning score to each lobe as follows [30, 31]: Score 0: 0% involvement Score 1: <5% involvement Score 2: 5-25% involvement Score 3: 25-50% involvement Score 4: 50-75% involvement Score 5: >75% involvement Overall involvement of lung parenchyma was provided by adding of each lobe score. Maximum score for bilateral lung involvement was 25. As departmental consensus we assigned score <8 as mild disease, 9-15 as moderate disease and >15 as severe disease. Statistical analysis was done using SPSS version 22.
Results
A total of 203 confirmed PCR positive COVID patients with COVID associated pneumonia on CT chest were included in our study. 152 patients were male (74.9%) and 51 were female (25.1%). Mean age was 56.9 years with standard deviation of 14.1. Highest number of patients were between 51-60 years age range. Bilateral lung involvement was observed in 201(99%) patients. Unilateral right lung involvement was seen in 1 patient (0.5%) and unilateral left lung involvement in 1 patient (0.5%). Right upper lobe was involved in 161 patients, right middle lobe in 183 patients, right lower lobe in 197,left upper lobe in 180, left lower lobe in 197 patients. In 145 patients (71.4%) the distribution of disease in axial plane was peripheral. 58 patients (28.6%) had peripheral and central distribution. Mean total score of lung severity was 13.04 with 5.332 standard deviation. 51 patients (25.1%) had mild disease, 90(44.3%) had moderate disease and 62(30.5%) had severe disease.
203 patients had lung opacities, out of which 32(15.8%) had ground glass opacities, 151(74.4%) had ground glass opacities and consolidation and 16(7.9%) had consolidations only. 45 patients (22.2%) had crazing paving pattern. 135 patients (66.5%) had interlobular septal thickening, 30(14.8%) had air bronchogram. Pleural thickening was seen in 8(3.9%) patients. Traction bronchiectasis was seen in 9(4.4%). 24(11.8%) had purely fibrotic changes. 3 had honey combing (1.5%). 18 patients (8.9%) had pleural effusion. 3 (1.5%) had pneumomediastenum. Reverse halo was observed in only 1 patient (0.5%). Dilated bronchi in 26(12.8%) patients. Thickened vessel was observed in 6 patients (3%). Previous underlying lung disease was observed in some of patients with 1 patient with history of pulmonary tuberculosis, 3 with interstitial lung disease, 1 with asthma and 2 with COPD. Tables1 and Table 2 shows cross tabulation between opacity, crazy paving and disease severity and their chi square values.
| Disease severity | Total | ||||
|---|---|---|---|---|---|
| Mild | moderate | severe | |||
| Opacity | GGO | 15 | 12 | 5 | 32 |
| GGO+consolidation | 26 | 72 | 53 | 151 | |
| Consolidation | 6 | 6 | 4 | 16 | |
| 4 | 0 | 0 | 4 | ||
| Total | 51 | 90 | 62 | 203 |
Table 1: opacity * Disease severity Cross tabulation.
Chi-Square Tests
| Value | Df | Asymp. Sig. (2-sided) | |
|---|---|---|---|
| Pearson Chi-Square | 27.086^{a}$ | 6 | 0 |
| Likelihood Ratio | 25.815 | 6 | 0 |
| Linear-by-Linear Association | 0.605 | 1 | 0.437 |
| N of Valid Cases | 203 |
Table 2: opacity * Disease severity Cross tabulation.
a. 5 cells (41.7%) have expected count less than 5. The minimum expected count is 1.00. Table 1: opacity * Disease severity Cross tabulation.
Count
| Disease severity | Total | ||||
|---|---|---|---|---|---|
| Mild | moderate | severe | |||
| crazy paving | Yes | 1 | 17 | 27 | 45 |
| No | 50 | 73 | 35 | 158 | |
| Total | 51 | 90 | 62 | 203 |
Table 3: crazy paving * Disease severity Cross tabulation.
Chi-Square Tests
| Value | Df | Asymp. Sig. (2-sided) | |
|---|---|---|---|
| Pearson Chi-Square | 29.057^{a}$ | 2 | 0 |
| Likelihood Ratio | 32.794 | 2 | 0 |
| Linear-by-Linear Association | 28.484 | 1 | 0 |
| N of Valid Cases | 203 |
Table 4: crazy paving * Disease severity Cross tabulation.
a. 0 cells (.0%) have expected count less than 5. The minimum expected count is 11.31. Table 2: crazy paving * Disease severity Cross tabulation.
Mean of hospital stay was 10.94 days with 8.994 standard deviation. Minimum period of hospital stay was 0days and maximum period was 40 days. One month mortality was observed in 3 patients with mild disease, 30 patients with moderate disease and 27 patients with severe disease (p<0.001) on initial CT chest. Tables 3-5 shows cross tabulation of hospital stay in days and one month mortality of patients with mild, moderate and severe disease on initial CT and imaging characteristics.
| Disease severity | Total | ||||
|---|---|---|---|---|---|
| Mild | Moderate | Severe | |||
| Hospital stay | not admitted | 31 | 14 | 1 | 46 |
| 1-7days | 15 | 10 | 9 | 34 | |
| 8-14days | 5 | 45 | 8 | 58 | |
| 15-30 days | 0 | 21 | 39 | 60 | |
| >30 days | 0 | 0 | 5 | 5 | |
| Total | 51 | 90 | 62 | 203 |
Table 6: Hospital stay * Disease severity Crosstabulation.
Chi-Square Tests
| Value | Df | Asymp. Sig. (2-sided) | Pearson Chi-Square | 20.175^{a}$ | 2 | 0 | |
|---|---|---|---|---|---|---|---|
| $Pearson Chi-Square | 130.641^{a}$ | $8 | 0 | Likelihood Ratio | 24.16 | 2 | 0 |
| Likelihood Ratio | 139.262 | 8 | 0 | Linear-by-Linear Association | 18.305 | 1 | 0 |
| Linear-by-Linear Association | 88.611 | 1 | 0 | N of Valid Cases | 203 | ||
| N of Valid Cases | 203 |
Table 8: Hospital stay * Disease severity Crosstabulation.
a. 3 cells (20.0%) have expected count less than 5. The minimum expected count is 1.26. Table 3: Hospital stay * Disease severity Crosstabulation.
Count
| Disease severity | Total | one month mortality | Total | |||||
|---|---|---|---|---|---|---|---|---|
| Total | Mild | Total | Moderate | Severe | Yes | No | ||
| Hospital stay | not admitted | 31 | 14 | 1 | 46 | 3 | 48 | 51 |
| Hospital stay | 1-7days | 15 | 10 | 9 | 34 | 30 | 60 | 90 |
| Hospital stay | 8-14days | 5 | 45 | 8 | 58 | 27 | 35 | 62 |
| Hospital stay | 15-30 days | 0 | 21 | 39 | 60 | Total | 60 | 143 |
Table 5: Disease severity * one month mortality Cross tabulation.
Chi-Square Tests
| Value | Df | Asymp. Sig. (2-sided) | |
|---|---|---|---|
| Pearson Chi- Square | 20.175a | 2 | 0 |
| Likelihood Ratio | 24.16 | 2 | 0 |
| Linear-by-Linear Association | 18.305 | 1 | 0 |
| N of Valid Cases | 203 |
Table 7: Disease severity * one month mortality Cross tabulation.
a. 0 cells (.0%) have expected count less than 5. The minimum expected count is 15.07. Table 4: Disease severity * one month mortality Cross tabulation.
| Imaging characteristics | Hospital stay(days) | P value | 1 month mortality | P value | |||||
|---|---|---|---|---|---|---|---|---|---|
| 0 | 7-Jan | 14-Aug | 15-30 | >30 | |||||
| 1. Opacity | GGO | 9 | 9 | 8 | 6 | 0 | 0.17 | 4 | 0.056 |
| GGO+ consolidation | 28 | 25 | 45 | 48 | 5 | 50 | |||
| Consolidation | 5 | 0 | 5 | 6 | 0 | 6 | |||
| 4 | 0 | 0 | 0 | 0 | 0 | ||||
| 2. Crazy paving | 5 | 7 | 12 | 20 | 1 | 0.096 | 15 | 0.325 | |
| 3. Interlobular septal thickening | 22 | 22 | 36 | 51 | 4 | 0.002 | 47 | 0.14 | |
| 4. Air bronchogram | 6 | 3 | 8 | 12 | 1 | 0.641 | 8 | 0.445 | |
| 5. Thickened vessel | 0 | 0 | 3 | 3 | 0 | 0.348 | 1 | 0.427 | |
| 6. Pleural thickening | 1 | 1 | 4 | 2 | 0 | 0.723 | 4 | 0.182 | |
| 7. Pleural effusion | 2 | 4 | 7 | 4 | 1 | 0.497 | 3 | 0.163 | |
| 8. Fibrosis | 8 | 5 | 6 | 5 | 0 | 0.536 | 5 | 0.228 | |
| 9. Reverse halo | 0 | 0 | 0 | 1 | 0 | 0.664 | 0 | 0.704 | |
| 10. Distribution | Peripheral | 45 | 25 | 50 | 25 | 0 | 0 | 33 | 0.001 |
| Peripheral+ central | 1 | 9 | 8 | 35 | 5 | 31 |
Table 9: Imaging characteristics in relation with hospital stay.
Discussion
CT chest is a very useful complementary tool to RT-PCR for the diagnosis of COVID-19 associated pneumonia. The main reason for this being increased sensitivity and rapidity. The typical features of COVID-19 associated pneumonia are ground glass opacities with/without consolidation or crazy paving pattern in bilateral distribution and peripheral predominance [13, 28, 31, 32].
We comprehensively analyzed the spectrum of features of 203 patients of COVID-19 associated pneumonia on CT chest, degree of severity and CT severity score on initial CT chest which will help radiologist and clinicians in understanding CT features to reach accurate and rapid diagnosis. Also we presented our research findings in our 37th Pakistan Annual Radiology Conference. One major limitation of our study is limited sample size.
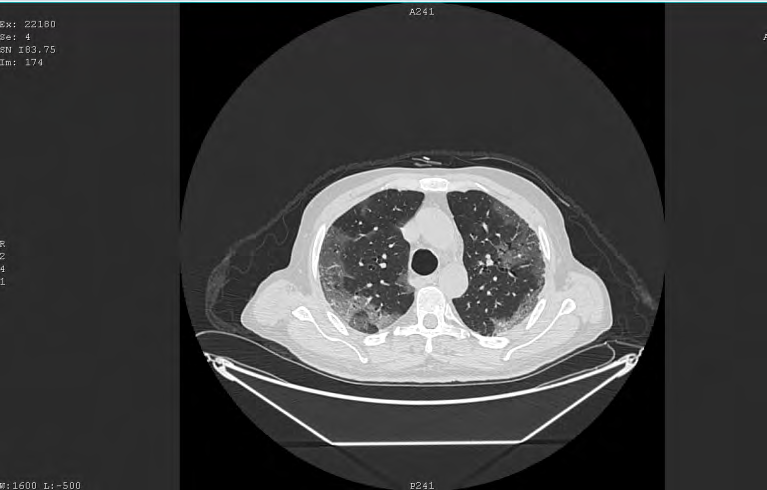
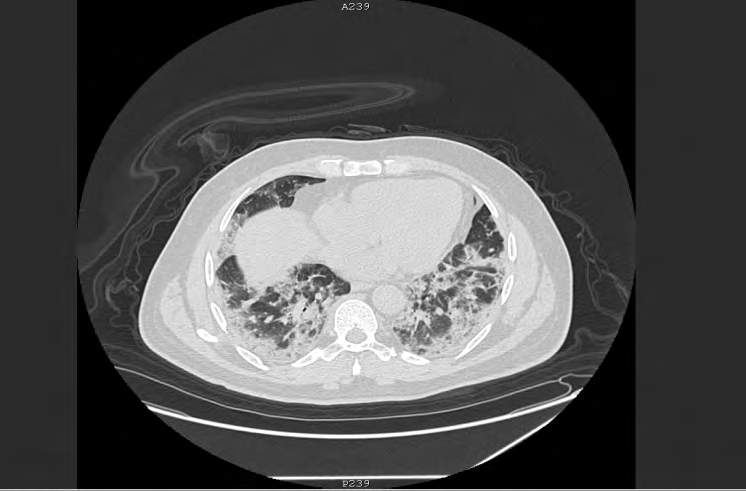
Most of our patients were in the older age group. Majority of patients had bilateral, multiple lobe pulmonary involvement with peripheral predominance. Ground grass opacities with consolidations was the main feature in our patients (Figures 1,2). On cross tabulation between disease severity and hospital stay and 30 days mortality and applying Chi square test our P value was <0.001. This implies that disease severity on basis of CT score can be a predictor of duration of hospital stay and one month mortality. A strength of this study is that we relied on CT chest findings for assessing the patients stay in hospital and one month mortality. Our results (p <0.001) suggested that triage with chest CT can be a very useful tool for COVID-19 patients.
Ahlstrand E, et al. in their study on role of visual scoring of CT chest at hospital admission in predicting hospitalization and ICU admission in COVID-19 patients revealed CT severity score and age as significant predictors for ICU admission and mortality [33]. Our study showed male predominance with 74% male and 25.4% female. This
was similar to study by Xiang C, et al. [34]. Other studies show no such gender predominance [31, 35]. One possible reason for this may be our limited sample size. 99% of our patients showed bilateral lung involvement with peripheral distribution in 72% patients. Chung, et al. and Shi, et al. [31] China. We aimed to describe the CT findings across different timepoints throughout the disease course. Methods: Patients with COVID-19 pneumonia (confirmed by next-generation sequencing or RT-PCR reported bilateral distribution in 88.9% and 79% patients respectively [31, 36]. The later study showed peripheral distribution in 54% of patients. Possible cause of bilateral lung involvement may be high viral load. The cause for peripheral predominance appear to be the ability of the virus to reach deep into the terminal bronchioles and alveolar spaces [37]such as severe acute respiratory syndrome coronavirus (SARS-CoV. Multiple lobes and multiple segments were commonly involved in our study. The lower lobes were more commonly involved with right and left lower lobe involvement in 95% of our patients. Xiang C, et al. reported multiple lobe involvement with lower lobe predominance. The lower lobe bronchi being relatively straight makes it easy for the virus to reach the lower lobe and affect them [31].
Ground glass opacity with consolidation was found in 72.2% of our patients, isolated consolidation was seen 7.7% of patients only. Other features included crazy paving, interlobular septal thickening, air bronchogram, dilated bronchi and thickened vessels. Similar CT chest findings were observed in study by Xiang C, et al. Ding X, et al. and Yu M, et al. [37, 38, 39]. Such CT chest features were appreciated in MERS and SARS [40]. Pleural effusion appeared in 8.6% of our patients which could be related to the infection or fluid over load. Very few of our patients showed pneumomediastenum which is likely iatrogenic secondary to intubation. In a case control study by S.M.H. Tabatabaei, et al. pleural effusion was observed in 40% of patients on CT chest of COVID-19 patients that expired and 3.3% of patients that were discharged [41].
Interestingly we found in our study that 11.2% of our patients showed purely fibrotic changes in the initial CT chest with 1.5% patients showing honey combing. This percentage is higher and in contradiction to typical lung findings seen in other studies. Further studies need to be carried out on to identify its cause. Also local study needs to be carried out on larger population with assessment of disease progression on CT chest.
Conclusion
Knowledge of typical CT chest findings can help in rapid screening of suspected patients of COVID-19 associated pneumonia. Ground glass opacity with or without consolidation with bilateral lung involvement are the main characteristics of the disease. Disease severity assessment is very important part of CT report of COVID-19 patients as it can be an indicator for clinicians to timely change the course of management for COVID-19 patients. It can be used as a predicting factor for duration of hospital stay and one month mortality.
References
-
Zhu N, Zhang D, Wang W, Li X, Yang B, et al. (2020) A Novel Coronavirus from Patients with Pneumonia in China, 2019. N Engl J Med 382(8): 727-733.
-
Huang C, Wang Y, Li X, Ren L, Zhao J, et al. (2020) Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 395(10223): 497-506.
-
WHO (2020) Coronavirus Disease (COVID-19) outbreak.
-
Mahase E (2020) China coronavirus: WHO declares international emergency as death toll exceeds 200. BMJ 368: m408.
-
(2020) Global surveillance for COVID-19 caused by human infection with COVID-19 virus: interim guidance 2 Probable case.
-
Ye G, Li Y, Lu M, Chen S, Luo Y, et al. (2020) Experience of different upper respiratory tract sampling strategies for detection of COVID-19. Journal of Hospital Infection 105(1): 1-2.
-
Shigemura J, Ursano RJ, Morganstein JC, Kurosawa M, Benedek DM (2020) Public responses to the novel 2019 coronavirus (2019-nCoV) in Japan: Mental health consequences and target populations. Psychiatry and Clinical Neurosciences 74(4): 281-282.
-
Ai T, Yang Z, Hou H, Zhan C, Chen C, et al. (2020) Correlation of Chest CT and RT-PCR Testing in Coronavirus Disease 2019 (COVID-19) in China: A Report of 1014 Cases. Radiology 296(2).
-
Fang Y, Zhang H, Xie J, Lin M, Ying L, et al. (2020) Sensitivity of Chest CT for COVID-19: Comparison to RT- PCR. Radiology 296(2): E115-E117.
-
Pan Y, Guan H, Zhou S, Wang Y, Li Q, et al. (2020) Initial CT findings and temporal changes in patients with the novel coronavirus pneumonia (2019-nCoV): a study of 63 patients in Wuhan, China. Eur Radiol 30(6): 3306- 3309.
-
Phelan AL, Katz R, Gostin LO (2020) The Novel Coronavirus Originating in Wuhan, China: Challenges for Global Health Governance. JAMA 323(8): 709-710.
-
Nishiura H, Jung SM, Linton NM, Kinoshita R, Yang Y, et al. (2020) The Extent of Transmission of Novel Coronavirus in Wuhan, China, 2020. J Clin Med 9(2): 330.
-
Pan F, Ye T, Sun P, Gui S, Liang B, et al. (2020) Time Course of Lung Changes at Chest CT during Recovery from Coronavirus Disease 2019 (COVID-19). Radiology 295(3): 715-721.
-
Xie X, Zhong Z, Zhao W, Zheng C, Wang F, et al. (2020) Chest CT for Typical Coronavirus Disease 2019 (COVID-19) Pneumonia: Relationship to Negative RT- PCR Testing. Radiology 296(2): E41-E45.
-
Fang Y, Zhang H, Xu Y, Xie J, Pang P, et al. (2020) CT Manifestations of Two Cases of 2019 Novel Coronavirus (2019-nCoV) Pneumonia. Radiology 295(1): 208-209.
-
Song F, Shi N, Shan F, Zhang Z, Shen J, et al. (2020) Emerging 2019 Novel Coronavirus (2019-nCoV) Pneumonia. Radiology 295(1): 210-217.
-
Ng MY, Lee EYP, Yang J, Yang F, Li X, et al. (2020) Imaging profile of the covid-19 infection: Radiologic findings and literature review. Radiol Cardiothorac Imaging 2(1).
-
Kong W, Agarwal PP (2020) Chest imaging appearance of covid-19 infection. Radiol Cardiothorac Imaging 2(1).
-
Kay FU, Abbara S (2020) The Many Faces of COVID-19: Spectrum of Imaging Manifestations 2(1).
-
Wu Y, Xie YL, Wang X (2020) Longitudinal CT findings in covid-19 pneumonia: Case presenting organizing pneumonia pattern. Radiol Cardiothorac Imaging 2(1).
-
Liu T, Huang P, Liu H, Huang L, Lei M, et al. (2020) Spectrum of Chest CT Findings in a Familial Cluster of COVID-19 Infection. Radiol Cardiothorac imaging 2(1).
-
Li X, Zeng X, Liu B, Yu Y (2020) Covid-19 infection presenting with CT halo sign. Radiol Cardiothorac Imaging 2(1): e200026.
-
Bayraktaroğlu S, Çinkooğlu A, Ceylan N, Savaş R (2021) The novel coronavirus pneumonia (COVID-19): a pictorial review of chest CT features. Diagn Interv Radiol 27(2): 188-194.
-
Kory P, Kanne JP (2020) SARS-CoV-2 organising pneumonia: ‘Has there been a widespread failure to identify and treat this prevalent condition in COVID-19?. BMJ open Respir Res 7(1).
-
Kanne JP, Little BP, Chung JH, Elicker BM, Ketai LH (2020) Essentials for Radiologists on COVID-19: An Update- Radiology Scientific Expert Panel. Radiology 296(2): E113-E114.
-
Shirani F, Shayganfar A, Hajiahmadi S (2021) COVID-19 pneumonia: a pictorial review of CT findings and differential diagnosis. Egypt J Radiol Nucl Med 52(1): 1-8.
-
Simpson S, Kay FU, Abbara S, Bhalla S, Chung JH, et al. (2020) Radiological Society of North America Expert Consensus Statement on Reporting Chest CT Findings Related to COVID-19. Endorsed by the Society of Thoracic Radiology, the American College of Radiology, and RSNA - Secondary Publication. J Thorac Imaging 35(4): 219- 227.
-
Kwee TC, Kwee RM (2020) Chest CT in COVID-19: What the Radiologist Needs to Know. Radiographics 40(7): 1848-1865.
-
Salehi S, Abedi A, Balakrishnan S Gholamrezanezhad A (2020) Coronavirus Disease 2019 (COVID-19): A Systematic Review of Imaging Findings in 919 Patients. AJR Am J Roentgenol 215(1): 87-93.
-
Chang YC, Yu CJ, Chang SC, Galvin JR, Liu HM, et al. (2005) Pulmonary sequelae in convalescent patients after severe acute respiratory syndrome: evaluation with thin-section CT. Radiology 236(3): 1067-1075.
-
Shi H, Han X, Jiang N, Cao Y, Alwalid S, et al. (2020) Radiological findings from 81 patients with COVID-19 pneumonia in Wuhan, China: a descriptive study. Lancet Infect Dis 20(4): 425-434.
-
Guillo E, Gomez IB, Dangeard S, Bennani S, Saab I, et al. (2020) COVID-19 pneumonia: Diagnostic and prognostic role of CT based on a retrospective analysis of 214 consecutive patients from Paris, France. Eur J Radiol 131: 109209.
-
Ahlstrand E, Cajander S, Cajander P, Ingberg E, Löf E, et al. (2021) Visual scoring of chest CT at hospital admission predicts hospitalization time and intensive care admission in Covid-19. Infect Dis (London) 53(8): 622-632.
-
Xiang C, Lu J, Zhou J, Guan L, Yang C, et al. (2020) CT Findings in a Novel Coronavirus Disease (COVID-19) Pneumonia at Initial Presentation. Biomed Res Int 2020.
-
Bernheim A, Mei X, Huang M, Yang Y, Fayad ZA, et al. (2020) Chest CT findings in coronavirus disease 2019 (COVID-19): Relationship to duration of infection. Radiology 295(3): 685-691.
-
Chung M, Bernheim A, Mei X, Zhang N, Huang M, et al. (2020) CT Imaging Features of 2019 Novel Coronavirus (2019-nCoV). Radiology 295(1): 202-207.
-
Liu L, Wei Q, Lin Q, Fang J, Wang H, et al. (2019) Anti- spike IgG causes severe acute lung injury by skewing macrophage responses during acute SARS-CoV infection. JCI insight 4(4): e123158.
-
Ding X, Xu J, Zhou J, Long Q (2020) Chest CT findings of COVID-19 pneumonia by duration of symptoms. Eur J Radiol 127: 109009.
-
Yu M, Xu D, Lan L, Tu M, Liao R, et al. (2020) Thin-section chest CT imaging of covid-19 pneumonia: A comparison between patients with mild and severe disease. Radiol Cardiothorac Imaging 2(2).
-
Tse GMK, To KF, Chan PKS, Lo AWI, Ng KC, et al. (2004) Pulmonary pathological features in coronavirus associated severe acute respiratory syndrome (SARS). J Clin Pathol 57(3): 260-265.
-
Tabatabaei SMH, Rahimi H, Moghaddas F, Rajebi H (2020) Predictive value of CT in the short-term mortality of Coronavirus Disease 2019 (COVID-19) pneumonia in nonelderly patients: A case-control study. Eur J Radiol 132: 109298.
- Psychogenic Erectile Dysfunction in Late Adulthood: A Case Report on Clinical Intervention and Intimacy Restoration
- Clinical Trials on COVID-19 in 2025: A New Chapter in Global Health Research
- Innovations and Challenges in Contemporary Medical Clinical Trials: An Editorial Perspective
- Innovations and Challenges in Contemporary Medical Clinical Trials: A Critical Perspective
- Reimagining Clinical Trials: The Power of Continuous Feedback from Medical Reports
- Factors Influencing Brain Drain: Perspectives from a Medical School in Turkey