Single Ventricle Physiology with Double Outlet and TGA: 3D Cardiac MDCT as a Picture-Perfect Diagnostic Modality
Single ventricle physiology is a cyanotic congenital heart disease that may require intensive medical management after birth. Multidetector computed tomography (MDCT) has recently expanded as advanced imaging modality for structural heart disease imaging. The 3-dimentional reconstruction of cardiac anatomy is cornerstone in diagnosis of congenital heart diseases which is limited in other imaging modalities like echocardiography and cardiac magnetic resonance (CMR). More recently, survival was estimated to be only 30% for the first year of life [1]. Survival into late adulthood is exceptional. We are presenting an exceptional case of univentricular physiology in an adult patient.
Case Report
A 24-yr old male patient presented with easy fatiguability and aggravated dyspnea on exertion over past one month. Echocardiography reveals severe pulmonary hypertension with poor right ventricular filling. Also, arteriovenous connections were not delineated correctly. To determine the complete structural depiction, cardiac MDCT with contrast was performed. The right ventricular cavity was rudimentary with poor contrast filling (Figure 1A). Interestingly right atrial outlet was connected to left ventricle (Figure 1B). Cross-sectional imaging of mid-ventricle revealed single cavity suggestive of dominant left ventricle (Figures 1C & 2D). Left atrium outlet was connected normally to left ventricle via mitral valve (Figure 1D). Simultaneous contrast filling of RV & LV is suggestive of single ventricle with dominant LV and rudimentary RV (Figures 1D, E, F). However, right atrial outlet appears connected to left ventricle as well and a very limited connection to possible false right ventricular cavity which is shown as a circling contrast jet to LV (Figures 1D, E, F & 2C). This confirms the diagnosis of single ventricle physiology with double-inlet ventricle.
Furthermore, 3D analysis of arterial connections reveals severely dilated main pulmonary trunk including right and left branches (Figure 2A). Surprisingly, ascending aorta was positioned anterior and rightward to pulmonary trunk suggestive of discordant major arterial connection as transposition of great arteries (TGA) (Figure 2B). This is a rate anomaly of TGA with double outlet ventricle. Overall, this is an extremely rate case of univentricular physiology with double inlet and double outlet ventricle with TGA. Till date, such rare case has not been found in literature.
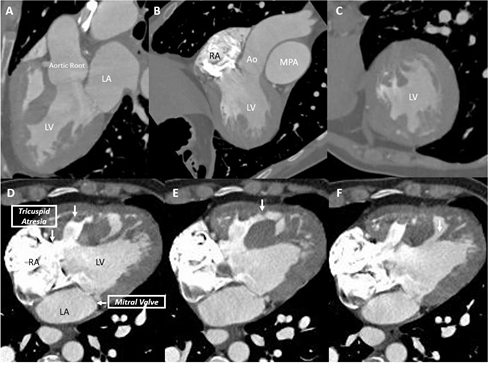
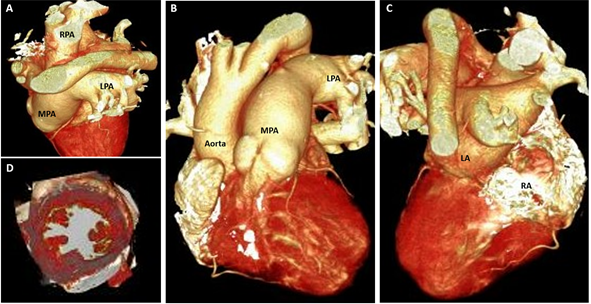
Figure 2: A) Grossly dilated MPA, LPA & RPA; B) Discordant major arterial connection with anterior and rightward position of aorta in relation to MPA; C) Left and right atrium connected to one ventricle; D) Cross-sectional image reveals single ventricle cavity. Abbreviations: LV Left Ventricle; RA Right Atrium; LA Left Atrium; MPA Main Pulmonary Artery; RPA Right Pulmonary Artery; LPA Left Pulmonary Artery; Ao Aorta.
Discussion
This case represents a case of single ventricle physiology as functional single ventricle (FSV) with 1:1 connection with hypoplastic RV [2]. FSV patients are living for decades before frequent imaging evaluation for preprocedural planning. Survival to adulthood is exceptional. Only about 30% of patients with single ventricle physiology survive till the age of 16 years [1].
The unbalanced atrioventricular canal represents approximately 10% of atrioventricular canal defects [3]. The ventricle that is partially excluded from the common atrioventricular valves (AVV) is often hypoplastic, which can result in single ventricle physiology [4]. The types of surgeries vary depending upon the clinical condition and it includes Blalock-Taussig Shunt (subclavian artery to pulmonary trunk), Glenn procedure (superior vena cava to pulmonary trunk), Fontal procedure (inferior vena cava to pulmonary trunk), Hybrid procedures and heart transplantation.
Advanced imaging is cornerstone in accurate and serial analysis of FSV patients. Echocardiography is insufficient for evaluation of the thoracic vasculature or for reproducible estimation of ventricular function [5]. Cardiovascular MRI is an emerging modality for these indications, but it requires relatively long imaging times which requires deep sedation, or anesthesia in young children. Many older patients have metallic implants with an artefact that degrades MRI quality [6]. In addition, it is relatively contraindicated in those with pacemakers and defibrillators as these devices have been known to cause an imaging artefact [7]. CT offers high-resolution anatomic detail that the surgeon can utilize for procedural planning, serving as a complement to the robust functional information gained from echocardiography. The main limitation of CT is exposure to ionizing radiation, which should be considered when imaging the relatively young population of patients with FSV, particularly since they may undergo multiple serial imaging examinations [8]. Image quality remains good at low radiation exposure, and accuracy is excellent when compared with interventional findings [9].
Conclusion
Diagnostic utility of low-radiation MDCT in cardiology has increased over past decade beyond coronary analysis. This case represents that cardiac CT represents the picture- perfect application of cardiac CT in highly complex congenital heart diseases. Only such analysis can guide to a treatment strategy with high prospect of favorable outcome. Future work should be directed towards low-radiation applications of 3D MDCT in pediatric population for early diagnosis and treatment planning that can improve the survival rate as well as quality of life in these patient populations.
References
-
Hager A, Kaemmerer H, Eicken A, Fratz S, Hess J (2002) Long-term survival of patients with univentricular heart not treated surgically. J Thorac Cardiovasc Surg 123(6): 1214-1217.
-
Wilkinson JL, Anderson RH (2012) Anatomy of functionally single ventricle. World J Pediatr Congenit Heart Surg 3(2): 159-164.
-
Foker JE, Berry JM, Vinocur JM, Harvey BA, Pyles LA (2013) Two-ventricle repairs in the unbalanced atrioventricular canal defect spectrum with midterm follow-up. J Thorac Cardiovasc Surg 146(4): 854-860.e3.
-
Cohen MS, Jegatheeswaran A, Baffa JM, Gremmels DB, Overman DM, et al. (2013) Echocardiographic features defining right dominant unbalanced atrioventricular septal defect: a multi-institutional congenital heart Surgeons’ Society study. Circ Cardiovasc Imaging 6(4): 508-513.
-
Han BK, Huntley M, Overman D, Witt D, Dassenko D, et al. (2018) Cardiovascular CT for evaluation of single- ventricle heart disease: risks and accuracy compared with interventional findings. Cardiol Young 28(1): 9-20.
-
Garg R, Powell AJ, Sena L, Marshall AC, Geva T (2005) Effects of metallic implants on magnetic resonance imaging evaluation of Fontan palliation. Am J Cardiol 95(5): 688-691.
-
Cronin EM, Mahon N, Wilkoff BL (2012) MRI in patients with cardiac implantable electronic devices. Expert Rev Med Devices 9(2): 139-146.
-
Orwat S, Diller GP, Baumgartner H (2014) Imaging of congenital heart disease in adults: choice of modalities. Eur Heart J Cardiovasc Imaging 15(1): 6-17.
-
Edwards RM, Reddy GP, Kicska G (2016) The functional single ventricle: how imaging guides treatment. Clin Imaging 40(6): 1146-1155.
- Psychogenic Erectile Dysfunction in Late Adulthood: A Case Report on Clinical Intervention and Intimacy Restoration
- Clinical Trials on COVID-19 in 2025: A New Chapter in Global Health Research
- Innovations and Challenges in Contemporary Medical Clinical Trials: An Editorial Perspective
- Innovations and Challenges in Contemporary Medical Clinical Trials: A Critical Perspective
- Reimagining Clinical Trials: The Power of Continuous Feedback from Medical Reports
- Factors Influencing Brain Drain: Perspectives from a Medical School in Turkey