Attitude and Behavior of Emerging Novel COVID-19 Disease Khartoum, Sudan
Background: The emerging COVID-19 is a devastating life-threatening disease, which is characterized by high morbidity. More than 40 million people have been affected globally with case fatality rate ranging between 5 – 10%. Attitude and behavior play a major role in preventing the emerging and re-emerging diseases. Our study aimed at assessing attitude and behavior of participants towards COVID-19. Methods: This is a descriptive cross-sectional community-based study. It was carried out in Khartoum States (Khartoum, Bahri and Omdurman localities). A total of 1200 participants were randomly interviewed face-to-face using close ended questionnaire. A multistage cluster sampling technique was applied. Statistical Package for Social Science (SPSS) Smart PLS were used. Logistic regression, factor analysis and tree analysis were performed. Results: Negative attitude was reported in greater that half of participants [(52.7%, n= 632, ] (95%Cl, 49.9% - 55.5%), whilst positive attitude was noted in [(47.3%, n= 568, (95%Cl, 44.5% - 50.1%)]. Regarding behavior, more than half of the participants [(55.3%, n= 663, (95%Cl, 52.5% - 58.1%)] had poor behavior, whereas the remaining [(44.7%, n= 537, (95%Cl, 41.9% - 47.5%)] had good behavior. Factor analysis revealed that, three factors extracted which explain 56% of change occurring attitude towards COVID-19 of the surveyed participants they were recorded into; misconceptions about covid19, infodemics of COVID19, and negative stereotyping. The spectrum of behavior was noted in; response to isolation strategy, anticipated stigma, and enacted stigma (61%). Logistic regression showed that, monthly income between 2000-2999 SDG was 2.25 times more likely to have negative attitudes towards COVID19 ( β = 0.809 , p <0.001, AOR=2.25, 95% C.I.; 1.48 -3.41,). Educational status was statistically associated with attitude towards COVID19 ( p <0.001). Males were 0.62 less likely to have poor behavior comparing with females ( β = −0.48 , p <0.05, AOR=0.62, 95% C.I.; 0.43 -0.89). Monthly income 2000-2999 SDG was 2.83 times more likely to have poor behavior towards COVID19 ( β = 1.04 , p <0.001, AOR=2.83, 95% C.I.; 1.77 -4.52). Tree analysis revealed that attitude was the best predictor of behavior towards COVID-19. Locality was the best predictor of negative attitude. Conclusion: Behavior and attitude combined have a potential effect on preventing and controlling COVID-19.
Background
On December 8, 2019, the first identified case of Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) was officially reported in Wuhan, China [1]. However, the emerging disease has become a global health emergency, and was declared by World Health Organization (WHO) in January 2020 [2].
The whole world is now facing a catastrophic massive burden from the COVID-19 pandemic. Coronaviruses have varied symptoms ranged from mild to more per acute illnesses such as SARS and MERS [3]. These symptoms of the COVID19 infection include fever, headache, cough, sore throat, nausea and vomiting, diarrhea, dermatological lesions. The vulnerability of the COV increases with underlying chronic illnesses diabetes Millets and hypertension are more likely to be infected with COV and would experience worsen conditions [4] like heart, and respiratory failure, acute respiratory syndrome, or even death [5].
Many countries have taken extraordinary precautionary measures to curb the spread of the COVID19. However, these severe restrictions; locking down, hand washing, contact avoidance, wearing masks, keeping social distance, travel restrictions, and avoiding crowded places would minimize the risk of infection. The COVID19 has led to health crisis which has resulted in many countries to opt for social quarantine of their populations, communication systems have been characterized by disintermediation, the acceleration of digitization and an infodemic.
Since COVID19 is a behavioral disease many ministries of health should be displayed awareness of protective behaviors against COVID19 and develop health-protective attitudes during a health crisis. Further, behavior and attitude will definitely have direct impact on prevention measures. Thereby, these steps would help individuals to take meaningful steps to protect themselves. Healthy behavior and attitude are also crucial in keeping healthy during the coronavirus pandemic [6].
An attitude is a psychological state of mind. It is the way a person thinks about situations, and it ultimately determines a person’s behavior. It also refers to inclinations to react in a certain way to certain situations. Moreover, behavior is defined by the actions of a person based on specific stimuli. It refers to our opinions, beliefs, and feelings about aspects of our environment [7, 8]. Psychological factors are called internal factors, while social factors are called external factors. These factors interact together whether psychological factors with social factors, and this interaction results in the behavior of the individual, which is maybe positive or negative behavior [9].
In addition, the direct impact of behavior and attitude of COVID 19 on of those infected is also significant, and is often precipitated due to increased stigma, social isolation and quarantine. Thus the social isolation and movement restrictions due to COV also jeopardize health and access to basic needs, and point to the need for human rights, which resulted in many deaths whether by corona virus or other causes [10].
In Sudan on 13th March, the first reported case of coronavirus was confirmed in Khartoum, a man who was visiting United Arab Emirate in the first week of March, and by 27 of May, a surge of reported cases and death was reached with no of 4521 case and 233 deaths. Therefore, the Federal Ministry of Health Sudan (MoH) has made ongoing campaigns of awareness concerning mode of transmission and the importance of applying protective measures, quarantine and curfew. Although strict measures taken, the awareness of individuals towards infectious viruses remains the most important factor in controlling and containment of the COVID19 [11].
However, during the current outbreak misleading information for example; rumours and myth particularly on social media were shared widely, fear and anxiety were apparently manifested and stigmatization was appeared to be prevailed [12]. Furthermore, some individuals’ fear of being diagnosed and/or categorized as suspected case, thus this situation created psychosocial dilemma of accessing health care to know their status. Moreover, another mark of the fear is that Sudan MoH announced that more than 50% of those who returned to their home during the outbreak were pledged incorrect information at airport check to deceive the health workers of being investigated and screened [13].
The ongoing outbreak, propaganda, fear, stigma and discrimination, besides the fragility health system worsen the situation and created an appropriate pathway for triggering COVID19 distribution. Thus, this study attempted to highlight the importance of attitude and behavior of Sudanese participants in bridging gaps of controlling the COVID-19. This study will potentially help policy makers in implementing comprehensive interventional campaigns.
Methods
The aim of the current study is to determine behavior and attitude of participants towards COVID-19 in Khartoum. This is a cross sectional community based study. It was carried out in Khartoum the capital of Sudan, which encompasses three localities; Khartoum, Bahri and Omdurman. A multistage random sampling was applied. A number of 1200 participants were enrolled randomly. A total of 400 participants were recruited from each locality, whilst half of those were drawn from central and the remaining from peripheral sites. The sample size was calculated based on the assumption that the probability of having positive attitude towards preventive measures against COVID19 disease was 50.0%, at 95% confidence interval, limit of precision of 5%, with a design effect of 1.0, the calculated sample size was 384 participants and 5% were added as contingents [14]. Participants were answered a yes-no question to confirm their willingness to participate voluntarily. Participants were inquired about (i) Socio-demographic information, (ii) Attitude concerning COVID-19 (iii) protective measures (iv) behaviors to prevent COVID-19 (v) types of information. However, all participants were directed to complete the self-report survey.
Statistical Analysis
Descriptive statistical methods were used to summarize data on socio-demographic profile and responses to questions concerning attitude and behavior towards COVID-19. Data were displayed as frequencies and percentages (%) for categorical variables. Data were analyzed using Statistical Package for the Social Sciences (SPSS, version 25; IBM, USA), and Smart PLS 3.3.2 version. A P value was considered statistically significant at level of P < 0.05. All baseline socio- demographics were described as categorical variables_._ Multivariable logistic analysis, with Odds Ratios (OR) reported, were used to determine factors associated with preventive behavior of COVID-19. Participants’ attitudes and behavior were categorized into two categories: poor and good. For attitudes, the median was of the scores was 33,
Overall Attitude and Behavior
while for behavior it was 36. Both of two values considered as cut-off points when categorizing attitudes and behavior. The moderating and mediating effects are used to explain the relationship between attitude and behavior. More, tree analysis was also applied.
Results
Two constructs namely attitudes and behavior towards COVID 19 of the sampled members (n=1200) were tested for reliability. The domain of attitudes scored good reliability, since Cronbach Alpha coefficient was between 0.7 to 0.79 while the domain of behavior scored a very good reliability, since Cronbach Alpha coefficient was between 0.8 to 0.89 (source), and hence our instrument developed was valid and reliable.
Gender ratio in favor of females since (60.9%, n=731) were females. Majority of the participants (48.8%, n=585) were between 20 to 29 years at the time of data collection, However, 11.2% (N=134) of the participants were 50 years or above at the time of survey. While only 42 (3.5%) participants were uneducated, and (56.6%, n= 679) had bachelor/diploma certificate. With regard to marital status, majority of the surveyed persons were singles (55.5%, n= 666. Up to 668 participants (55.7%) reported that their families had between 4 to 6 members. Moreover, employed are (57.7%, n=693). Of the 693 participants who were employed closed to 40% of them work in private sector (39.4%, n= 273), regarding monthly income level greater than a half of the participants (51.2%, n=614) earned 3000 SDG or more a month.
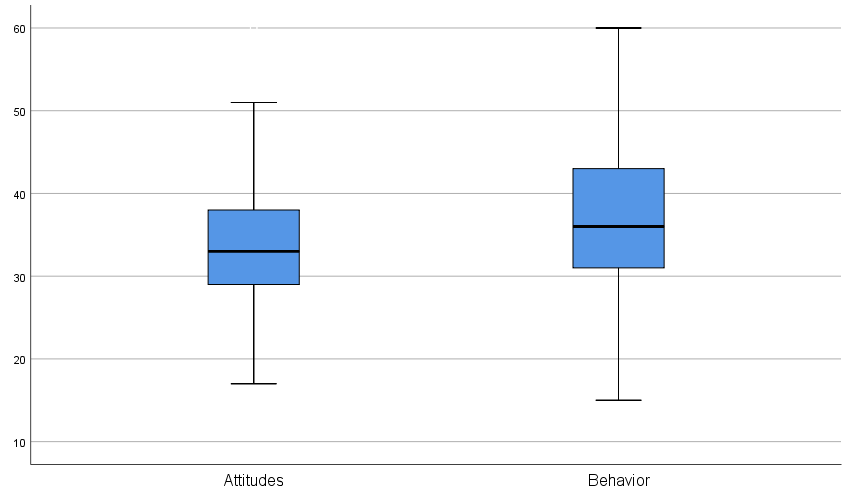
When attitudes towards COVID 19 categorized, (median 33) greater than the half of the participants (52.7%, n= 632) had negative attitudes (95%Cl, 49.9% - 55.5%), while 47.3% of them had positive attitudes (95%Cl, 45.9% - 50.1%). Regarding behavior (median 36), greater than the half of the participants (55.3%, n= 663) had poor behavior (95%Cl, 52.5% - 58.1%), while 44.7% of them had good behavior (95%Cl, 41.9% - 47.5%).
Factor Analysis for Attitudes and Behavior towards COVID 19
Factor analysis for attitude and behavior towards COVID19 revealed that the Kaiser –Meyer-Olkin Measure of sampling adequacy was 0.857, therefore, this value considered statistically good according to Kaiser’s classifications, and Bartlett’s test was significant (p value < 0.001) Three factors were extracted which explain 56% of change occurring attitudes towards COVID 19 of the surveyed participants. They were Misconceptions about covid19, infodemics of COVID19, and negative stereotyping. In addition, there were three factors extracted for behavior and explain 61% of change occurring behavior towards COVID19 of the surveyed participants. They were Response to isolation strategy, anticipated stigma, and enacted stigma.
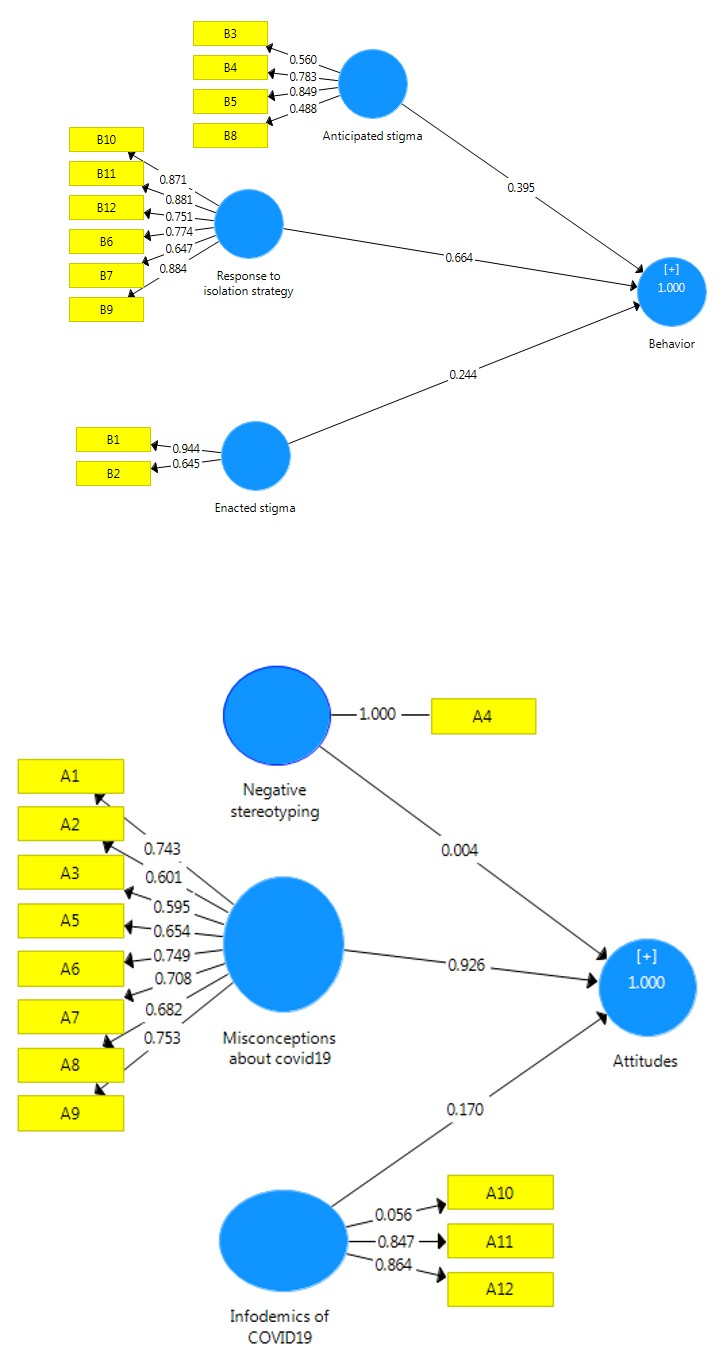
Figure 2a: Factors describe Attitudes.
Figure 2b: Factors describe Behaviors.
As Figure 2a and 2b shows misconceptions about COVID
19 and infodemics of COVID19 statistically describe person’s
attitudes positively ( left ) and (
$$ (\beta = 0. 9 2 6, p - v a l u e < 0. 0 0 1) $$
respectively. However, negative stereotyping showed no role
in describing attitudes of the members towards COVID 19 $$ (\beta = 0. 0 0 4, p - v a l u e > 0. $$
. The Confirmatory factor analysis
(CFA) ran using SmartPls 3.0 indicated that three factors
statistically describe the behavior of the participants
positively (Right). These three factors were response to
isolation strategy ( 0.664, 0.001) p value β = − < , anticipated stigma ( 0.395, 0.001) p value β = − <
, and enacted stigma
$$ (\beta = 0. 2 4 4, p - v a l u e < 0. 0 0 1). $$
Main Channel of Information
Most of the participants (81.7%, n=980) indicated that they heard about COVID19 from the television and this choice represents the mode of the participants’ selections with (26.9%) of the total responses. Breakdown of the responses indicated that social media exposure represents 22.7% of the total responses (68.9% of cases). Since we have 3640 and 1200 participants, so each participant did tick at least three sources of information about the COVID19.
| Sources | Responses | Percent of Cases | |
|---|---|---|---|
| N | Percent | ||
| Friends | 643 | 17.7% | 53.6% |
| Family | 631 | 17.3% | 52.6% |
| Radio | 341 | 9.4% | 28.4% |
| Television | 980 | 26.9% | 81.7% |
| Social media | 827 | 22.7% | 68.9% |
| Doctor | 191 | 5.2% | 15.9% |
| Other/select | 27 | 0.7% | 2.3% |
| Total | 3640 | 100.0% | 303.3% |
Table 1: Source of information about the COVID19.
Bivariate Analysis of Attitude and Behavior towards COVID19
| Characteristic (N = 1200) | Dependent variable: Attitudes towards COVID19 | Dependent variable: Behavior towards COVID19 | ||||
|---|---|---|---|---|---|---|
| Chi-square | DF | p value | Chi-square | DF | p value | |
| Locality | 21.5 | 2 | 0.000 | 37.6 | 2 | 0.000 |
| Gender | 5.6 | 1 | 0.018 | 1.2 | 1 | 0.278 |
| Age | 125.7 | 4 | 0.000 | 94.5 | 4 | 0.000 |
| Work status | 2.7 | 1 | 0.101 | 0.1 | 1 | 0.803 |
| Sector | 14.4 | 2 | 0.001 | 7.5 | 2 | 0.024 |
| Monthly income | 36.9 | 3 | 0.000 | 42.5 | 3 | 0.000 |
| Educational level | 124.8 | 4 | 0.000 | 62.4 | 4 | 0.000 |
| Marital status | 97.2 | 3 | 0.000 | 78.1 | 3 | 0.000 |
| Number of family members | 97.2 | 3 | 0.000 | 10.2 | 2 | 0.006 |
| Attitudes | NA | NA | NA | 210.0 | 1 | 0.000 |
Table 2: Chi-square Test results.
In the bivariate analysis, using the chi-squared and Fischer’s exact tests as Table 2 below presents, while work status had no significant association with attitudes and behavior towards COVID19 (p value > 0.10), gender statistically associated with attitudes towards COVID19 $$ \left(\chi^ {2} = 5. 6 1, d f = 1, p v a l u e < 0. 0 5\right) $$
but has no significant
association with behavior (p value > 0.10). Concerning
locality, age, monthly income, person’s education, marital
status, and number of family members there were high
statistical associations with attitudes and behavior toward
COVID19 (p value > 0.001)concerning sector was high
statistical association with attitude (p value < 0.001), and statistical association of pvalue < 0.05 with the behavior.
Multivariate Analysis of Factors Associated with Attitudes towards COVID19: Logistic Regression Approach
Multivariate analysis was performed using the binary logistic regression by forward stepwise method with a likelihood ratio approach at a p value less than 0.25 in the bivariate analysis using chi-square test and Fisher’s exact test was included in the multivariable analysis.
Explanatory Variables β S.E. Wald df p value AOR 95% C.I. for AOR Lower Upper Monthly Income 17.65 3 0.001 < 1000 SDG 0.374 0.335 1.25 1 0.264 1.45 0.75 2.80 1000 -1999 SDG -0.225 0.271 0.69 1 0.407 0.80 0.47 1.36 2000-2999 SDG 0.809 0.214 14.32 1 0.000 2.25 1.48 3.41 Educational Level 41.02 4 0.000 Uneducated 2.524 0.790 10.19 1 0.001 12.47 2.65 58.72 Below Secondary School 2.328 0.440 27.95 1 0.000 10.26 4.33 24.32 Secondary School 1.284 0.314 16.71 1 0.000 3.61 1.95 6.68 Bachelor/Diploma 0.611 0.242 6.37 1 0.012 1.84 1.15 2.96 Marital status 31.21 3 0.000 Single -0.783 0.184 18.12 1 0.000 0.46 0.32 0.66 Divorced 0.870 0.384 5.13 1 0.024 2.39 1.12 5.07 Widowed 0.695 0.839 0.69 1 0.408 2.00 0.39 10.38 Table 3: Factors determined attitudes towards COVID19.
The model obtained is better fit than the baseline model, since the -2LL value for the selected model was 814.7. In addition, the Nagelkerke’s R2 suggests that the model explains roughly 24.4% of the variation in the outcome variable (i.e. attitudes towards COVID19).
Among the 10 factors presented in Table 3, the regression model indicated that three variables have significant effect on attitudes towards COVID19. Monthly income statistically has effect on attitudes towards COVID19 (Wald=17.65, DF=3, p <0.001). Those who earned between 2000-2999 SDG a month were 2.25 times more likely to have negative attitudes towards COVID19 ( 0.809 β = , p <0.001, AOR=2.25, 95% C.I.;
1.48 -3.41,). Educational Level statistically has significant
effect on attitudes towards COVID19 (Wald=41.02, DF=4,
p <0.001). Those who were uneducated (p value <0.001),
had below secondary school certificate (p value <0.001),
had secondary school certificate (p value <0.001), and had
Bachelor/Diploma certificate (p value <0.05) were more
likely to have negative attitudes towards COVID19, regarding
marital status Being a single has negative effect on attitudes
towards COVID19 ( (
$$ (\beta = - 0. 7 8 3, p v a l u e < 0. 0 0 1). $$
. In addition,
those who were divorced were 2.39 times more likely to have
negative attitudes towards COVID19 comparing with those
who were married (
0.876 β =
, p <0.05, AOR=2.39, 95% C.I.;
1.12 -5.07)
Multivariate Analysis of Factors Associated with Behavior towards COVID19: Logistic Regression Approach
| Explanatory Variables | B | S.E. | Wald | Df | Sig. | Exp(B) | 95% C.I. for EXP(B) | |
|---|---|---|---|---|---|---|---|---|
| Lower | Upper | |||||||
| Gender | -0.48 | 0.186 | 6.59 | 1 | 0.010 | 0.62 | 0.43 | 0.89 |
| Age | 25.98 | 4 | 0.000 | |||||
| Below 20 years | 1.08 | 0.660 | 2.66 | 1 | 0.103 | 2.94 | 0.81 | 10.71 |
| 20-29 years | -0.33 | 0.307 | 1.19 | 1 | 0.275 | 0.72 | 0.39 | 1.31 |
| 30-39 years | 0.38 | 0.328 | 1.35 | 1 | 0.246 | 1.46 | 0.77 | 2.78 |
| 40-49 years | 0.94 | 0.371 | 6.34 | 1 | 0.012 | 2.55 | 1.23 | 5.28 |
| Income | 20.24 | 3 | 0.000 | |||||
| < 1000 SDG | 0.68 | 0.348 | 3.84 | 1 | 0.050 | 1.98 | 1.00 | 3.91 |
| 1000 -1999 SDG | 0.31 | 0.278 | 1.23 | 1 | 0.267 | 1.36 | 0.79 | 2.35 |
| 2000-2999 SDG | 1.04 | 0.240 | 18.78 | 1 | 0.000 | 2.83 | 1.77 | 4.52 |
| Locality | 16.23 | 2 | 0.000 | |||||
| Bahri | 0.86 | 0.220 | 15.26 | 1 | 0.000 | 2.36 | 1.54 | 3.64 |
| Omdurman | 0.26 | 0.226 | 1.28 | 1 | 0.259 | 1.29 | 0.83 | 2.01 |
| Attitudes | -1.61 | 0.184 | 76.70 | 1 | 0.000 | 0.20 | 0.14 | 0.29 |
Table 3: Factors determined behavior towards COVID19-Logistic Regression.
Logistic regression with forward LR method was used. Model obtained was better fit than the baseline model, since the -2LL value for the selected model was 746.3 In addition, the Nagelkerke’s R2 suggests that the model explains roughly 34.4% of the variation in the outcome variable (i.e. behavior towards COVID19).
Five variables have significant effect on behavior towards COVID19. Gender statistically has negative effect on behavior. Males were 0.62 less likely to have poor behavior comparing with females ( 0.48 β = − , p <0.05, AOR=0.62, 95% C.I.; 0.43 -0.89). Age generally has significant effect on behavior (Wald=25.98, DF=4, p <0.001). Those who were between 40 to 49 years of age were 2.55 more likely to have poor behavior comparing with those who were in the upper class of age ( 0.94 β = , p <0.05, AOR=2.43, 95% C.I.; 1.23 -5.28).
Furthermore, monthly income statistically has effect on behavior towards COVID19 (Wald=20.24, DF=3, p <0.001).
Those who earned between 2000-2999 SDG a month were 2.83 times more likely to have poor behavior towards COVID19 ( 1.04 β = , p <0.001, AOR=2.83, 95% C.I.; 1.77 -4.52). In addition, residential area (locality) statistically has significant effect on behavior (Wald=16.23, DF=2, p <0.001). People in Bahri were 2.36 times more likely to have poor behavior comparing with those who were in Khartoum locality ( 0.86 β = , p <0.001, AOR=2.36, 95% C.I.; 1.54 -3.64). Participants’ who had positive attitudes were 0.2 times less likely to report poor behavior ( 1.61 β = − , p <0.001, AOR=0.20, 95% C.I.; 0.14 -0.29).
Determinants of Behavior: Decision Tree Analysis Approach
In Decision Tree analysis, the researchers entered ten independent variables and four variables of them namely attitudes, locality, age, and gender were included in the final model.
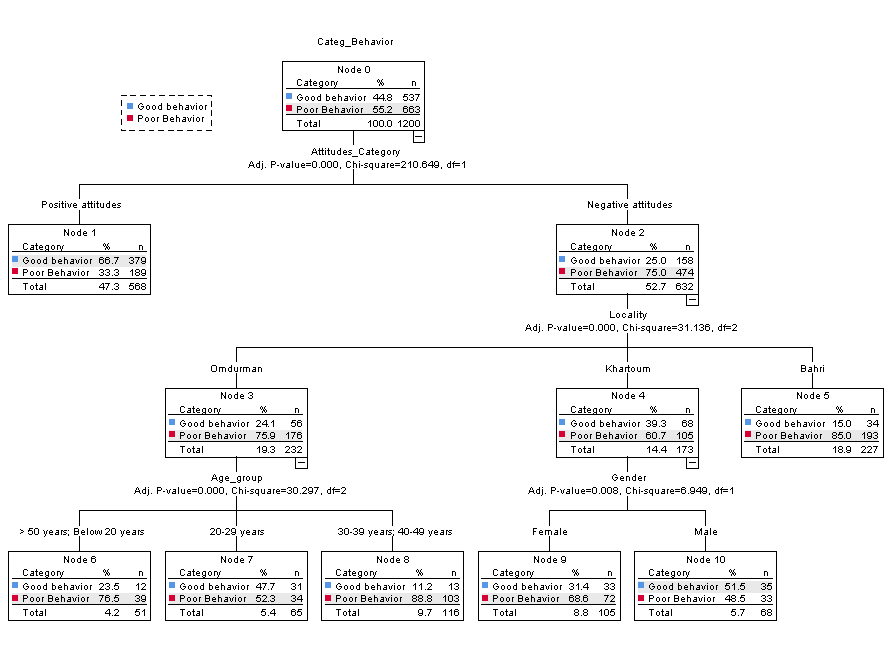
The other six variables did not make a significant contribution to the model, so they were automatically dropped. The tree diagram (graphic representation of the tree model) showed that using the CHAID method, attitudes was the best predictor of behavior towards COVID19. For negative attitudes category, the next best predictor is locality. In Omdurman locality slightly greater than three-quarters of those who have negative attitudes have poor behavior (75.9%), while in Khartoum locality slightly greater than three fifths of those who have negative attitudes have poor behavior (60.7%). Since there are no child nodes below Bahri locality node, therefore it considered a terminal node.
Furthermore, for Omdurman locality the next best predictor is participants’ age. For all categories of age the percentages of participants who have poor behavior varied between (52.3%) for those who were in 20-29 years and (88.8%) for who were in the next upper categories of age (30-39 and 40-49). Since there are no child nodes below age node, therefore it considered a terminal node.
For Khartoum locality, the next best predictor is participants’ gender. Proportion of females who reported poor behavior was (68.6%) among the group of females who classified as negative attitudes (n=105), while among the group of males who classified as negative attitudes (n=68) more than the half of the participants had good behavior (n=35, 51).
Discussion
Currently, the widespread of propagating COVID19 outbreak is constituted a major public threat universal. Hitherto, no treatment or vaccine has been discovered. Therefore, prevention is an only solely solution. Effective prevention and control of COVID-19 is achieved through increasing the populations’ encourage positive attitude, and behavior towards COVID19. To our knowledge, this study is a pathfinder community based study to be carried out in Sudan, which demonstrates attitude and behavior during the COVID-19 outbreak.
According to the findings of our study, among the attitude being investigated, greater than half (56.7%) of the participants have negative attitudes, while 47.3% the remaining have positive attitudes. This result is higher than that of other studies conducted in Saudi Arabia [15], China [16] (81%) and (74%) respectively. where the majority of participants have optimistically positive attitude confident that the disease is curable and their country will contain the disease. In Saudi Arabia, approximately 81% of participants had high confidence that the virus can be successfully controlled, and 97% are convinced that the Saudi government will control the outbreak. This discrepancy might be attributed by selecting certain stratum from their communities, which did not reflect the actual situation. More, they thought that the capabilities and preparedness health system and rapid response for such outbreaks and also these affluence countries and they have capabilities for prompt interventions.
Our results indicate the behavior of participant regarding COVID 19 was categorized into two; poor was noted in 55% (995% CI, 52.5% - 58.1%), whilst the good behavior was found in 45%. Our result is incoherence with Ethiopian study done by Akalu Y, et al. [17] which was reported poor behavior in (47.3%). This result could be explained by the similarity of social context of the two populations regarding customs, traditions and lifestyle. However, other studies found poor behavior was less than we found. For example, other studies conducted in Nigeria [18] and Uganda [19] reported that poor behavior was seen in 17.7% and 14.7% correspondingly. These discrepancies could be ascribed to the difference sources of information channels, intensively awareness and panic of COVID 19 outbreak.
This study found three factors are negatively affected behavior regarding COVID 19 (61%) of the total variance clarified, which were reported in; isolation strategy anticipated stigma and enacted stigma. The overwhelming of pessimistically behavior was entirely focused on the isolation strategy, thus refusal to be put in quarantine facility, besides the most the imagined phantom image of the isolation environment, lack of confidence in health authorities’ competency. This may be due to the fact that the health authorities did not take into account the use of effective mechanisms to reflect the ideal image of isolation centers. However, many studies have been conducted among those who had been quarantined found that there is a high prevalence of psychological symptoms, emotional disturbance, depression , stress, low mood, anger, and emotional exhaustion [20, 21, 22, 23, 24, 25, 26].
Demographic characteristics showcase that males have less likely poor behavior as compared to their females counterparts( 0.48 β = − , p <0.05, AOR=0.62, 95% C.I.; 0.43 -0.89). This finding is inconsistence with other authors’ findings [27, 28]. Further, also corresponding to other epidemiological studies which declared that females prone to poor behavior compared to males [29], this disparity might be attributed to those males had had exposed to extensive awareness.
This study found that an attitude was the best predictor of behavior towards COVID19. While for negative attitudes category, the next best predictor is locality. However Omdurman locality was found greater than three-quarters of the inhabitants had had negative attitudes and poor behavior (75.9%) compared to other localities. This variance might be
attributed to that Omdurman is more populated compared
to others. Further, in one study was conducted in China [30]
found that the variability of spatial has a role in behavioral
variation. Our study reported that, the monthly income
played major role in determining the individuals behaviors,
participants earned between 2000-2999 SDG a month
were 2.83 times more likely to have poor behavior towards
COVID19 compared with those who earned 3000 SDG and
$$ \mathrm {a b o v e} (\beta = 1. 0 4, $$
, p <0.001, AOR=2.83, 95% C.I.; 1.77 -4.52).
Furthermore, this result is supported enormous studies
carried out in Ethiopia [17], Malaysia [31] and United States
[32] which reported that participants with low income have
tendency of poor behavior of COVID-19.
This study found that participants aged between 40 - 49
years were 2.55 more likely to have poor behavior compared
with those who were in the upper class of age (
$$ (\beta = 0. 9 4, p $$
<0.05, AOR=2.43, 95% C.I.; 1.23 -5.28). This point could be
explained by the virulence of the disease that because of
those who elder are more vulnerable to the infection. This
finding agreed with Saudi study [33] that revealed good
practicing behavior among old age people and young was
considered that it is the disease of the old and young people;
therefore, to avoid getting this infection, their practicing
behavior was better.
Previous studies have shown different source of obtaining knowledge. Our study was conducted on first months of outbreak. The main source of information in this study was reported in TV (81.7%) followed by social media (68.9) in addition to at least each participant receive information from three different channels. This finding is supported by previous studies performed in Ethiopia [34], and Egypt [35] have shown social media platforms, and the internet represented the most important sources of information. This difference might be due to a difference in study populations’ socioeconomic and educational status, and can be explained by the time of data collection was early day strict lockdown were people exposure to TV could be more infodemic and multiple nonofficial source of information give chance to Rumors and spread of inaccurate information. In this study, infodemic and misconception was the main contributor in formulation negative attitude. Now, there has been increase in the internet access and usage to receive information about infection control [36]. Moreover, now a day’s internet is widely available and utilized to gain knowledge on evolving disease by many people. This has been proven from multiple studies published about the disease in China [37]. Again this reflects the effectiveness of the message provided by the different media platforms, which was confirmed by the negative assumptions that that media is exaggerating the risk (16.8% only thought that media outlets exaggerate the danger of the disease).
Misconceptions about COVID19 of statistically describe
person’s attitudes positively (
$$ (\beta = 0. 9 2 6, p - v a l u e < 0. 0 0 1) $$
; therefore, misconception was the main contributor in
forming negative attitude.
Participants perceptions was varied, 28% believed the disease is life-threatening danger and potentially fatal and the prognosis recorded in 31%. Up to 19% of our participants convinced the outbreak is a political lie, 42.5 % agree with it is God’s punishment and about (18.5%) of participants thought; the infection is associated with stigma. Many previous studies have been conducted are in agreement with our finding [38, 39, 40, 41].
Stigma (anticipated and enacted) was also extracted as factor changing behavior because of stigma hurts everyone by creating more fear or anger toward ordinary people instead of focusing on the disease that is causing the problem. Stigma can also make people more likely to hide symptoms or illness, keep them from seeking health care immediately, and prevent individuals from adopting healthy behaviors it also makes them practice some negative behaviors, such as distancing everyone who has been exposed to illness, even if he is cured, impeding ambulances and rejecting them in their areas. Our finding is in line with enormous authors’ results conducted elsewhere [42, 43, 44, 45]. This result in agreement with our finding, thus can be resolved through proper education
Conclusion
Majority of participants had had negative attitude. More than half of participants had a poor behavior. The spectrum of behavior was noted in; response to isolation strategy, anticipated stigma, and enacted stigma. Factors had occurred changing attitude were misconceptions about covid19, infodemics of COVID19, and negative stereotyping. Monthly income and education status were significantly associated with negative attitude.
Declarations
Declaration
Title of Manuscript: Breadth: Attitude and Behavior of Emerging a Novel COVID19 Disease Khartoum, Sudan I solemnly declare that this paper is genuinely original work carried out by the platform research group of Arab Open University and neither previously published nor currently under consideration by another Journal.
Ethics Statement
Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article. According to the World Health Organization Guidelines on Ethical Issues in Public Health Surveillance, a surveillance study in emergency outbreak situations is clearly exempted from ethical review and oversight (HO guidelines on ethical issues in public health surveillance. Geneva: World Health Organization; 2017. Licence: CC BY-NC-SA 3.0 IGO.).
Consent for Publication
I’m Dr. Khalid Abdalla Gasimalla Abdalla give my consent for Information about myself to be published in BMC Public Health journal. Khalid Abdalla Gasimalla Abdalla. I understand that the information will be published and full anonymity cannot be guaranteed. I have been offered the opportunity to read the article. This consent form will be submitted with the article and will be treated confidentially. Signing this consent form does not remove my rights to privacy. Name: Khalid Abdalla Gasimalla Abdalla Date: 10-Dec-20 Signed: Khalid Abdalla Gasimalla Abdalla
Availability of Data and Material
Data are available; nevertheless we need to publish more articles concerning COVID-19. These paper will be submitted sequentially during coming weeks. Competing Interests Funding The Arab Open University initially sponsored the tools of data designing and collection. Analysis was performed by two of the team of data collection. Other expenses paid by the member of the platform research group.
Authors’ contributions
All authors were contributed and work as a team since the designing, pretesting, collecting and analysising data. Moreover, also the team work collaboratively in writing the manuscript.
Acknowledgment
This study was fully supported by Arab Open University in Sudan. The Authors (Arab Open Research Group Members) thank all the involved participants for their cooperation and support. Special thank for the research assistants for data collection and management.
References
-
Li Q, Guan X, Wu P, Wang X, Zhou L, et al. (2020) Early transmission dynamics in Wuhan, China, of novel coronavirus–infected pneumonia. N Engl J Med 382(13): 1199-1207.
-
Wu JT, Leung K, Leung GM (2020) Nowcasting and forecasting the potential domestic and international spread of the 2019-nCoV outbreak originating in Wuhan, China: a modelling study. Lancet 395(10225): 689-697.
-
Ashour HM, Elkhatib WF, Rahman M, Elshabrawy HA (2020) Insights into the recent 2019 novel coronavirus (SARS-CoV-2) in light of past human coronavirus outbreaks. Pathogens 9(3): 186.
-
Chen N, Zhou M, Dong X, Qu J, Gong F, et al. (2020) Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. Lancet 395(10223): 507-513.
-
Holshue ML, DeBolt C, Lindquist S, Lofy KH, Wiesman J, et al. (2020) First case of 2019 novel coronavirus in the United States. N Engl J Med 382(10): 929-936.
-
Morganstein J (2020) Coronavirus and Mental Health: Taking Care of Ourselves During Infectious Disease Outbreaks. American Psychiatry Association.
-
An attitude is “a relatively enduring organization of beliefs, feelings, and behavioral tendencies towards socially significant objects, groups, events or symbols” (Hogg & Vaughan 2005, p. 150).
-
Shultz JM, Baingana F, Neria Y (2015) The 2014 Ebola Outbreak and Mental Health: Current Status and Recommended Response. JAMA 313: 567-568.
-
Ali BA-H (2016) The role of organizational behavior in the performance of business organizations. PhD thesis, College of Graduate Studies, Sudan University of Science and Technology.
-
Vigo D, Patten S, Pajer K, Krausz M, Taylor S, et al. (2020) Mental health of communities during the COVID-19 pandemic. Can J Psychiatry 65(10): 681-687.
-
Kunna E (2020) Sudan: Managing COVID-19 Pandemic during a Time of Transition. Arab Reform Initiative.
-
Hung LS (2003) The SARS epidemic in Hong Kong: What lessons have we learned?. Journal of the Royal Society of Medicine 96(8): 374-378.
-
Naib F, Suliman A (2020) Sudan: Spread facts, not fear, in the fight against COVID-19 As coronavirus (COVID). UNICEF.
-
Lemeshow S, Hosmer DW, Klar J, Lwanga SK (2020) World Health Organization. Adequacy of sample size in health studies. John Wiley & Sons.
-
Almofada SK, Alherbisch RJ, Almuhraj NA, Almeshary BN, Alrabiah B, et al. (2020) Knowledge, Attitudes, and Practices Toward COVID-19 in a Saudi Arabian Population: A Cross-Sectional Study. Cureus 12(6): e8905.
-
Zhong BL, Luo W, Li HM, Zhang QQ, Liu XG, et al. (2020) Knowledge, attitudes, and practices towards COVID-19 among Chinese residents during the rapid rise period of the COVID-19 outbreak: A quick online cross-sectional survey. Int J Biol Sci 16(10): 1745-1752.
-
Akalu Y, Ayelign B, Molla MD (2020) Knowledge, Attitude and Practice Towards COVID-19 Among Chronic Disease Patients at Addis Zemen Hospital, Northwest Ethiopia. Infection and drug resistance 13: 1949-1960.
-
Reuben RC, Danladi MMA, Saleh DA, Ejembi PE (2020) Knowledge, Attitudes and Practices Towards COVID-19: An Epidemiological Survey in North-Central Nigeria. J Community Health 46(3): 457-470.
-
Ssebuufu R, Sikakulya F, Binezero SM, Wasingya L, Nganza SK, et al. (2020) Awareness, knowledge, attitude and practice towards measures for prevention of the spread of COVID-19 in the Ugandans: A nationwide online cross-sectional Survey. medRxiv.
-
Mihashi M, Otsubo Y, Yinjuan X, Nagatomi K, Hoshiko M, et al. (2009) Predictive factors of psychological disorder development during recovery following SARS outbreak. Health Psychol 28(1): 91-100.
-
Yoon MK, Kim SY, Ko HS, Lee MS (2016) System effectiveness of detection, brief intervention and refer to treatment for the people with post-traumatic emotional distress by MERS: a case report of community-based proactive intervention in South Korea. Int J Ment Health Syst 10: 51.
-
Hawryluck L, Gold WL, Robinson S, Pogorski S, Galea S, et al. (2004) SARS control and psychological effects of quarantine, Toronto, Canada. Emerg Infect Dis 10(7): 1206-1212.
-
DiGiovanni C, Conley J, Chiu D, Zaborski J (2004) Factors influencing compliance with quarantine in Toronto during the 2003 SARS outbreak. Biosecur Bioterror 2(4): 265-272.
-
Lee S, Chan LY, Chau AM, Kwok KP, Kleinman A (2005) The experience of SARS-related stigma at Amoy Gardens. Soc Sci Med 61(9): 2038-2046.
-
Marjanovic Z, Greenglass ER, Coffey S (2007) The relevance of psychosocial variables and working conditions in predicting nurses’ coping strategies during the SARS crisis: an online questionnaire survey. Int J Nurs Stud 44(6): 991-998.
-
Maunder R, Hunter J, Vincent L (2003) The immediate psychological and occupational impact of the 2003 SARS outbreak in a teaching hospital. CMAJ 168(10): 1245- 1251.
-
Wang C, Pan R, Wan X, Tan Y, Xu L, et al. (2020) Immediate Psychological Responses and Associated Factors during the Initial Stage of the 2019 Coronavirus Disease (COVID-19) Epidemic among the General Population in China. Int J Environ Res Public Health 17(5): 1729.
-
Liu X, Kakade M, Fuller CJ, Fan B, Fang Y, et al. (2012) Depression after exposure to stressful events: lessons learned from the severe acute respiratory syndrome epidemic. Compr Pschiatry 53(1): 15-23.
-
Lim GY, Tam WW, Lu Y, Ho CS, Zhang MW, et al. (2018) Prevalence of Depression in the Community from 30 Countries between 1994 and 2014. Sci Rep 8(1): 2861.
-
Zhan S, Yang YY, Fu C (2020) Public’s early response to the novelcoronavirus–infected pneumonia. Emerg Microbes Infect 9(1): 534.
-
Azlan AA, Hamzah MR, Jen T, Id S, Hadi S, et al. (2020) Public knowledge, attitudes and practices towards COVID-19: a cross-sectional study in Malaysia. PLos One 15(5): 1-15.
-
Wolf SM, Serper M, Opsasnick L, Conor RMO, Curtis LM (2020) Awareness, attitudes, and actions related to COVID-19 among adults with chronic conditions at the onset of the U. S. outbreak: A Cross-sectional Survey. Ann Intern Med 173(2): 100-109.
-
Baig M, Jameel T, Alzahrani SH, Mirza AA, Gazzaz ZJ, et al. (2020) Predictors of misconceptions, knowledge, attitudes, and practices of COVID-19 pandemic among a sample of Saudi population and its impact: a cross- sectional study. medRxiv.
-
Bulck JVd (2004) Television viewing, computer game playing, and Internet use and self-reported time to bed and time out of bed in secondary-school children. Sleep 27(1): 101-114.
-
Choi K, Son H, Park M, Han J, Kim K, et al. (2009) Internet overuse and excessive daytime sleepiness in adolescents. Psychiatry Clin Neurosci 63(4): 455-462.
-
Cheng HC, Su CY, Huang CF, Chuang CY (2012) Changes in Compliance with Recommended Infection Control Practices and Affecting Factors Among Dentists in Taiwan. J Dent Educ 76(12): 1684-1690.
-
Li LQ, Huang T, Wang YQ, Wang ZP, Liang Y, et al. (2020) COVID-19 patients’ clinical characteristics, discharge rate, and fatality rate of meta-analysis. Journal of Medical Virology 92(6): 577-583.
-
Olapegba PO, Ayandele O, Kolawole SO, Oguntayo R, Gandi JC, et al. (2020) A preliminary assessment of novel Coronavirus (COVID-19) Knowledge and Perceptions in Nigeria. medRxiv.
-
Qureshi N, Shaikh BT (2006) Myths, fallacies and misconceptions: Applying social marketing for promoting appropriate health seeking behaviour in Pakistan. Anthropol Med 13(2): 131-139.
-
Tabish SA (2020) COVID-19 Pandemic: The crisis and the longer-term perspectives. J Cardiol Curr Res 13(2): 41-44.
-
Adegboye OA, Adekunle AI, Gayawan E (2020) Early transmission dynamics of novel coronavirus (COVID-19) in Nigeria. Int J Environ Res Public Health 17(9): 3054.
-
Uvais NA, Aziz F, Hafeeq B (2020) COVID-19-related stigma and perceived stress among dialysis staff. Journal of Nephrology 33(6): 1121-1122.
-
Uvais NA, Shihabudheen P, Bishurul Hafi NA (2020) Perceived stress and stigma among doctors working in COVID-19-designated hospitals in India. Prim Care Companion CNS Disord 22(4): 20br02724.
-
Wang C, Pan R, Wan X, Tan Y, Xu L, et al. (2020) A longitudinal study on the mental health of general population during the COVID-19 epidemic in China. Brain Behav Immun 87: 40-48.
-
Hao F, Tan W, Jiang L, Zhang L, Zhao X, et al. (2020) Do psychiatric patients experience more psychiatric symptoms during COVID-19 pandemic and lockdown? A case-control study with service and research implications for immunopsychiatry. implications for immunopsychiatry. Brain Behav Immun 87: 100-106.
- Psychogenic Erectile Dysfunction in Late Adulthood: A Case Report on Clinical Intervention and Intimacy Restoration
- Clinical Trials on COVID-19 in 2025: A New Chapter in Global Health Research
- Innovations and Challenges in Contemporary Medical Clinical Trials: An Editorial Perspective
- Innovations and Challenges in Contemporary Medical Clinical Trials: A Critical Perspective
- Reimagining Clinical Trials: The Power of Continuous Feedback from Medical Reports
- Factors Influencing Brain Drain: Perspectives from a Medical School in Turkey