Cerebellar Transcranial Direct Current Stimulation and Dual-Task Performance
The importance of accurate cognitive performance during a complex motor task is essential for professions including athletes, police and military personnel. Cerebellar Transcranial direct current stimulation (tDCS) has been used as a low-cost, non-invasive technique to enhance performance of individuals in a variety of isolated motor and cognitive tasks but not in a dual-task. Twenty healthy college-age individuals completed this study. A baseline dual-task was conducted with participants completing four cognitive tasks: Reaction Time (simple, choice) and Working Memory (Stroop and N-Back) while simultaneous maintaining balance on an unstable BioDex Balance platform. Each participant received anodal (n=10) or sham (n=10) cerebellar tDCS at 1mA.min for a total of 40mA.min (~45mins). During this time, participants completed cognitive and balance training. Participants repeated the dual-task testing immediately following training, and again one week later. Results showed no differences in cognitive performance between the tDCS and sham groups (p>0.05). Balance continued to show improvements during the simple cognitive tasks in the tDCS group one week later (p
Introduction
Cognitive function is imperative for all individuals because it encompasses both knowledge and abilities like memory, attention, and social skills. Much of the literature relating to cognition has focused on cognitive impairments 1, but it may also be valuable to improve cognition during a motor task in certain populations (athletes, military, police, etc). Similarly, multitasking has become more apparent (i.e. texting and walking), especially in the college aged population. Therefore, even those individuals without cognitive deficits could benefit from cognitive improvements during a motor task. There is new evidence that the cerebellum plays a role in cognition as well as the frontal lobe. Individuals with cerebellar lesions are seen to have memory problems [1, 2, 3] and difficulty with executive functioning [4]. Furthermore, there are neuronal loops within the brain that connect the cerebellum to outputs in both the frontal cortex and parietal cortex [5]. More recently, however, research has shown there is cerebellar activation during non-motor tasks [6] and cognitive tasks [7], specifically. Cerebellar activation during cognitive tasks confirms that the cerebellum also participates in networks involving cognition; it is not solely the frontal lobe. Although the cerebellum has been shown to play a role in cognition, its main behavioural outputs include motor planning [8], motor coordination and balance [9]. Furthermore, postural control is directly related to cerebellar disorders [10]. This is evident as damage to the cerebellum causes deficits in the loco motor systems [11]. High functioning loco motor systems are important as it directly relates to one’s motor function, which is imperative for everyday function. Therefore, enhancing cerebellar neurons could improve both balance and cognitive performance, thus improving one’s quality of life and ability to multitask. Dual-tasks force attentional processes to be exceeded, so balance, cognition, or both, will be compromised [10], which demonstrates how two different processes compete for the same resources. The amount one’s performance declines indicates the extent to which the two tasks share the same attentional resources [12]. Both cognitive function and balance tasks depend on the cerebellum; thus, in a dual-task condition, these tasks are diminished when compared to a single task [13, 14]. For example, postural stability has been seen to decline in populations with Parkinson’s disease while also completing a verbal cognitive task [15]. Similarly, more postural sway was reported during a dual-task condition in stroke survivors [16]. The current strategies for cognitive improvements mainly rely on “mind games” that require the participant to practice his or her cognitive abilities. This method is effective as learning a new skill strengthens neural connections and induces neural plasticity [17]. These activities can include games like Sudoku and crossword puzzles. More recently, however, Transcranial direct current stimulation (tDCS) has been on the rise as an alternate solution to these interventions as it induces similar plasticity changes [18, 19, 20, 21]. Each tDCS unit sends low amounts of current between the two electrodes, which either excites or inhibits the neurons where that electrode is placed on the brain, thus altering the electrical potential of those neurons. Most studies involving tDCS have focused on motor improvements [21, 22, 23, 24]. However, with the growing prevalence of cognitive deficits, this area has also become a growing interest for researchers. Given the neuronal connections within the brain, it is possible to indirectly stimulate different brain lobes via tDCS. Evidence that the cerebellum has output channels to the prefrontal cortex, presents a hopeful, alternate method for enhancing cognition. When looking at cognition, there are multiple avenues to investigate, like both working memory and decision-making. Some studies have found that tDCS can enhance working memory [25, 26, 27, 28, 29], yet each aspect of cognition is important to its overall function. Therefore, applying tDCS to the cerebellum can enhance cerebellar neurons and thus the neuronal loops connecting the cerebellum to the prefrontal cortex. Ultimately, cerebellar tDCS could improve both balance and cognitive performance during a dual-task. The purpose of this study is to determine the effects that cerebellar tDCS has on a dual-task consisting of balance and cognition.
Methods and Materials
Participants
Twenty healthy young adults with no known cognitive impairments took part in this study (male n=7, female n=13, mean age 20.75 years, range 20-22) and were included in statistical analysis. None of the participants had a history of neurologic concerns (i.e. epilepsy) or were taking any medication for cognitive or balance impairments. Four participants were medicated for ADHD, one had a previous diagnosis of dyslexia, and one had a previous knee surgery as self-reported on their Health History Information sheet. None of these disclosures were a concern for this task but were noted. Written informed consent was taken from all subjects. This study was approved by the institutional IRB.
Instrumentation
To deliver the stimulation, a Dupelionto phoresis device (Empi Inc., Vista, CA) was used with a 9-volt alkaline battery. Two electrode sponges (each 25 cm2, Amrex, Paramount, CA) saturated with sterile saline (0.9% NaCl) were placed on the scalp to help the electrodes pass current to the brain. In the anodal condition, the current was set to 1 mA $$ \mathrm {E} = \mathrm {E} _ {1} + \mathrm {E} _ {2} + \dots + \mathrm {E} _ {n} $$ min for a total charge of 40 mAmin. During stimulation (sham or anodal) participants alternated between cognitive and balance training. Cognitive training included crossword puzzles, Sudoku or a maze on an Etch-a-Sketch. Balance training consisted of completing exercises on the Bosu Ball (Bosu International Global Headquarters, Ashland, OH). Participants also completed a cognitive and balance dual-task. Participants were placed on a BioDex Balance System TM (BioDex Medical Systems Inc., Shirley, NY) in one of the four foot placements: balanced on one foot (right of left) or tandem (either right or left foot in front). During the balance task, participants simultaneously completed a cognitive task on an iPad using the Psych Lab 101 application (Simple Reaction Time, Choice Reaction Time, Numeric Stroop and N-Back) (Neurobehavioral Systems Inc., Berkeley, CA). In the Simple Reaction Time task, there was only one stimulus that participants needed to respond to while in the Choice Reaction Time task, there were two stimuli that required different responses. In the Numeric Stroop task, participants had to select the larger number based on either physical or numerical size. Lastly, in the N-Back task, participants were presented with a sequence of letters; they were instructed to respond when the current letter matched the letter from n letters previously in the sequence. In this study, participants completed both a 1-back and 2-back task.
Procedure (Figure 1)
Participants entered the lab where informed consent was received and they completed a Health History Information sheet. Participants then completed a dual- task (using the BioDex balance machine and cognitive tasks using the Psych101 application on an iPad) to obtain baseline measures of dual-task ability. The participant’s performance on the BioDex is noted as a stability index. The stability index represents the variance of platform displacement in degrees from level. A high number is indicative of a lot of motion, which is indicative of the patient having trouble balancing. Participants then received cerebellar tDCS (anodal or sham) by random assignment. Electrodes were placed on the participant’s cerebellum and DLPFC using the 10-20 system.
Researchers were then able to use this measured location to estimate the location of the electrodes for the rest of the participants. The physiological mechanisms of tDCS are still not well understood, particularly as to how it affects neuronal loops in the brain [30]. Furthermore, stimulation type (anodal or cathodal), when delivered to the cerebellum, is less important due to the complex folding of the cerebellum [28]; different neurons are facing different directions and thus, the exact mechanism of stimulation is unknown. However, anodal cerebellar tDCS has been seen to produce more short-term and long- term offline improvement in reaction time [29]. The anode was placed on the participant’s cerebellum while the cathode, the reference electrode, was placed on the right dorsolateral prefrontal cortex (DLPFC) see (Figure 1A). For most participants, anodal stimulation lasted for about 35 minutes, but skull and hair thickness can alter the exact amount of time it took to reach a total charge of 40 mA min. In the sham condition, the current was turned on for about 30 seconds until the total charge reached 1 mAmin. Similar to the anodal group, skull and hair thickness altered the amount of time it took for the charge to reach 1 mA, but the device was turned off when total charge reached 1 mA and remained turned off for the rest of the stimulation. Participants were unaware of which condition they were in; only two reported minimal discomfort and they both were in the sham condition. None of the participants had previously ever received tDCS stimulation, so delivering the current for a short period of time leads the participant to believe that he or she is receiving stimulation, even when the device has been turned off. While participants received cerebellar tDCS (anodal or sham), they alternated between completing cognitive and balance training. During cognitive training, participants chose to complete a Sudoku puzzle, crossword puzzle and/or a maze on the Etch-a-Sketch. Participants were instructed to engage in a cognitive training of their choice; every ten minutes, participants switched to complete balance training for five minutes before they switched back to cognitive training. During balance training, participants used a Bosu ball and were free to either complete squats, or merely stand on the ball with one foot or two feet whichever they deemed challenging. This allowed participants to work up to their comfort level: those who were worse at balance engaged in simpler balance tasks, while those participants who were more stable felt comfortable to engage in squats and other challenging balance training. After stimulation, participants completed the same dual-task. In cerebellar anodal tDCS, previous research has suggested online versus offline effects are not straightforward due to the complex twisting of neurons in the cerebellum [28].
Research has not looked into detail regarding specific effects of online versus offline tDCS [31] and its effects may be dependent on the specific function of the stimulated brain region [32]. However, offline cerebellar tDCS may be useful for improvement of offline motor learning [29]. Participants then came back one week later to complete the dual-task for a third time such that all our performance tests were completed offline (not during stimulation). Figure 1B shows the timeline of events.
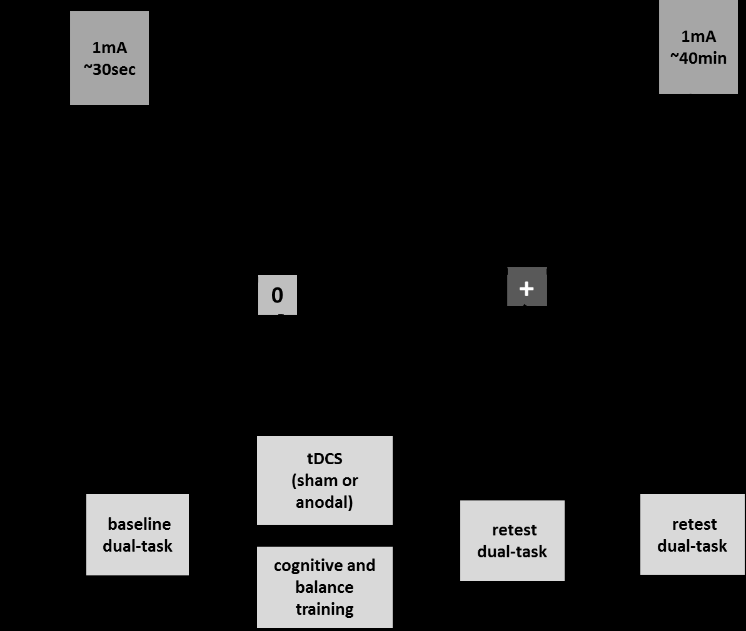
Figure 1A: Schematic of tDCS sponge placement for sham and stim. Figure 1B: Timeline of events.
Design and Analysis
A 3(time: pre, post, week) x 2(group: stim, sham) repeated measures MANOVA was conducted for the cognitive tasks including reaction time (simple, choice), Numeric Stroop accuracy and reaction time (congruent, incongruent, neutral), and the N-Back task reaction time and accuracy (target, detractor). In addition this 3(time) x 2(group) was run for the balance measures average across tasks (overall sway, AP sway, ML sway) and with task (4) entered as a repeated measure. Alpha level was set at p<0.05. Partial eta-squared (ƞp2) are also reported (0.01 - small effect size; 0.09 - medium effect size; 0.25 - large effect size).
Results
Cognitive Performance
For simple and choice reaction time, there was not a significant multivariate Time Effect (F(4, 72) = 1.57, p>0.05, ƞp2 = 0.08), or Time x Group interaction (F(4, 72) = 0.72, p>0.05, ƞp2 = 0.04) or Group Effect for Simple(F(1, 18) = 1.02, p>0.05, ƞp2 = 0.05) and Choice (F(4, 72) = 0.23, p>0.05, ƞp2 = 0.01) RT. For the Numeric Stroop task reaction time, there was not a significant multivariate Time Effect (F(12, 64) =1.05, p>0.05, ƞp2 = 0.17), or Time x Group interaction (F(12, 64) = 0.59 p>0.05, ƞp2 = 0.10) or Group Effect (F(1, 18)=0.27, p>0.05, ƞp2 = 0.02). Or for the Numeric Stroop task accuracy, there was not a significant multivariate Time Effect (F(10, 66) = 0.68, p>0.05, ƞp2 = 0.09), or Time x Group interaction (F(12, 64) = 1.15 p>0.05, ƞp2 = 0.15) or Group Effect (F(1, 18) = 1.0, p>0.05, ƞp2 = 0.05). For the N-Back task reaction time, there was not a significant multivariate Time Effect (F(8, 64) = 1.70, p>0.05, ƞp2 = 0.18), or Time x Group interaction (F(8, 64) = 1.29 p>0.05, ƞp2 = 0.14) or Group Effect (F(1, 17)=0.01, p>0.05, ƞp2 = 0.001). Or for the N-Back task accuracy, there was a significant multivariate Time Effect (F(8, 64) = 2.13, p>0.05, ƞp2 = 0.21), but not a significant Time x Group interaction (F(8, 64 ) = 1.0 p>0.05, ƞp2 = 0.11) or Group Effect (F(1, 17) = 0.39, p>0.05, ƞp2 = 0.02).
Balance Performance
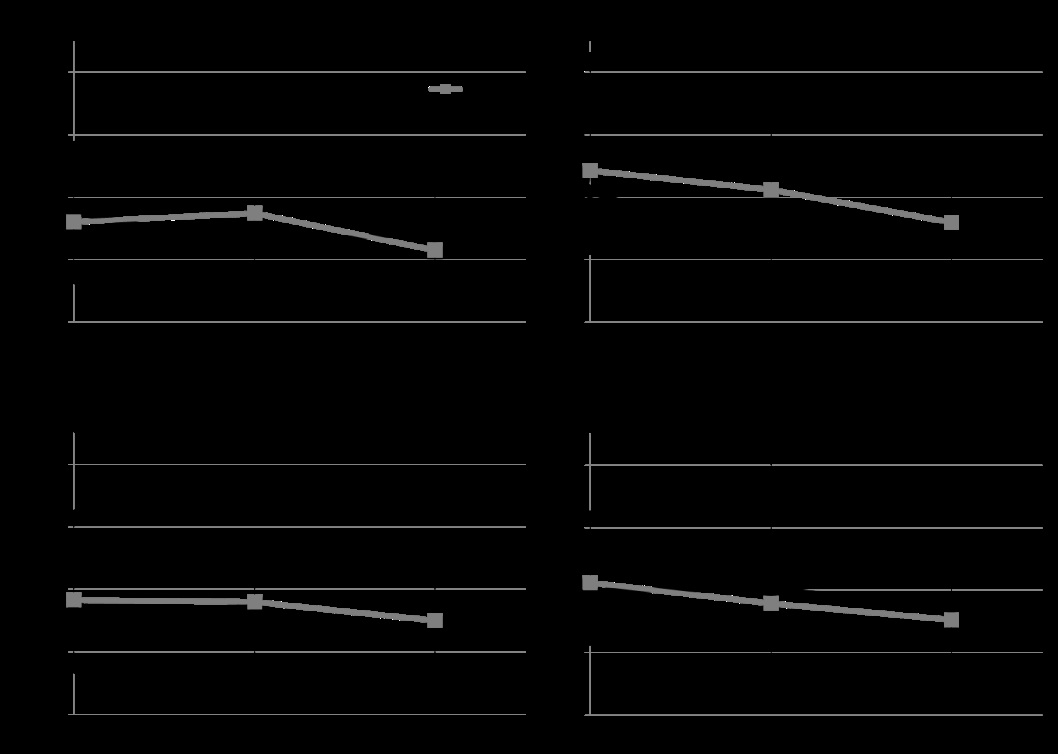
For balance sway scores were analyzed across time and task. There was not a significant Time Effect (F(6, 70)=1.59, p>0.05, ƞp2 = 0.12), Task Effect (F(9, 162)=0.73, p>0.05, ƞp2 = 0.04), Group Effect (F(1, 18)=0.3, p>0.05, ƞp2 = 0.01), a Time x Group Interaction (F(6, 70)=0.81, p>0.05, ƞp2 = 0.07), a Task x Group Interaction (F(9, 162)=0.96, p>0.05, ƞp2 = 0.02), or a Time x Task Interaction (F(18, 324)=0.70, p>0.05, ƞp2 = 0.04). There was a significant Time x Task x Group Interaction (F(18, 324) = 1.74, p=0.025, ƞp2 = 0.09). The Univariate analysis for Time x Task x Group interaction show a significant effect for Overall Sway (F(6, 108) = 2.48, p=0.028, ƞp2 = 0.12). As can be seen in Figure 2, overall sway continues to improve in the tDCS group one week after stimulation for the Simple and Choice Reaction time tasks but whereas in the sham group that improvement did not continue and they return to baseline levels (Figure 2A & 2B). In the working memory tasks we see continued improvement in balance one week later for both groups (Figure 2C & 2D).
This study tested the effects of cerebellar tDCS during a dual-task consisting of balance and cognition in healthy, young adult students. Results suggest that the training was enhanced with stimulation to some degree and continued one week later when the dual-task being performed did not involve working memory. Based on many of these moderate effect sizes, there doesn’t seem to be a power issue with this data but rather a need to conduct longer training times in this dual-task or a different stimulation configuration. It is also possible that a healthy young adult population is already showing strong performances on cognitive and balance tasks and thus training is not as effective as it would be in a group that was compromised in one or both of these tasks. Previous research using cerebellar tDCS has found improvements in a working memory task [28]. They used a Paced Auditory Serial Addition Test (PASAT) as well as a novel Paced Auditory Serial Subtraction Test (PASST), which are demanding cognitive task that involves working memory, attention and arithmetic capabilities [28]. This task presented a harder working memory task for the participants, which ultimately left more room for improvement. Similarly, Boehringer and colleagues [25] assessed participants’ performance in forward and backward digit spans as a measure of verbal working memory. Sequences of digits were read and participants were asked to recall digits in forward or backward order immediately after and the number of digits per sequence was increased if a participant successfully recalled a given sequence length twice. Both of these studies found improvements in cognition using tDCS, but these participants were performing each task at an individual difficulty level to avoid ceiling effects, which were not controlled for in the current study.
This study looked at a dual-task of balance and cognition. However, by nature, the cognitive tasks themselves required a motor component as well because participants needed to tap the iPad to respond to certain stimuli. The dual-task that was used in this study had a larger motor component than cognitive component and therefore, could be a factor as to why fewer cognitive improvements were seen amongst the participants. tDCS is a novel intervention in regards to the ability to excite neuronal loops within the brain. The exact mechanism of excitation or inhibition is unknown and it is further complicated by the interference of one’s skin, skull and cerebrospinal fluid [33]. Vöröslakos and colleagues found that only about 25% of the current from tDCS actually enters the brain [30]. Therefore, it may be necessary to increase tDCS current to 4-6 mA to reach a 1 mV/mm voltage gradient in the brain, which is needed to reliably affect neuronal loops [30]. This study used a current of 1 mA, which may not be large enough to actually alter the neuronal loops and ultimately why cognitive improvements were not noted. tDCS uses both an anode and a cathode to send current through the brain. In this study, the anode was placed on the cerebellum, which has been seen to show improvements in balance and cognition. However, the cathode, which has been seen to inhibit neurons [25] was placed on the DLPFC. This inhibition to the DLPFC could explain why cognition did not improve in this study, although caution should be used in this interpretation as we also did not see cognitive inhibition which is typically shown in cathodal configurations. Further research with tDCS and detailed analysis of cerebellar pathways may help researchers understand the impact of anodal versus cathodal stimulation. To date research has shown improvements using both techniques and we were not able to replicate those finding with any magnitude in this study. Training of participants included cognitive and balance tasks, but the exact time on each task was not controlled. Participants were asked to challenge themselves and were welcome to change tasks at anytime. They were instructed to engage in balance training every 10 minutes with all participants completing at least 3 balance training components. This is a therapeutic model setting, but there are limitations on how to interpret these results based on the possibility that individuals did different things. In addition, it is worth noting that the small sample size of this study limits the power of statistical findings. Furthermore, this was not a double-blinded study. While the participant was blinded to the treatment, the experimenter was not. However both cognitive and balance performance was evaluated using objective measures. The strength of this work is assessing the efficacy of using tDCS as a therapeutic tool. These types of studies we and other experts in tDCS have published previously [30, 31, 32, 33].
Conclusion
This research is important as many tDCS studies show positive outcomes and improvements in performance with stimulation. tDCS is used commercially to enhance cognitive skills in tasks such as gaming. This research suggests that caution should be used in when applying this technology to healthy populations in complex tasks. There is no evidence that it hurts performance or health, but it is likely an added cost with little benefit. Future research should increase training sessions to determine if this effect would be enhanced over time and across tasks, but short term cerebellar tDCS use does not seem beneficial in a dual-task.
References
-
Gottwald B, Wilde B, Mihajlovic Z, Mehdorn HM (2004) Evidence for distinct cognitive deficits after focal cerebellar lesions. J Neurol Neurosurg Psychiatry 75(11): 1524-1531.
-
Sokolov AA, Miall RC, Ivry RB (2017) The cerebellum: Adaptive prediction for movement and cognition. Trends Cogn Sci 21(5): 313-332.
-
Fiez JA, Petersen SE, Cheney MK, Raichle ME (1992) Impaired non-motor learning and error detection associated with cerebellar damage. A single case study. Brain pp: 155-178.
-
Schmahmann JD, Sherman JC (1998) The cerebellar cognitive affective syndrome. Brain J Neurol 121(4): 561-579.
-
Middleton FA, Strick PL (2000) Basal ganglia and cerebellar loops: motor and cognitive circuits. Brain Res Brain Res Rev 31(2-3): 236-250.
-
Stoodley CJ, Schmahmann JD (2009) Functional topography in the human cerebellum: a meta-analysis of neuroimaging studies. Neuro Image 44(2): 489- 501.
-
Krienen FM, Buckner RL (2009) Segregated fronto- cerebellar circuits revealed by intrinsic functional connectivity. Cereb Cortex 19(10): 2485-2497.
-
Ilg W, Synofzik M, Brötz D, Burkard S, Giese MA (2009) Intensive coordinative training improves motor performance in degenerative cerebellar disease. Neurology 73(22): 1823-1830.
-
Bunn LM, Marsden JF, Giunti P, Day BL (2015) Training balance with opto-kinetic stimuli in the home: a randomized controlled feasibility study in people with pure cerebellar disease. Clin Rehabil 29(2): 143-153.
-
Shumway Cook A, Woollacott MH (2011) Motor Control: Translating Research into Clinical Practice; 4(Edn.), LWW: Philadelphia, ISBN 9781608310180.
-
Van Donkelaar P, Lee RG (1994) Interactions between the eye and hand motor systems: disruptions due to cerebellar dysfunction. J Neurophysiol 72(4): 1674- 1685.
-
Jamet M, Devitern D, Gauchard GC, Vançon G, Perrin PP (2007) Age-related part taken by attentional cognitive processes in standing postural control in a dual-task context. Gait Posture 25(2): 179-184.
-
Ashburn A, Stack E, Pickering RM, Ward CD (2001) A community-dwelling sample of people with Parkinson’s disease: characteristics of fallers and non-fallers. Age Ageing 30(1): 47-52.
-
Marchese R, Bove M, Abbruzzese G (2003) Effect of cognitive and motor tasks on postural stability in Parkinson’s disease: a posturographic study. Mov Disord Off J Mov Disord Soc 18(6): 652-658.
-
O’Shea S, Morris ME, Iansek R (2002) Dual task interference during gait in people with Parkinson disease: effects of motor versus cognitive secondary tasks. Phys Ther 82(9): 888-897.
-
Bensoussan L, Viton JM, Schieppati M, Collado H, Milhe de Bovis, et al. (2007) Changes in postural control in hemiplegic patients after stroke performing a dual task. Arch Phys Med Rehabil 88(8): 1009-1015.
-
Madhavan S, Shah B (2012) Enhancing motor skill learning with Transcranial direct current stimulation - a concise review with applications to stroke. Front Psychiatry 3: 66.
-
Erickson KI, Colcombe SJ, Wadhwa R, Bherer L, Peterson MS, et al. (2007) Training-induced plasticity in older adults: effects of training on hemispheric asymmetry. Neurobiol Aging 28: 272-283.
-
Grimaldi G, Argyropoulos GP, Boehringer A, Celnik P, Edwards MJ, et al. (2014) Non-invasive cerebellar stimulation--a consensus paper. Cerebellum Lond Engl 13: 121-138.
-
Madhavan S, Sriraman A, Freels S (2016) Reliability and Variability of tDCS Induced Changes in the Lower Limb Motor Cortex. Brain Sci 6(3): 26.
-
Hendy AM, Tillman A, Rantalainen T, Muthalib M, Johnson L, et al. (2016) Concurrent transcranial direct current stimulation and progressive resistance training in Parkinson’s disease: study protocol for a randomised controlled trial. Trials 17(1): 326.
-
Dumel G, Bourassa ME, Desjardins M, Voarino N, Charlebois-Plante C, et al. (2016) Multisession Anodal tDCS Protocol Improves Motor System Function in an Aging Population. Neural Plast.
-
Galea JM, Celnik P (2009) Brain polarization enhances the formation and retention of motor memories. J Neurophysiol 102(1): 294-301.
-
Schabrun SM, Lamont RM, Brauer SG (2016) Transcranial Direct Current Stimulation to Enhance Dual-Task Gait Training in Parkinson’s Disease: A Pilot RCT. PLOS ONE 11(6).
-
Boehringer A, Macher K, Dukart J, Villringer A, Pleger B (2013) Cerebellar transcranial direct current stimulation modulates verbal working memory. Brain Stimulat 6(4): 649-653.
-
Fregni F, Boggio PS, Nitsche M, Bermpohl F, Antal A, et al. (2005) Pascual-Leone, A. Anodal Transcranial direct current stimulation of prefrontal cortex enhances working memory. Exp Brain Res 166(1): 23-30.
-
Pope PA, Brenton JW, Miall RC (2015) Task-Specific Facilitation of Cognition by Anodal Transcranial Direct Current Stimulation of the Prefrontal Cortex. Cereb Cortex 25(11): 4551-4558.
-
Pope PA, Miall RC (2012) Task-specific facilitation of cognition by cathodal Transcranial direct current stimulation of the cerebellum. Brain Stimul 5(2): 84- 94.
-
Ferrucci R, Bocci T, Cortese F, Ruggiero F, Priori A (2016) Cerebellar Transcranial direct current stimulation in neurological disease. Cerebellum Ataxias 3(1): 16.
-
Vöröslakos M, Takeuchi Y, Brinyiczki K, Zombori T, Oliva A et al. (2018) Direct effects of Transcranial electric stimulation on brain circuits in rats and humans. Nat Commun 9(1): 483.
-
Monti A, Ferrucci R, Fumagalli M, Mameli F, Cogiamanian F, et al. (2013) Transcranial direct current stimulation (tDCS) and language. J Neurol Neurosurg Psychiatry (8): 832-842.
-
Pirulli C, Fertonani A, Miniussi C (2013) the role of timing in the induction of neuromodulation in perceptual learning by Transcranial electric stimulation. Brain Stimul 6(4): 683-689.
-
Datta A, Dmochowski JP, Guleyupoglu B, Bikson M, Fregni F (2013) Cranial electrotherapy stimulation and Transcranial pulsed current stimulation: a computer based high-resolution modeling study. Neuroimage 65: 280-287.
- A Review of Gene Therapy for Parkinson's Disease to Control Dopaminergic Neurons
- Late-Onset Myasthenia Gravis in a Patient with Recurrent Breast Cancer: A Case Report
- Covid-Induced Dystonia and Opsoclonus: A Case Report
- Generalized Tonic-Clonic Seizure in a Pediatric Patient with Sunflower Syndrome: A Case Report
- Comparison of Doppler Guided Seldinger Technique Versus Classic Palpatory Seldinger Technique for Radial Artery Cannulation-an Open Label Randomized Controlled Trial
- Brown Sequard Syndrome: Understanding the Complexities of Spinal Cord Injury