Immune Checkpoint Therapeutics for Today’s Fight and Beyond
An important hallmark of cancer is its ability to escape immune surveillance by developing several immunological barriers. These include a plethora of mechanisms that either dampen immune cell functionality, or foster tumor cell resistance towards immune attack. Immunotherapeutic strategies, such as immune checkpoint (IC) blockade, have emerged as promising therapeutic approaches for cancer treatment. However, the majority of tumor patients are refractory to current immune therapeutic tools, emphasizing the need to identify more key players that could radically improve immunotherapy efficacy. The variability of patients’ responses to immunotherapy can be ascribed to a differential immune signature across different tumors. Therapeutic strategies that reinforce the immune system against cancer are opposed by the numerous immune modulatory mechanisms exploited by the tumor and its microenvironment. This review aimed to achieve a comprehensive overview of tumor immunological features by untravelling the key arsenal of immune modulators expressed by tumor cells
Introduction
Many hematological and solid malignancies can escape our natural antitumor immunity by disrupting immune checkpoint (IC) expression and interaction. Immune checkpoint inhibitors (ICI), a promising immunotherapy, re- regulate the activity of cytotoxic T lymphocytes and c) cells re-establishing and enhancing innate immunity. Therapies targeting ICs such as cytotoxic T-lymphocyte antigen (CTLA-4), programmed cell death (PD-1), and its ligand (PD-L1), have been approved by the FDA to treat various cancers [1]. Despite their promise, IC therapies often suffer from non-response in most patients, a condition termed primary resistance. Other patients, who respond initially, can develop resistance and experience tumor relapse, defined as acquired resistance [2]. Altogether, only a small percentage of patients is responsive to ICI therapy, limiting their clinical application. Thus, focus has shifted to exploring the underlying mechanisms responsible and finding new ICs or combination treatment strategies to improve treatment efficacy.
Cancer Immunoediting
The current theory of cancer immunoediting is based
on a multitude of studies on genetically modified mouse models with altered immune system [3]. Additionally, there are several proofs that cancer immunoediting occurs in humans as well. The most convincing evidence is the correlation among the quantity, the quality and the spatial distribution of tumor-infiltrating lymphocytes (TILs) and patient survival [4]. The complex interplay between aberrant cells and immune cells can be schematized into three main phases: elimination, equilibrium, and escape [5].
The immune system can prevent tumor formation and progression using at least three different mechanisms. First, immune cells are able to clear viral infections, thus protecting the host from virus-associated tumors. Second, elimination of pathogens by the immune system prevents the establishment of a pro-inflammatory milieu, which promotes tumorigenesis. Finally, immune cells are able to directly build up an efficient response against tumor cells [3]. The latter mechanism is also referred to as immune surveillance, and is mainly mediated by two cell subsets: NK cells and CD8+ T cells, also called cytotoxic T lymphocytes.
Cancer immune equilibrium is conceived as a period during which tumor cells and immune cells reach a steady state [5]. In this phase, immune cells arrest cancer progression without eliminating the tumor. The concept of immune equilibrium derives from the observation that tumors can reach a dormant stage in the body [6]. Cancer dormancy is a phase in tumor progression where cells undergo quiescence because of unfavorable conditions from the tumor microenvironment such as lack of appropriate growth factors [7, 8].
The persistency of the immune system, together with the genomic instability of cancer cells, ultimately results in the formation of resistant malignant cell variants. In the later stage of equilibrium, the accumulation of selected malignant clones with molecular abnormalities renders the tumor less immunogenic, thus preparing the soil for the tumor immune escape phase [9, 10]. Cancer immune escape is the ultimate phase of cancer immunoediting. This phase consists in the establishment of multiple resistance mechanisms, developed by the tumor and its microenvironment, to elude both the innate and the adaptive anti-tumor immune responses [11]. As a result, the tumor progresses uncontrolled, thus leading to a clinically progressive disease.
Immune Checkpoint Inhibitor Resistance Mechanisms
ICI resistance mechanisms are classified as either primary or acquired. They encompass cancer cell alterations, including immune recognition, cell signaling, gene expression, DNA damage response and T-cell activation process [12]. Currently, several resistance mechanisms have been identified. In this article, the major mechanisms contributing to primary and acquired resistances are explored.
Immune Contexture
Immune contexture, also known as tumor microenvironment (TME), refers to immune factors extrinsic to cancer cells (immune and stromal cells, cytokines, and other biologics that influences therapeutic response) [13]. Within this microenvironment, molecular and cellular compositions are altered establishing an immunosuppressive climate. Regulatory T cells (Tregs), myeloid-derived suppressor cells, and tumor-associated macrophages all contribute to this modification through various mechanisms including cytokine secretion, T effector cell suppression, and elevated transforming growth factor beta (TGF-b). This contributes directly to primary resistance of ICI therapy.
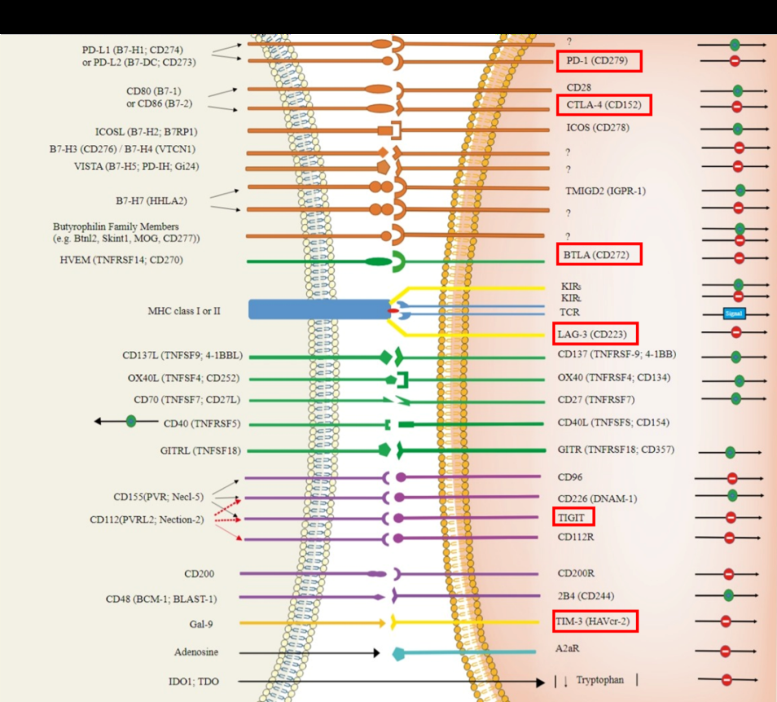
Co-opting Alternative Immune Checkpoints
A critical part of our innate immune response is the evolution of response, a process that is often manipulated in tumor malignancies. Unlike the TME which generates an immunosuppressive climate, the modification in immune response inhibits T cell proliferation and diversification. This generally starts through the overexpression of ICs, including CTLA-4 and PD-1. In cases of acquired resistances to CTLA-4 and PD-1 IC therapies, overexpression of alternate ICs has been observed. Alternate IC receptors include mucin domain -3 protein (TIM-3) and lymphocyte- activation gene 3 (LAG-3), B and T lymphocyte attenuator (BTLA), T-cell immunoreceptor tyrosine-based inhibition motif domain (TIGIT), and V-domain immunoglobulin- containing suppressor of T-cell activation (Figure 1). Co- expression of multiple ICs results in a severely exhausted T-cell state causing impaired effector function, progressive loss of T cell function, altered transcriptional states, and antigen persistence. In cases of upregulated, co-expressed ICs, targeting or co-targeting these alternative checkpoint receptors may serve as a potential solution to preventing acquired resistance.
Tumor Immunogenicity
Finally, the last resistance mechanism towards IC therapies is tumor immunogenicity, otherwise known as sensitivity to immune effector molecules. Tumor immunogenicity can be measured by the number of immunogenic neoantigens recognized as foreign or tumor mutational burden (TMB). Heterogeneous tumors that interact with the immune system preferentially select low TMB tumors. This phenomenon is a major contributor to acquired resistance, as shown in a study on relapsed non- small-cell lung carcinomas (NSCLC) [14].
Novel Immune Checkpoint Targets for Immunotherapy
Based on the insights highlighted above, the role of ICs in guiding the innate immune system is clear. Over- and under- expression of ICs can be considered as a driving factor in building the immune suppressive TME and altering immune response evolution. However, variation in response to ICI therapy indicates the complexity of ICI resistance and the presence of undiscovered mechanisms. As such, developing new ICI therapies have the potential to overcome resistance mechanisms and expand the limited applications of current immunotherapies.
One notable ICI is LAG-3. LAG-3 is a major immunosuppressive molecule that downregulates T cell cytokine production, CD4/8 expansion, and favors Treg adoption to prevent tissue damage and autoimmunity [15, 16]. Blockade of LAG-3 results in a favorable immune activation against tumor cells while further enhancing other ICIs. Clinically, pairing LAG-3 with PD-1 therapy results in an augmented therapeutic effect, whereas LAG-3 monotherapies only give a moderate response. Recently, a LAG-3/PD L1 combination therapy (Opdualag) was approved by the FDA for unresectable or metastatic melanoma [17]. Over 100 clinical trials evaluating LAG-3 inhibitors are ongoing, further highlighting its potential as an IC therapy.
Another potential IC target is TIM-3. TIM3 is expressed on a wide variety of immune cells including CD4/8 T cells, Tregs, myeloid cells, NK cells, and mast cells [18]. The cellular diversity of TIM-3 results in immune response modulation through multiple cell pathways. For now, the pathophysiology of TIM-3 in innate immunity remains elusive, however, its role across various cell pathways and the significant preclinical data supports TIM-3 as IC, thus revealing itself as a promising treatment method for immunotherapy across various diseases beyond cancer.
Perspectives on Immune Checkpoint Therapies
Despite the significant potential of immunotherapy, ICI therapies have found limited use due to the prevalence of primary or acquired resistance and narrow indications for use. In part, this stems from an incomplete understanding of the ICs and resistance mechanisms, as well as a limited number of actionable IC targets for therapeutic use. Despite current gaps in knowledge, clinically and biologically, the initial promising results and durable responses of immunotherapies cannot be ignored. The potential of immunotherapy towards unlocking the secrets of our innate defense defenses is immense.
References
-
Archilla-Ortega A, Domuro C, Marn-Liberal J, Muñoz P (2022) Blockade of novel immune checkpoints and new therapeuc combinaons to boost antumor immunity. J Exp Clin Cancer Res 41(1): 62.
-
Bagchi S, Yuan R, Engleman EG (2021) Immune Checkpoint Inhibitors for the Treatment of Cancer: Clinical Impact and Mechanisms of Response and Resistance. Annu Rev Pathol 16: 223-249.
-
Vesely MD, Kershaw MH, Schreiber RD, Smyth MJ (2011) Natural Innate and Adaptive Immunity to Cancer Senescence and tumour clearance is triggered by p53 restoration in murine liver carcinomas. Annual Review of Immunology 29(1): 235-271.
-
Schreiber RD, Old LJ, Smyth MJ (2011) Cancer Immunoediting: Integrating Immunity’s Roles in Cancer Suppression and Promotion. Science 331(6024): 1565- 1570.
-
Dunn GP, Bruce AT, Ikeda H, Old LJ, Robert D (2002) SchreiberCancer immunoediting: from immunosurveillance to tumor escape. Nat Immunol 3(11): 991-998.
-
Aguirre-Ghiso JA (2007) Models, mechanisms and clinical evidence for cancer dormancy. Nat Rev Cancer 7(11): 834-846.
-
Ranganathan AC, Adam AP, Aguirre-Ghiso JA (2006) Opposing Roles of Mitogenic and Stress Signaling Pathways in the Induction of Cancer Dormancy. Cell cycle 5(16): 1799-1807.
-
Wikman H, Vessella R, Pantel K (2008) Cancer micrometast asis and tumour dormancy. APMIS 116(7- 8): 754-770.
-
Hakansson L (2009) The capacity of the immune system to control cancer. Eur J Cancer 45(12): 2068-2070.
-
Felsher DW (2006) Tumor dormancy: death and resurrection of cancer as seen through transgenic mouse models. Cell Cycle 5(16): 1808-1811.
-
Dunn GP, Old LJ, Schreiber RD (2004) The three Es of cancer immunoediting. Annu Rev Immunol 22: 329-360.
-
Fares CM, Van Allen EM, Drake CG, Allison JP, Hu- Lieskovan S (2019) Mechanisms of Resistance to Immune Checkpoint Blockade: Why Does Checkpoint Inhibitor Immunotherapy Not Work for All Paents? Am Soc Clin Oncol Educ Book 39: 147-164.
-
Hassan G, Seno M (2020) Blood and Cancer: Cancer Stem Cells as Origin of Hematopoiec Cells in Solid Tumor Microenvironments. Cells 9(5): 1293.
-
Anagnostou V, Smith KN, Forde PM, Niknafs N, Bhattacharya R, et al. (2017) Evoluon of neoangen landscape during immune checkpoint blockade in non- small cell lung cancer. Cancer Discov 7: 264-276.
-
Maruhashi T, Sugiura D, Il-Mi O, Okazuki T (2020) LAG- 3: from molecular funcons to clinical applications. J Immunother Cancer 8(2): e001014.
-
Marin-Acevedo JA, Kimbrough EO, Lou Y (2021) Next generation of immune checkpoint inhibitors and beyond. J Hematol Oncol 14(1): 45.
-
Food and Drug Administration (2022) FDA approves Opdualag for unresectable or metastatic melanoma.
-
Wolf Y, Anderson AC, Kuchroo VK (2020) TIM3 comes of age as an inhibitory receptor. Nature Reviews Immunology 20(3): 173-185.
- Cancer Diagnosis from RNA Sequence of Blood Cells by Using AI
- Field Cancerization in Oral Cavity, Case Report and Review of Literature. Oncologic Program Salud Integral Hospital, Managua, Nicaragua
- Identification of B Lymphocytes in Cancer Patient’s Blood
- A Case Report of a Breast Cancer Patient Developing Pneumonitis as a Result of Abemaciclib Therapy
- The Amalgamated Sophomore-Gonadoblastoma
- Festered and Fenced-Lymphoepithelial Carcinoma Lung