Identification of B Lymphocytes in Cancer Patient’s Blood
B lymphocytes, integral to the adaptive immune system, are known for generating immune responses through antibody production and aiding T-cell-mediated immunity against pathogens. However, their role in cancer biology remains less established. Recent findings indicate that cancer patients exhibit an increased total B-cell population compared to healthy individuals, suggesting a potential protective role against tumour growth via anti-tumour immune responses. Yet, the underlying biology is complex. This study investigates B-cell dynamics in breast cancer patients’ blood, revealing shifts in B-cell subtypes that influence immune suppression and tumour progression.
Mayukh Mukherjee
Keywords: B Lymphocytes; Cancer; Tumour Immunology; Breast Cancer
PBMC: Peripheral Blood Mononuclear Cells; TME: Tumour Microenvironment; Breg: Regulatory B Cells; Beff: Effector B Cells; FACS: Fluorescence-Activated Cell Sorting.
Introduction
It has been well described, that there has been a dynamic relationship between the immune system and the development of cancer. The tumour microenvironment (TME) plays an essential role in modulating immune responses during the progress of cancer. Cancer still remains a major cause of death world-wide down the line. Over the past few decades, it has been established that cancer is not simply a genetic disease but rather a complex ecosystem composed of cancer cells, extracellular matrix (ECM), resident mesenchymal support cells, endothelial cells, and infiltrated immune cells.
There is a balance between immune effector cells and immunosuppressive cells in the TME.
There has been evidence collected that tumour- associated immune cells act in concert to both controlling and promoting the tumour formation. Immune cells like effector CD4+ T-cells, CD8+ T-cells, NK cells and M1 macrophages attack the cancer cells to reduce their proliferation and growth. Other site cells like T-regulatory cells, myeloid- derived suppressor cells, M2 macrophages, etc helps in tumour progression by inhibiting the functions of effector immune cells to make an immunosuppressive environment.
Tumour cells evade attacks to the immune system by using 2 strategies: avoiding the immune recognition and instigating an immunosuppressive TME.
At first, there is a high chance that cancer cells lose the expression of tumour antigens on the cellular surface, and thus, CD8+ T cells cannot recognize them.
Secondly, cancer cell-derived factors instigate an immune-tolerant environment. This is done by Secretion of suppressive molecules such as IL10 and TGFβ. Recruitment of immunosuppressive M2 macrophages, MDSCs, and Treg
cells by tumour-derived chemokines Thus, there forms a complete and efficient system for immune evasion Figure 1.
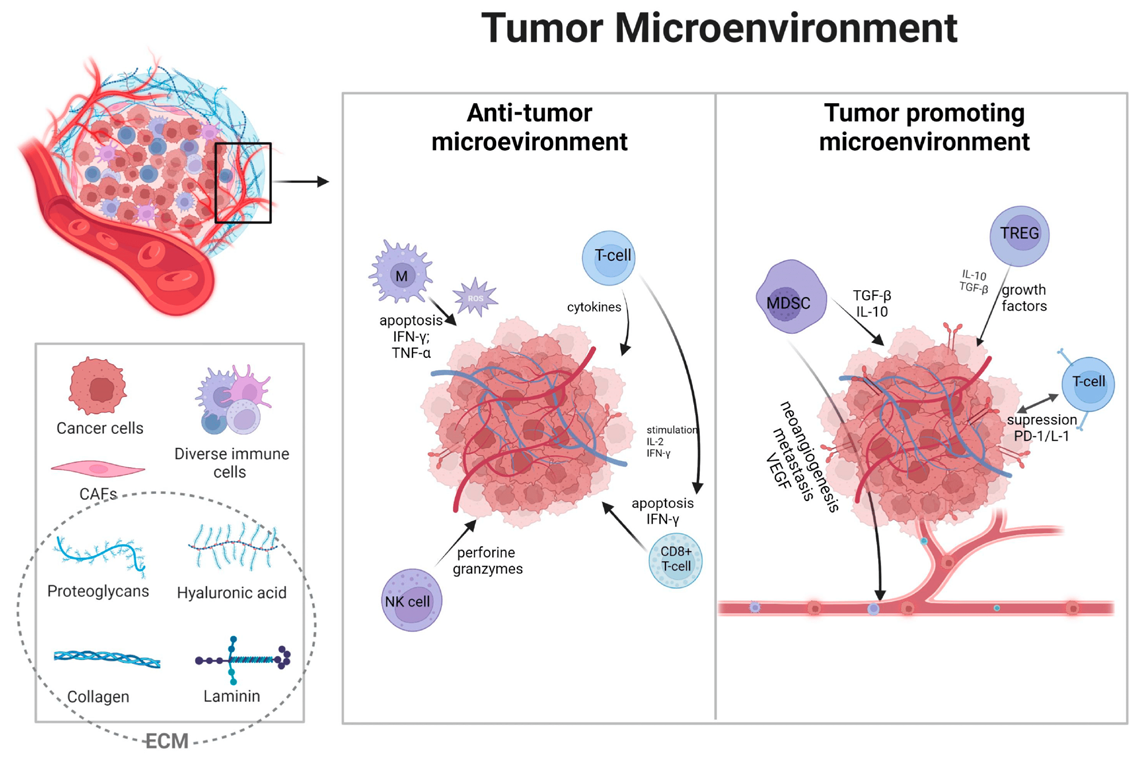
Figure 1: Tumour microenvironment showing immune cells trying to block and promote tumour growth (Figure collected from internet): Tumour microenvironment contains various types of cells including immune cells. T-cell, NK cell, CD8+ T-cell, M1 macrophages present in tumour try to block the tumour growth by generating anti-tumour immune responses. Other side, Treg cell, MDSC promotes tumour growth by creating immunosuppressive environment.
The role of T-cells, NK cells, macrophages etc. are well studied in context of tumour, but the role of B cells is still yet to be known and is a current topic in the field of research in tumour immunology.
We now summarize the functions of B cells in the field of tumour immunology which in turn can shed light upon the therapeutic strategies against cancer Figure 2.
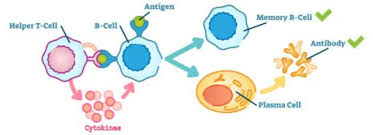
B cells or B lymphocytes originate from hematopoietic stem cells in the living system. They mainly play functions by producing different antibodies against antigens. B-cells are developed in bone marrow and later move into secondary lymphoid organ spleen for further maturation process. There are several subtypes of B cells are present like, transitional B-cells, mature B-cells, memory B-cells, plasma cells, etc. If an antigen (Ag) be recognized, then a naïve B cell enters the primary follicles of the lymph nodes or even other lymphoid tissues. B cells undergo extensive proliferation and form germinal centers or GCs, or even class switches to immunoglobulin G, A and/or E. In the GCs, some B cells further differentiate into plasma cells which in turn, can produce high affinity antibodies.
We know that B cells are an integral component of the adaptive immune system, but it is important to note that they can prominently affect anti-tumour responses and this science can be widely used for clinical applications and purposes. These functions are elucidated as follows-
AntigenGenerator
Upon antigen recognition, B cells start the process of antibody production by initiating 3 steps- • Proliferation
- Class switch recombination
- Plasma Cell Differentiation Meanwhile during the process, a large proportion of B cells are either in the resting phase, expressing IgM or not terminally differentiated into plasma cells. Interaction of antibodies with antigens serves as a great advantage to anti- tumour immunity.
As for instance, the antibodies secreted out by B cells may bind to tumour inducing antigens and amplify the adaptive immune response in triple negative breast cancer.
Antibody Production
B cells can lead to the promotion of anti-tumour immunity by 2 ways-
- Passing antigens to CD4+ and/or CD8+ cells
- Cross presentation of antigens to APCs B cells aid to the inhibition of tumour development in terms of functions. But it is important to note that recent scientific evidence suggests that B cells can also be immunosuppressive to the body, especially in the form of Breg or B regulatory cells.
In malignant forms of cancer, as well as in the case of infectious diseases and autoimmune disorders, B regulatory cells are the most prominent or in other words, the most dominating elements playing the role of immune response attenuation.
We can say that B regulatory cells are inhibitory effectors in the body- interacting with tumour tissues, as well as immune cells such as T cells, APCs, T regulatory cells as well as Myeloid Derived Suppressor Cells or MDSCs.
There are two opposing subsets of B cells-
- Breg or regulatory B cells, which inhibit immunity
- Beff or effector B cells, which promote immune responses
Regulatory B cells
The subset of B cells negatively regulating immune responses, have been termed as regulatory B cells. This subset has been recognized as an important component in the immune system in both mice and humans. B cells play an important role in various immune responses and diseases, which includes complex systemic autoimmune diseases. Interleukin-10 or IL-10 producing Breg cells are under investigation regarding their role in immune responses and diseases. Likewise, the role of Tumour Growth Factor- β or TGF-β for negative regulation by B cells has been found out.
IL-10 producing regulatory B cells (IL-10+ Breg cells): IL-10 is an anti-inflammatory cytokine that suppresses the production of pro-inflammatory cytokines in T cells and the function of dendritic cells (DCs) and macrophages. IL-10 is produced by various immune cells such as T cells, macrophages and B cells.
IL-10+ Breg cells have been proven to be immunoregulatory due to critical functions performed by them.
TGF-β producing regulatory B cells (TGF-β cells): TGF-β is a multi-functional cytokine which are not only immunoregulatory but also play a vital role in tissue fibrosis. It is because of TGF-β, that naïve CD4+ T cells are induced to differentiate into regulatory T cells and immature DCs are induced to tolerogenic DCs. Despite having T cells in the immune system, B cells have been recently found to produce TGF-β.
Effector B cells
Beff cells promote immune responses by the provision of several pro-inflammatory cytokines such as IL-2, IL-4, IL-6, IL-12, IL-17, IFN-γ, and TNF-α along with GM-CSF.
IFN-γ producing effector B cells have currently shown importance to immunological responses.
IFN-γ producing effector B cells (IFN-γ Beff cells): IFN-γ is a type-II IFN or interferon which plays important roles in innate immunity against intracellular infections and in adaptive immunoregulation.
IFN-γ has a vital role in strengthening innate immunity by the induction of antimicrobial factors as well as degradative pathways in other immune cells such as macrophages. It has been proved that B cells can also produce IFN-γ.
Peripheral B cells are identified as phenotypic surface markers. The immature transitional B cells mature within the microenvironment of the spleen into cells which form the backbone of adaptive humoral immunity.
These cells are listed as follows:
- Naive follicular B cells
- Germinal centre B cells
- Memory B cells
- Plasma blasts (secreting antibodies)
- Plasma cells These are the conventional B cells constituting the immune system. In addition to them, the immune system is comprised of marginal zone (MZ) B cells, which represent a category of memory B cell responding against blood borne pathogens. Henceforth, subsets of B cells have diverse phenotypes and each category of the B cells can perform a different function altogether which is related to anti-tumour response [1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13] Figure 3.
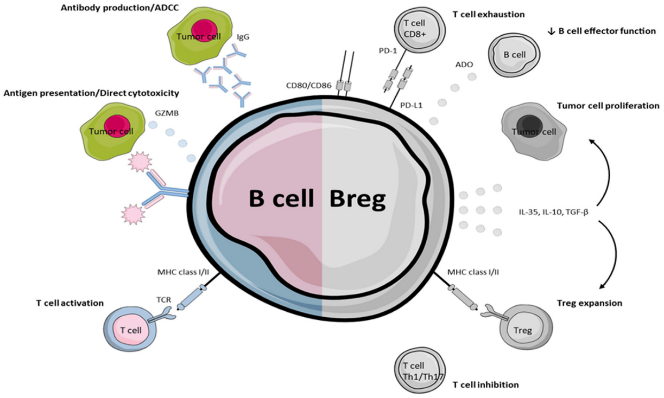
Figure 3: Functions of B cells and B regulatory cells (Breg cells): B- cells by producing antibodies against antigen and presenting antigen to T-cell helps in generation of immune response. Other side, Breg cells suppress immune responses by inhibiting effector T cell functions as well as promoting Treg cells generation. Picture courtesy: internet.
Isolation of PBMCs from blood
PBMCs refer to Peripheral Blood Mononuclear Cells which are certain immune cells, present in the blood.
Objective
Identification of B- Lymphocytes in cancer patient’s blood
Reagents & specialized equipment required
- 15ml conical tube
- 1.5ml conical tube
- Pipettes
- Pipette tips
- Blood from breast cancer patient and healthy individual
- 1x Phosphate buffer saline (PBS)
- Fluorophore Tag Antibodies
- Hi-sep (density of 1.077 g/mL)
- Biosafety cabinet
- Centrifuge machine/s
- BD FACS Verse Machine
Methodology
To identify B-lymphocytes, peripheral blood was collected from breast cancer patients and healthy individuals respectively. After that, blood samples were processed to collect peripheral blood mononuclear cells (PBMCs).
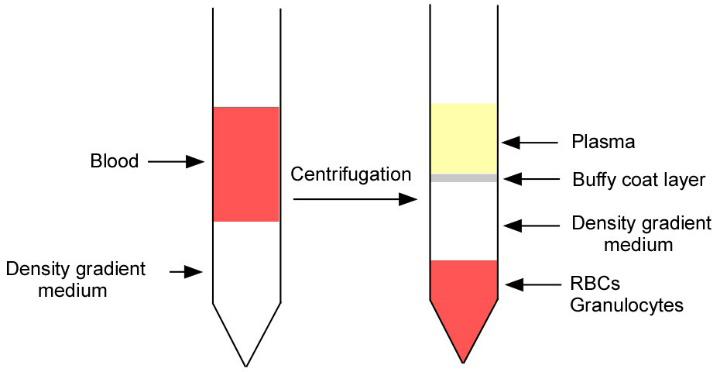
PBMC isolation is commonly done via density gradient centrifugation. For this, a density gradient medium, known as Hi-Sep was taken to a fresh 15 ml conical tube and gently layer the blood on top of the density gradient medium (Hi- Sep: Blood ratio= 1:1). Then density gradient centrifugation was done at 1000xg for 40 minutes at room temperature in a centrifuge.
After that the buffy coat layer obtained (containing PBMC) was carefully harvested to a new fresh 15ml conical tube and washed. For this 1x phosphate buffer saline (PBS) was added into it, mixed and then further subjected to centrifuge at 3000xg for 3 minutes at room temperature.
Carefully, supernatant is removed to leave a PBMC pellet in the base of the tube. Then adding 1ml fresh 1x PBS, followed by mixing is carried out with gentle pipetting and keeping the sample for further use.
Observation
After density gradient centrifugation four layers are formed-
- Plasma
- Buffy coat layer
- Density gradient medium layer
- RBCs and granulocytes The buffy coat layer contains PBMCs, in which lymphocytes are present Figure 4.
For this, PBMC was isolated from each condition and was incubated with anti-human CD19-FITC (Fluorescein isothiocyanate) tag antibody for 30 mins at 4°C. After that, samples were washed with 1x PBS at 3000 x g for 3mins.
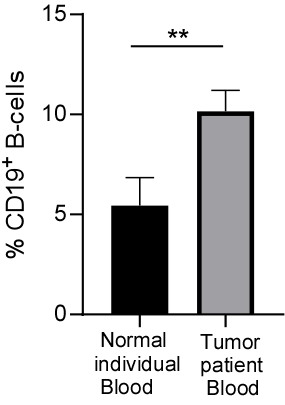
Figure 5: A graphical plot showing the rise in count of B cells in cancer patients as compared to that in a normal healthy individual. The representative bar plot is showing changes in percentage of B-cells between normal and breast tumour patient’s blood (n=3). Unpaired student’s t-test was used to evaluate statistical significance of the data using Graph Pad prism8 software.
Frequency of various B-cell type
After comparing total B cell count between a cancer patient and a normal healthy individual, we now study the different subtypes of B cells. After observing total B-cell percentage increases in tumour patients, we investigated different B-cell subtypes like, memory
Observation
Total B-cell percentage significantly increases in breast tumour patients’ blood compared to healthy individual’s blood Figure 5.
B-cell (CD19+CD24+posCD38-neg), transitional B- cell (CD19+CD24hiCD38hi), plasma cell (CD19+CD24- negCD38+pos), and mature B-cell (CD19+CD24intCD38int) in healthy and breast tumour patient’s blood respectively. For this, we take the isolated PBMC sample from each condition and incubate them with anti-human CD19-FITC (Fluorescein isothiocyanate), CD24-PE-Cy7 (Phycoerythrin-
Cyanine7), and CD38-APC (Allophycocyanin) tag antibodies for 30 minutes at 4°C temperature. After that, samples were washed with 1x PBS at 3000 x g for 3mins. Then carefully supernatant is discarded and the cell pellet is dissolved in 500µl PBS. Unstained and single tag sample was used as control for proper gating during data acquisition in BD FACS Verse flow-cytometry machine.
Observation
Percentage of memory and plasma B-cells was significantly lower in cancer patient blood compare to healthy individual blood, but the transitional B-cells number significantly increases in patients with breast cancer than the healthy individual. Mature B-cell population shows no significant changes between healthy and tumour patient blood Figure 6.
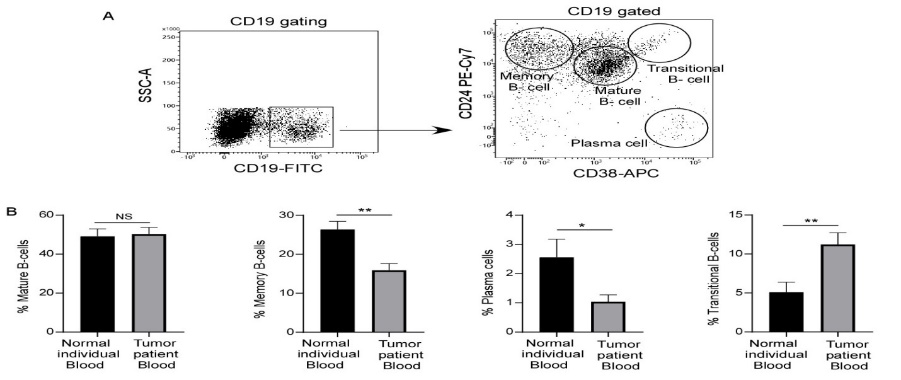
Figure 6: Identification of B-cell subtypes. (A) Representative flow-cytometry plot showing different B-cell subtypes. (B) The representative bar plot showing changes in percentage of important B-cell subtypes like mature, memory, plasma, and transitional B-cells (from left to right) between normal and breast tumour patient’s blood (n=3). Unpaired student’s t-test was used to evaluate statistical significance of the data using GraphPad prism8 software.
Conclusion
B cells are an important component of our immune system. They generate immune responses by producing antibodies. They also help in developing T-cell mediated immune responses against pathogens. The role B-cells in the field of cancer biology is relatively less established. Recent findings highlight the fact that cancer patients have increased number of total B-cell population as compared to that in a healthy individual. We all know that B-cells play a protective part in our body by producing antibodies against diseases. Therefore, it would not be out of context if we hypothesize that this increased B-cells might target the cancer cells by mounting anti-tumour immune responses and resultantly can prevent tumour growth. But in reality, the underlying biology is more complex. In-depth investigation of B-cell subtypes indicates significant alteration in B-cell subtypes between normal and cancer patient blood.
It is found that the memory B-cell as well as plasma B-cell population, which are mainly responsible for generating immune responses by producing different types of antibodies, decreases in blood-stream of the breast cancer patients when compared to normal individuals. Moreover, another B-cell subtype, transitional B-cells; significantly increases in cancer patients’ blood than healthy individuals. Interestingly, literature study revealed that the transitional B-cell populations which produce IL10 and suppress, the immune responses are called B-regulatory cells. So, mining all these observations one can conclude that during breast cancer onset, immunosuppressive Breg cell population increases as well as the effector B-cell subtypes like, plasma and memory B-cells are decreased. As a result, anti-tumour immune responses are found to be decreased leading to lower survival of the breast cancer patients.
References
-
Gonzalez H Catharina H, Zena Werb (2018) Roles of the immune system in cancer. Genes & development 32(19- 20): 1267-1284.
-
Visser KED, Joyce JA (2023) The evolving tumour microenvironment. Cancer Cell 41(3): 374-403.
-
Galli F, Aguilera JV, Palermo B, Svetomir NM, Paola N, et al (2020) Relevance of immune cell and tumour microenvironment imaging. J Exp Clin Cancer Res 39: 1-21.
-
Wang J, Danyang L, Huaixing C, Bo G (2019) Crosstalk between cancer and immune cells. Cancer Medicine 8(10):4709-4721.
-
Bates JP, Roshanak D, Laundette J, Tonya JW, (2018) Mechanisms of immune evasion in breast cancer. BMC Cancer 18:1-14.
-
Le Bien TW, Tedder TF (2008) B lymphocytes: how they develop and function. Blood 112: 1570-1580.
-
Shen M, Qian S, Jian W, Wei P, Xiubao R (2016) Positive and negative functions of B lymphocytes in tumours. Oncotarget 7: 55828-55839.
-
Hoffman W, Lakkis FG, Chalasani G (2016) B Cells, Antibodies, and More. Clin J Am Soc Nephrol 11: 137- 154.
-
Ichwaku R, Donghwan J, Jena EM, Anusha M, Hemanth KP, et al (2022) Role of B cells as antigen presenting cells. Front Immunol 13:954936.
-
Takashi M (2019) Regulatory and effector B cells: Friends or foes? J Dermatological Science 93: 2-7.
-
Chekol Abebe E, Tadesse AD, Teklie MA, Nega DB, Assefa AT, et al (2021) The Role of Regulatory B Cells in Health and Diseases. J Inflamm Res 14:75-84.
-
Paul AB, Lina YN, Fabian F, David AI, Michael RE (2010) CD19+CD24hiCD38hi B Cells Exhibit Regulatory Capacity. Immunity 32: 129-140.
-
Wei WW, Xiang LY, Hui C, Guo HX, Yan HM, et al (2015) CD19+CD24hiCD38hiBregs in gastric cancer. Oncotarget 6: 33486-33499.
- Cancer Diagnosis from RNA Sequence of Blood Cells by Using AI
- Field Cancerization in Oral Cavity, Case Report and Review of Literature. Oncologic Program Salud Integral Hospital, Managua, Nicaragua
- A Case Report of a Breast Cancer Patient Developing Pneumonitis as a Result of Abemaciclib Therapy
- Immune Checkpoint Therapeutics for Today’s Fight and Beyond
- The Amalgamated Sophomore-Gonadoblastoma
- Festered and Fenced-Lymphoepithelial Carcinoma Lung