Field Cancerization in Oral Cavity, Case Report and Review of Literature. Oncologic Program Salud Integral Hospital, Managua, Nicaragua
Medrano FJ¹*, Castro AC², Padilla Rᶾ, Matus R⁴, Quezada CM⁵ and Ubilla V⁶
¹Head and Neck surgeon, Oncologic Program Salud Integral Hospital, Nicaragua ²Oral Pathologist and Oral Surgeon, Chairman Linda Vista Medical Clinic, Nicaragua ³Maxilofacial Surgeon and Prosthetic Rehabilitation, Staff Oncologic Program Salud Integral Hospital, Nicaragua ⁴Radiologist, Chairman of X ray Medical Centre, Nicaragua ⁵Hematopatologist, Chairman of Pathology Department, Salud Integral Hospital, Nicaragua ⁶Dentist, Staff Linda Vista Medical Clinic, Nicaragua
Introduction
Oral cancer is the most common in India [1]. Europe and United State data systems reported an increase for two decades [2]. Goldemberg reported a new trend of tongue cancer epidemiology in Brazil [3] such as was reported prior by Jia Hui, et al [4]. Tobacco products are generally involved as risk factor in oral cancer [5, 6].
Human papilloma virus (HPV) infection may be associated with oropharyngeal cancer and oral cavity [7, 8, 9]. Several premalignant lesions maybe develop a cancer [10, 11, 12, 13]. The knowledge of molecular and genetic aspects has allowed us to define a new term: Oral Potentially Malignant Disorders (OPMD) [14] Oral cancers are typically preceded by OPMD.
Different methods assessment, have been used to identify the risk of progress of OPMD to cancer. Since clinical inspection, to advanced technologic methods [15, 16, 17, 18]. The genetic loss of heterozygosity (LOH) is the better biomarker for this, but the high cost avoids the use into day to day [19, 20, 21]. Slaughter in 1953 proposed the field cancerization. This hypothesis was reproduced by several experimental models [22, 23].
The main is to describe a patient with multiples oral premalignant lesion and squamous cell carcinoma areas concomitant and review of literature.
A 74-year-old female reported a burning sensation and pain of superior left gingiva for three years ago, followed by a new ulcer formation near of gingiva in the same location an ulcer.
She visited a doctor and received treatment without relief and appear a new lesion in mucosa of cheek and behind of the third molar. She has no history of tobacco and alcohol, but she suffers from diabetes disease for 30 years. She weighs 53.8 Kgs and she is 1.63 meters tall.
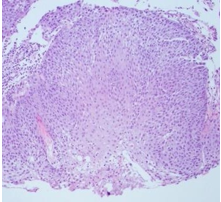
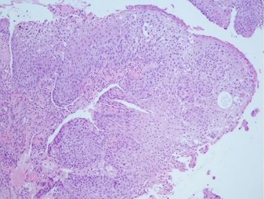
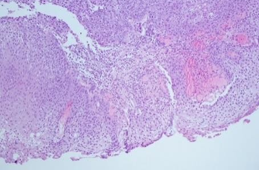
Intraoral examination: Erythroplasia lesion involving right and left buccal mucosa, upper left gingiva and ulcer in cheek (1.5 x 2 cm) she has retromolar trigone lesion Figure 1-4.




Routine blood investigations revealed normal tests and HIV was negative. Radiologic assessment with CT scan, chest radiograph and abdominal ultrasound reported as normal. The incisional biopsy was done of left mucosa and retromolar area. Invasive squamous cell carcinoma of oral mucosa and field cancerization was diagnosed. Figure 5-7 HPV P16 was negative.
Discussion
The oral cancer is relationship with tobacco [24, 25]. However, several papers have reported that other agents are really protooncogenic that the end did not permit the grow cell control.
There are patients with specific conditions that predispose them to this alteration; to mention a few Examples: the spoilage of the immune system as it occurs during aging, chronic diseases and biologic agents, rheumatological disease. Our patient has no tobacco history but she belongs to the elderly. The constant stimulation of some agents can generate to loss of adequate inflammatory responses to them [26]. The loss of this balance can lead to the development of autoimmune diseases, infectious and cancer [27, 28, 29].
Another aspect related to the spoilage of immunity due to aging is the natural involution of the thymus. A decrease in the production of immune system cell has been reported, which also predisposes them to infections, autoimmune diseases and cancer. The subject of autoimmune diseases Medrano et al reported a series of cases of patients with rheumatic disease that developed thyroid cancer similar to the study published by Antonelli [30, 31, 32, 33].
After the history of diabetes in our case, is a well known the autoimmune pathogenesis of this disease. The chronic inflammatory state in them generates several antibodies that have been detected as a autoimmune event [34, 35, 36]. Another different aspect in this group of patients is the phenotypic patients without obesity and older than 65 years as our case similar to reported by Turner et al [37, 38, 39].
Oral potentially malignant disorders (OPMD) have made it possible to homogenize the nomenclature of lesions in the oral cavity. The main objective is to allow early detection of lesions that can potentially progress to carcinoma [40]. The workshop held in London 2005, recommended the use of the term [41].
Tobacco continues to be the most important risk factor in the transformation of an OPMD. Although there are others of lower risk, which must be considered: local infections, chronic trauma, HPV among others. [42, 43] The sequence of cellular changes that end in carcinoma are very similar, leukoplakia is an example, to cite the most common induced by tobacco. However, our patient has erythroplakia, which are lesions with a higher risk of transformation to carcinoma in the context of diabetes and aging without tobacco history [44, 45, 46].
Schepman reported that risk of transformation of leukoplakia can be as low as 1.2% however, associated with other cellular changes it could be up to 14.5 % [47, 48, 49]. On the other hand, dysplasias are more common in erythroplaias, mainly in old patients. The rate of malignant transformation rate is 14.3%–66.7%. The biopsy report of our case shows a focus of severe dysplasia close an invasive carcinoma as reported by Villa and Peter [50, 51, 52].
Early detection of any OPMD requires a histological biopsy to classify the risk of transformation to cancer. Adequate clinical training in this subject is the first step, even if its percentages of sensitivity and specificity are very low [53, 54]. On the other hand, several studies using high technology are appearing every day, allowing for earlier diagnosis in the high-risk patients. Autofluorescence imaging (AFI), In vivo microscopy IVM, Optical coherence tomography, Reflectance confocal microscopy, Multiphoton microscopy [55, 56, 57, 58, 59, 60]. These technological tools have the disadvantage of having high costs and are not available in our country.
Molecular biology has made it possible to identify similar genetic alterations in OPMD and cancer, in such a way that they have become the main biomarkers that identify the patient at high risk of transformation [61, 62].
The development of a second primary tumour in the head and neck could be as high as 15% and as low as reported by Medrano at 1.4%. [63]. Microsatellite marker term has a gene expression that could have macroscopic, microscopic manifestations or only genetic. Boland reported that 30% of cells with hyperplasia’s shared the same genetic changes in areas with cancer. This has also been identified in head and neck cancer. In our case there are lesions with severe dysplasia close of squamous cell carcinoma oral mucosa [64] in 1953 Slaughter had already proposed this hypothesis: field cancerization, which continues to be used today.
Conclusion
The early detection is the main goal in front to OPMD, the first step in patients with or without tobacco and alcohol exposition. There are others patient´s risk factor that allow to develop it. The histological biopsy will help to identify the progression risk to cancer and allow establish the follow-up or the most appropriate therapeutic decision.
References
-
Sankaranarayanan R, Masuyer E, Swaminathan R, Ferlay J, Whelan S (1998) Head and neck cancer: A global perspective on epidemiology and prognosis. Anticancer Res 18: 4779-4786.
-
Gillison ML (2007) Current topics in the epidemiology of oral cavity and oropharyngeal cancer. Head & Neck 29(8).
-
Goldemberg DC, Lima LH, Spindola H, Cristina DMA, Santos LC (2018) Tongue cancer epidemilogy in Brazil: Incidence, morbidity and mortality. Head & Neck 40:(8): 1834-1844.
-
Hui J, Gopalakrishna N, Min-Han T, Gustaf E (2016) Changing epidemiology or oral squuamous cell carcinoma of the tongue: a global study. Head & Neck 39(2): 297-304.
-
(2007) IARC Working Group on the Evaluation of Carcinogenic Risks to Humans. Smokeless tobacco and some tobacco-specific N-nitrosamines. IARC Monogr Eval Carcinog Risks Hum 89: 1-592.
-
Boffetta P, Hecht S, Gray N, Gupta P, Straif K (2008) Smokeless tobacco and cancer. Lancet Oncol 9: 667-675.
-
Rosemaruy G, Ralph BS, Andrew ON (1998) Humam Papillomavirus and head and neck cancer : Epidemiology and molecular biology. Head &Neck20(3): 250-267.
-
Bradford C(2000) Human Papillomavirus Infection In “Young” Versus “Old” Patients with Squamous Cell Carcinoma of The Head And Neck.
-
Ch J (2007) Role of Human Papillomavirus In The Etiology Of Head And Neck.
-
Aroquiadasse M, Daniel MJ, Srinivasan SV, Jimsha VK (2016) Correlation of degree of dysplasia in potentially malignant disorders with tobacco use: A cross-sectional study. Clin Cancer Investig J 5: 398.
-
Murti PR, Bhonsle RB, Pindborg JJ, Daftary DK, Gupta PC, et al. (1985) Malignant transformation rate in oral submucous fibrosis over a 17-year period. Community Dent Oral Epidemiol 13: 340-341.
-
Mehta FS, Pindborg JJ, Gupta PC, Daftary DK (1969) Epidemiologic and histologic study of oral cancer and leukoplakia among 50,915 villagers in India. Cancer 24: 832-849.
-
Reichart PA, Philipsen HP (2005) Oral erythroplakia-A review. Oral Oncol 41: 551-561.
-
Sarode SC, Sarode GS, Tupkari JV (2014) Oral potentially malignant disorders: A proposal for terminology and definition with review of literature. Journal of Oral and Maxillofacial Pathology.
-
Forman MS, Chuang S-K, August M (2015) The accuracy of clinical diagnosis of oral lesions and patient- specific risk factors that affect diagnosis. J Oral Maxillofac Surg 73: 1932-1937.
-
Macey R, Walsh T, Brocklehurst P (2015) Diagnostic tests for oral cancer and potentially malignant disorders in patients presentingwith clinically evident lesions. Cochrane Database Syst Rev.
-
Poh CF, Zhang L, Anderson DW (2006)Fluorescence visualization detection of field alterations in tumor margins of oral cancer patients. Clin Cancer Res 12: 6716-6722.
-
Matsui T, Mizuno H, Sudo T (2017) Non-labeling multiphoton excitation microscopy as a novel diagnostic tool for discriminating normal tissue and colorectal cancer lesions. Sci Rep 7: 6959.
-
Li Mao, El-Naggar, Papadimitrakopoulou V, Shin D, Shin H, et al. (1998) Hong Phenotype and Genotype of advanced premalignant head and neck lesions after chemopreventive therapy. Journal of the National Cancer Institute 90(20).
-
Knudson AG (1985) Hereditary cancer, oncogenes, and antioncogenes. Cancer Res 45: 1437-1443.
-
Riet P, Nawroz H, Hruban RH, Corio R, Tokino K, et al. (1994) Frequent loss of chromosome pp: 21–22 early in head and neck cancer progression. Cancer Rev 54: 1156- 1158.
-
Slaughter, DP, Southwick HW, Smejkal, W (1956) Field cancerization in oral stratified squamous epithelium: clinical implications of multicentric origin. Cancer (Phila.) 6: 963-968.
-
Califano J, Riet P, Westra W, Nawroz H, Clayman G, et al. (1996) Genetic progression model for head and neck cancer: implications for field cancerization. Cancer Res 56: 2488-2492.
-
Znaor A, Brennan P, Gajalakshmi V, Mathew A, Shanta V, Varghese C, et al. (2003) Independent and combined effects of tobacco smoking, chewing and alcohol drinking on the risk of oral, paryngeal and esophageal cancers in Indian men. Int J Cancer 105: 681-686.
-
He QQ, Wong TW, Du L, Jiang ZQ, Yu TS, et al. (2011) Environmental tobacco smoke exposure and Chinese schoolchildren’s respiratory health: A prospective cohort study. Am J Prev Med 41: 487‑493.
-
Wick G, Berger P, Jansen-Durr P, Grubeck-Loebenstein B (2003) A Darwinian evolutionary concept of age- related diseases. Exp Gerontol 38: 13-25.
-
Dejaco C, Dufner C, Schirmer M (2006) Are regulatory T-cells linked with aging? Exp Gerontol 41: 339-345.
-
Raynor J, Lages CS, Shehata H, Hildman DA, Chougnet CA (2012) Homeostasis and function of regulatory T cells in aging. Curr Opin Immunol 24: 482-487.
-
Vadasz Z, Haj T, Kessel A, Toubi E (2013) Age-related autoimmunity. BMC Medicine 11: 94.
-
Palmer S, Albergante L, Blackburn CC, Newman TJ (2018) Thymic involution and rising disease incidence with age. Proc Natl Acad Sci U S A 115: 1883-1888.
-
Kooshesh K, Brody FH, Sykes DB, Gustafsson K, David T, et al. (2023) Health Consequences of Thymus Removal in Adults. N Engl J Med 389: 406- 417.
-
Medrano F, Martinez AM, Sandino S, Matus R, Carmona G et al. (2020) Thyroid Cancer in Patients with Rheumatic Diseases. J Endocrinol 4(1): 000147.
-
Antonelli A, Mosca M, Fallahi P, Neri R, Ferrari SM, et al. (2010) Thyroid cancer in Systemic Lupus Erithematosus. A case- control study. J Clin Endocrinol Metabol 95(1): 314-318.
-
Wentworth JM, Fourlanos S, Harrison LC (2009) Reappraising the stereotypes of diabetes in the modern diabetogenic environment. Nat Rev Endocrinol 5: 483- 489.
-
Fourlanos S (2006) A clinical screening tool identifies autoimmune diabetes in adults. Diabetes Care 29: 970- 975.
-
Donath MY, Shoelson SE (2011) Type 2 diabetes as an inflammatory disease. Nat Rev Immunol 11: 98-107.
-
Pietropaolo M (2000) Evidence of islet cell autoimmunity in elderly patients with type 2 diabetes. Diabetes 49: 32- 38.
-
Turner R, Stratton I, Horton V, Manley S, Zimmet P, et al (1997) UKPDS 25: autoantibodies to islet-cell cytoplasm and glutamic acid decarboxylase for prediction of insulin requirement in type 2 diabetes. UK Prospective Diabetes Study Group. Lancet 350: 1288-1293.
-
Itariu BK, Stulnig TM (2014) Autoimmune Aspects of Type 2 Diabetes Mellitus -A Mini-Review Gerontology 60:189-196.
-
Sarode SC, Sarode GS, Karmarkar S, Tupkari JV (2012) Oral (mucosal) potentially malignant disorders. Oral Oncol 48: e35‑e36.
-
Warnakulasuriya S, Johnson NW, van der Waal I (2007) Nomenclature and classification of potentially malignant disorders of the oral mucosa. J Oral Pathol Med 36: 575‑580.
-
Sarode SC, Sarode GS, Karmarkar S, Tupkari JV (2011) A new classification of potentially malignant disorders of the oral cavity. Oral Oncol 47: 920‑921.
-
Isaäc van derWaal (2018) Historical perspective and nomenclature of potentially malignant or potentially premalignant oral epithelial lesions with emphasis on leukoplakia-some suggestions for modifications. Oral and Maxillofacial Pathology. 125: 577–581.
-
Ekanayaka RP, Tilakaratne WM (2016) Oral submucous fibrosis: review on mechanisms of malignant transformation. Oral Surg Oral Med Oral Pathol Oral Radiol 122: 192-199.
-
Syrjänen S, Lodi G, Bültzingslöwen IV, Aliko A, Arduino P, et al. (2011) Human papillomaviruses in oral carcinoma and oral potentially malignant disorders: a systematic review. Oral Dis. 17: 58- 72.
-
Porter S, Gueiros LA , Leão JC, Fedele S (2018) Risk factors and etiopathogenesis of potentially premalignant oral epithelial lesions. Oral Surg Oral Med Oral Pathol Oral Radiol 125: 603–611.
-
Amagasa T, Fujii E, Suzuki T, Yamashiro M, Ogura I et al. (1999) Clinical characteristics of precancerous lesions and early squamous cell carcinoma in the oral cavity. J Japan Society Oral Tumors 11: 357–363.
-
Schepman KP, van der Meij EH, Smeele LE, van der Waal (1998) Malignant transformation of oral leukoplakia : a follow-up study of a hospital-based population of 166 patients with oral leukoplakia from The Netherlands. Oral Oncol 34: 270-275.
-
Amagasa T, Yamashiro H, Ishikawa H (2006) Oral Leukoplakia Related to Malignan Transformation. Oral Science International p: 45-55
-
Villa A, Villa C, Abati S (2011) Oral cancer and oral erythroplakia: An update and implication for clinicians. Aust Dent J 56: 253‑256.
-
Reichart PA, Philipsen HP (2005) Oral erythroplakia- a review. Oral Oncology 41: 551-561.
-
Awadallah M, Idle M, Patel K, Kademani D (2018) Management update of potentially premalignant oral epithelial lesions. Oral Surg Oral Med Oral Pathol Oral Radiol 125: 628-636.
-
Epstein JB, Güneri P, Boyacioglu H, Abt E (2012) The limitations of the clinical oral examination in detecting dysplastic oral lesions and oral squamous cell carcinoma. J Am Dent Assoc 143: 1332-1342.
-
Forman MS, Chuang SK, August M (2015) The accuracy of clinical diagnosis of oral lesions and patient- specific risk factors that affect diagnosis. J Oral Maxillofac Surg 73: 1932-1937.
-
Poh CF, Anderson DW, Durham JS, Chen J, Berean KW et al. (2015) Fluorescence visualization–guided surgery for early-stage oral cancer. JAMA Otolaryngol Neck Surg 142: 209-216.
-
Pierce MC, Schwarz RA, Bhattar VS, Mondrik S, Williams MD et al. (2012) Accuracy of in vivo multimodal optical imaging for detection of oral neoplasia. Cancer Prev Res (Phila) 5: 801-809.
-
Tsai MT, Lee CK, Lee HC, Chen HM, Chiang CP et al. (2009) Differentiating oral lesions in different carcinogenesis stages with optical coherence tomography. J Biomed Opt 14: 44028.
-
Olsovsky C, Hinsdale T, Cuenca R, Cheng YL, Wright YM et al. (2017) Handheld tunable focus confocal microscope utilizing a double clad fiber coupler for in vivo imaging of oral epithelium. J Biomed Opt 22: 56008.
-
Pal R, Edward K, Ma L, Qiu S, Vargas G (2017) Spectroscopic characterization of oral epithelial dysplasia and squamous cell carcinoma using multiphoton autofluorescence micro-spectroscopy. Lasers Surg Med 49: 866-873.
-
Yang EC, Melody BST, Richard AS, Rebecca RRk, Ann MG, Nadarajah V (2018) Noninvasive diagnostic adjuncts for the evaluation of potentially premalignant oral epithelial lesions: current limitations and future directions. Oral Surg Oral Med Oral Pathol Oral Radiol 125: 670-68.
-
Reed AL, Califano J, Cairns P, Westra WH, Jones RM, et al. (1996) High frequency of p16 (CDKN2/MTS-1/INK4A) inactivation in head and neck squamous cell carcinoma. Cancer Res 56: 3630-3633.
-
El-Naggar AK, Lai S, Clayman G, Lee JK, Luna MA, et al. (1997) Methylation, a major mechanism of p16/CDKN2 gene inactivation in head and neck squamous carcinoma. Am J Pathol 151: 1767-174.
-
Medrano FJ, Perez G Second primary tumour in patients with head and neck cancer, February 2003-July 2015, Salud Integral Hospital, Managua, Nicaragua-P507-9ᵀᴴ International conference on head and neck cancer, July 16-20, 2016 Seattle, Washington US.
-
Boland CR, Sato J, Appelman HD, Bresalier RS, Feinberg AP (1995) Microallelotyping defines the sequence and tempo of allelic losses at tumour suppressor gene loci during colorectal cancer progression. Nat. Med 1: 902- 909.
- Cancer Diagnosis from RNA Sequence of Blood Cells by Using AI
- Identification of B Lymphocytes in Cancer Patient’s Blood
- A Case Report of a Breast Cancer Patient Developing Pneumonitis as a Result of Abemaciclib Therapy
- Immune Checkpoint Therapeutics for Today’s Fight and Beyond
- The Amalgamated Sophomore-Gonadoblastoma
- Festered and Fenced-Lymphoepithelial Carcinoma Lung