Autosomal Dominant Hypophosphatemic Rickets: A Case ReportÂ
<p class="MsoNormal" style="margin-bottom: .0001pt; text-align: justify; text-justify: inter-ideograph; line-height: 150%;"><span lang="EN-GB" style="font-size: 10.0pt; line-height: 150%; font-family: 'Cambria','serif'; mso-ascii-theme-font: major-latin; mso-hansi-theme-font: major-latin; mso-ansi-language: EN-GB;">Autosomal dominant hypophosphatemic <span class="highlighthighlighted">rickets (ADHR) </span>is characterized by isolated renal phosphate wasting, hypophosphatemia, and inappropriately normal 1,25-dihydroxyvitamin D3 (calcitriol) levels. We present </span><span style="font-size: 10.0pt; line-height: 150%; font-family: 'Cambria','serif'; mso-ascii-theme-font: major-latin; mso-hansi-theme-font: major-latin;">a 3 y old girl with short stature and metaphases dysplasia. <span style="color: black;">Plasma phosphorus was low, with high levels of alkaline phosphatase and parathormone. She has great loss of phosphorus in urine. Amino acids, bicarbonate, </span>serum 1,25-dihydroxyvitamin D3 <span style="color: black;">showed normal levels. </span>Skeletal x-ray revealed signs of rickets particularly in the wrist. The DNA study <span style="color: black; background: white;">detected missense mutations R179Q in</span></span> <span style="font-size: 10.0pt; line-height: 150%; font-family: 'Cambria','serif'; mso-ascii-theme-font: major-latin; mso-hansi-theme-font: major-latin;">FGF23 gene</span><span lang="EN-GB" style="font-size: 10.0pt; line-height: 150%; font-family: 'Cambria','serif'; mso-ascii-theme-font: major-latin; mso-hansi-theme-font: major-latin; mso-ansi-language: EN-GB;">. </span><span style="font-size: 10.0pt; line-height: 150%; font-family: 'Cambria','serif'; mso-ascii-theme-font: major-latin; mso-hansi-theme-font: major-latin;">We started treatment with calcitriol and Joulie solution with recovered of her growth, increasing 10.5 cm in 13 months. Her varus knees normalized during this period. The rickets signs on the x-ray become better. No family history was found. FGF23 gene of parents were negative. </span><span class="highlighthighlighted"><span lang="EN-GB" style="font-size: 10.0pt; line-height: 150%; font-family: 'Cambria','serif'; mso-ascii-theme-font: major-latin; mso-hansi-theme-font: major-latin; mso-ansi-language: EN-GB;">The risk for next pregnancy is low because our case was a sporadic presentation.</span></span></p>
Introduction
Autosomal dominant hypophosphatemic rickets (ADHR) is characterized by isolated renal phosphate wasting, hypophosphatemia, and inappropriately normal 1,25-dihydroxyvitamin D3 (calcitriol) levels. The prevalence is: <1 / 1 000 000. In childhood onset, the patients showed between 1 to 3 years: short stature, rickets, lower limb deformities, renal phosphate wasting, decreased tubular maximum for phosphate reabsorption per glomerular filtration rate (TmP/GFR).
Laboratory findings included: hypophosphatemia, inappropriately normal serum 1,25-dihydroxyvitamin D3, increased serum alkaline phosphatase, increased serum alkaline phosphatase, normocalcemia, normal serum parathyroid hormone (PTH), with exception of sporadic cases in which PTH is elevated. Rarely, patients with childhood-onset may lose the renal phosphate-wasting defect. FGF23 gene confirmed the diagnosis. Treatment with vitamin D and phosphate is effective. Calcitriol is administered in two doses per day (10 to 20 ng/kg per dose). Phosphorus is administered in four to five doses that are equally spaced throughout the 24-hour period; the starting dose is 40 mg of elemental phosphorus/kg per day. In our experience, a nighttime’s dose is important to achieve satisfactory results. Some catch-up growth should be noticeable within the first year of therapy. If this does not occur despite good compliance, the daily phosphorus dose should be increased in steps of 250 mg to 500 mg up to a maximum of 3500 mg/day. Children who cannot take pills can receive phosphorus supplementation in the form of Joulie's solution (155 g of dibasic anhydrous sodium phosphate and 64 g of phosphoric acid 85 percent per litre solution, corresponding to 50 mg/mL of elemental phosphorus).
Case Report
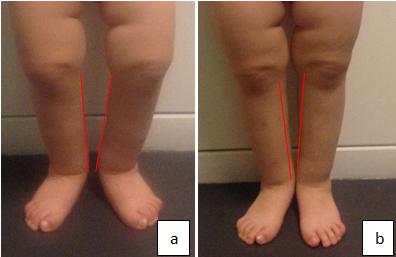
A 3 y old girl was sent to our pediatric outpatient because of short stature and suspect of metaphases dysplasia. She is the only child of young and unrelated parents. The patient stature was on 50 percentile until two years of age and after decreased to less than 5 percentile with weight and head circumference over 95 percentile. She also showed varus knees. The growth velocity was normal at the first year of life and increased only 5.5 cm at the second year. She has normal skills for age. The analyses showed normal karyotype and thyroid function. Plasma phosphorus was low, with high levels of alkaline phosphatase and parathormone. She has great loss of phosphorus in urine. Amino acids, bicarbonate, serum 1,25-dihydroxyvitamin D3 showed normal levels. Skeletal x-ray revealed signs of rickets particularly in the wrist (Figure 1).

Showed metaphyseal widening and signs of bone rarefaction We started treatment with calcitriol and Joulie solution with recovered of her growth, increasing 10.5 cm in 13 months. Her varus knees normalized during this period. (Figure 2) The rickets signs on the x-ray become better.
Discussion
Patients frequently present with bone pain, rickets, and tooth abscesses. In contrast to X-linked dominant hypophosphatemic rickets (XLH), ADHR shows incomplete penetrance, variable age at onset (childhood to adult), and resolution of the phosphate-wasting defect in rare cases. Other forms of hypophosphatemic rickets include an autosomal recessive forms, ARHR1, caused by mutation in the DMP1 gene on chromosome 4q21, and ARHR2, caused by mutation in the ENPP1 gene on chromosome 6q22- q23. An X-linked dominant form is caused by mutation in the PHEX gene, and an X-linked recessive form is caused by mutation in the CLCN5 gene. Our case after one year of treatment responded well to association of calcitriol and Joulie solution. The most two important clinical respond was the normalization of varus knees and catch-up growth velocity. The laboratory and radiologic changes will take time to normalize. The child onset has much better prognosis than in the adult form. There are reports that the final stature will achieve the target growth for the mean parental height. No family history was found. The risk for next pregnancy is low because our case was a sporadic presentation.
References
-
Vasconcellos AG, Sousa DAL, Carneiro FB, Rios GP, Santos LS, et al. (2010) Uncommon forms of rickets in childhood: a case report. Gazeta Médica da Bahia 79: 111-116.
-
Jones LV, Domingo MM (2013) Hereditary hypophosphatemic rickets. Bol Med Hosp Infant Mex 70(6): 421-431.
- Shaping Healthy Futures: Pediatric Endocrine Breakthroughs of 2025
- Precision Medicine in Obesity: Customizing Treatment for 2025
- The Thyroid Revolution: How 2025 is Redefining Hormone Health
- Editorial- Targeting Immunometabolism for Generating Innovative Therapies for Cancer
- Current Knowledge of Chickenpox
- Correlation of Preinjection Values of Gonadotropins and Estradiol Level with Clinical and Radiologic Evidence of Sufficient Pubertal Suppression in Girls with Central Precocious Puberty