The Relevance of Insulin-Like Growth Factor-Binding Protein- 3 Concentrations According to Optimal Cut-Points as a Screening Test for Diagnosis of Growth Hormone Deficiency
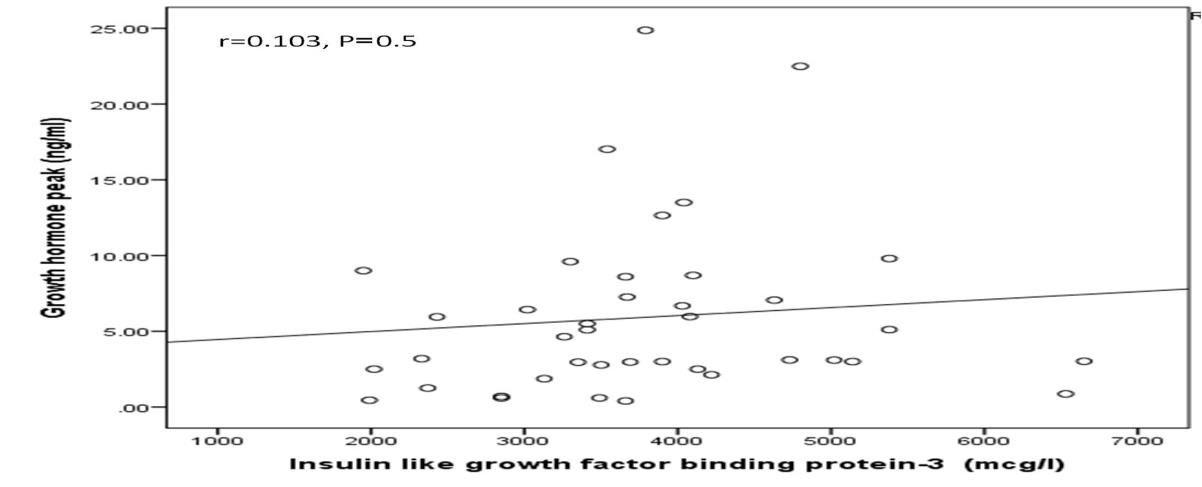
Background and Objective: Growth hormone deficiency (GHD) is one of the most important endocrine and treatable causes of short stature. Reports regarding the sensitivity and specificity of insulin-like growth factor binding protein-3 (IGFBP-3) are not consistent. The aim of our study was to analyze the relevance of IGFBP-3 concentration as a screening test for diagnosis of GHD. Design: We retrospectively studied 40 patients whom were evaluated for short stature at the Endocrinology Department of King Fahad Armed Forces Hospital, Jeddah, Saudi Arabia between January 2015 to December 2018. For IGFBP-3 concentration, laboratory reference ranges were based on age and sex. For all eligible patients, IGFBP-3 concentration was determined and an insulin tolerance test (ITT) was performed. Patients with a peak GH of ≤5.0 ng/ml were considered to be GHD. The cut-off for optimal clinical performance measures was determined from the ROC curve. Sensitivity, specificity, positive and negative predictive values were calculated for IGFBP-3 concentration. Results: Mean age was 14.7 ±1.7 years. There were 83 males (30.9%) and 9 females (99.9%) and mean IGFPB-3 concentration was 3783.3 ±1099.7 mcg/L. Results from the ITT indicated that 21 (52.5%) had GHD. Age was not statistically significant different between GHD (14.7 ±1.9 years) and non-GHD (14.7 ±1.7 years), p=0.9. Moreover, there was non statistical significant more males (53.1%) than females ( 50%) in the GHD patients, P=0.9. In addition, there were not statistically significantly different (p=0.9) between GHD (3752.9 ±1295.9 mcg/L) and non-GHD (3816.8 ±867.0 mcg/L) patients. The mean peak for GH concentration was significantly lower in patients with GHD than without GHD (2.2 ±1.3 ng/ml vs. 9.9 ±5.6 ng/ml, p<0.0001). Peak GH concentration was not significantly positively correlated with IGFBP-3 concentration (r=0.103, P=0.5) (figure 1). The AUC was 43.9%. An IGFBP-3 threshold of <3665 mcg/L was selected to emphasize sensitivity rather than specificity. We tested the diagnostic accuracy of several thresholds. With a threshold of IGFBP-3 in reference to age and sex, sensitivity was 19%, specificity was 89% and the negative predictive value for the diagnosis of GHD was 50%. With a threshold of IGFBP-3 <3665 mcg/L, sensitivity was 57%, specificity was 58% and the negative predictive value for the diagnosis of GHD was 55%. With a threshold of <3075 mcg/L, the sensitivity was 29% and the specificity was 84%. A threshold of <2175 mcg/L, gave a positive predictive value of 67% but a negative predictive value of 49%. 11 of the patients with IGFBP-3 concentration above the threshold of <3665 mcg/L (N=20) were normal and 9 had GH deficiency. These 9 GHD patients had IGFBP-3 concentration that did not differ significantly from those of their GH-sufficient counterparts (4890 ± 1080 vs 4345 ± 609 ng/dl, P=0.2). If IGFBP-3 was used as a screening test (with a concentration threshold <3665 mcg/L) and ITT as a confirmatory test, 00 (50%) out of 40 ITT would not have been performed, leading to the misdiagnosis of 9 GH-deficient adults. Thus, in our study population, such a procedure would misdiagnose 9 (43%) out of 21 GHD patients and yield a sensitivity of 57%. Conclusion: Our study demonstrated the poor negative predictive value of IGFBP-3 concentration for the diagnosis of GHD, making it not possible to minimize the use of the “reference test†method ITT. This observation remains to be validated by population-based studies.
Introduction
Growth is a continuous biologic process subject to genetic, environmental, nutritional and hormonal influences. Altered growth potential may result from disturbance of any of these factors. Short stature (SS), a common problem in child population of developing countries [1, 2]. Common endocrine disorder leading to SS include growth hormone deficiency (GHD) [3]. The prevalence of GHD in children with SS ranges from 2.8% to 69% with the national prevalence of 11% [4, 5, 6, 7, 8, 9].
There are two growth factors; insulin-like growth factor-1 (IGF-1) and IGF-2 and up to six transporter proteins. Though IGF binding protein-1 (IGFBP-1) and IGFBP-3 are the two most studied. IGFBP3 is the most abundant IGFBP in blood and has the highest affinity for IGF1, therefore it accounts for 75–80% of the total carrying capacity. IGF-1 concentration is not recommended to establish the diagnosis of GHD, mainly due to the overlap of IGF-1 concentrations between normal and GH- deficient subjects [10]. If GHD is suspected, IGF-1 and IGFBP-3 levels must be measured and a study of growth hormone (GH) secretion should be carried out. Values of IGF-1 or IGFBP-3 which are more than 2 SD below the normal range suggest a serious disorder of the GH axis, if other causes have been ruled out (malnutrition, liver diseases, hypothyroidism) [11]. Dynamic tests are currently recommended for the diagnosis of GHD: the insulin tolerance test (ITT) is considered as the reference test [12, 13, 14, 15].
Reports regarding the sensitivity and specificity of IGFBP-3 are not consistent [16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27]. In general, however, IGFBP-3 is reported to have good specificity but relatively poor sensitivity for GHD. Another advantage of IGFBP-3 is that they show superior reproducibility in comparison to stimulated GH concentrations [28].
To our knowledge, there have been no nationwide studies using uniform diagnostic criteria. Thus, we tried to improve the simplicity and safety of the diagnosis of GHD. The use of diagnostic strategy IGFBP-3 as the first screening step and the ITT as the second confirmatory step, has not been studied well in a population admitted on routine endocrinological practice for short stature. The aim of our study was to analyze the relevance of optimal cut-points of IGFBP-3 concentration as a screening test for diagnosis of GHD.
Aljabri KS and Bokhari SA. The Relevance of Insulin-Like Growth Factor-Binding Protein-3 Concentrations According to Optimal Cut-Points as a Screening Test for Diagnosis of Growth Hormone Deficiency. J Endocrinol 2019, 3(1): 000136.
Methods
We retrospectively studied 40 patients whom were evaluated for SS at the Endocrinology Department of King Fahad Armed Forces Hospital, Jeddah, Saudi Arabia between January 2015 to December 2018. For IGFBP-3 concentration, laboratory reference ranges were based on age and sex. For all eligible patients, IGFBP-3 concentration were determined and an ITT was performed. The ITT consisted in the IV injection of 0.1 units of insulin/kg body weight. Blood samples were collected 0 (baseline), 30, 60, 90, and 120 min for GH. Blood glucose concentration was also determined to ensure that the patient was hypoglycaemic if blood glucose concentration < 2.2 mmol/l. Patients with a peak GH of ≤5.0 ng/ml were considered to be GHD and patients with a peak GH of ≥5.9 ng/ml were considered not GHD (nGHD). Blood was centrifuged, and serum was frozen with dry ice until analysis by an independent laboratory. Blood glucose was determined using a glucose oxidase method. GH concentration was determined using a radioimmunometric test, with IS 80/505 as international standard. This kit is specific for 20 KD and 22 KD human GH. The detection limit is 0.2 ng/ml. At 1.70 ng/ml, intra and inter assay coefficients of variation are 3.9% and 2.3%, respectively. IGFBP-3 concentration was determined using an immunoradiometric method (Unilabs company, Germany) [29].
Statistical Analysis
Data are presented as means ± standard deviation or numbers (%). Quantitative variables were compared between two groups by using the Student’s test. Differences in categorical variables were analysed using the chi-square test. The relationship between continuous variables was assessed using coefficients of correlation. The ability of IGFBP-3 concentration to discriminate between normal and GH-deficient patients was evaluated by receiver operating characteristic (ROC) curve analysis. The cut-off for optimal clinical performance measures was determined from the ROC curve. Sensitivity, specificity, positive and negative predictive values were calculated for IGFBP-3 concentration. A greater area under the curve (AUC) indicates better predictive capability. An AUC=0.5 indicates that the test performs no better than chance, and an AUC=1.0 indicates perfect discrimination. An ideal test is one that reaches the upper left corner of the graph (100% true positives and no false positives). To determine the optimal IGFBP-3 concentration cutoff points, we computed and searched for the shortest distance between any point on the curve and the top left corner on the y-axis. Distance was estimated at each one-half unit of IGFBP-3 concentration according to the equation: Distance in ROC curve=(9−sensitivity)2+(9−specificity) [30, 31, 32]. Diagnostic performance of IGFBP-3 concentration in predicting GHD was assessed by calculating AUC, sensitivity, specificity, positive and negative predictive values. P value <0.05 indicates significance. The statistical analysis was conducted with SPSS version 23.0 for Windows.
Results
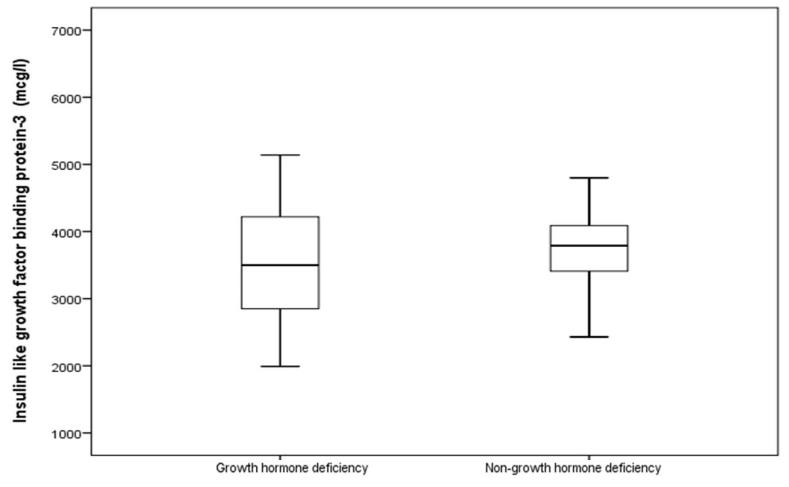
We retrospectively included 40 patients evaluated for SS. Mean age was 14.7 ±1.7 years (Table 1). There were 83 males (30.9%) and 9 females (99.9%) and mean IGFPB-3 concentration was 3783.3 ±1099.7 mcg/L. The observed male to female ratio was 4.2:1. Results from the ITT indicated that 21 (52.5%) had GHD (Table 2). Age was not statistically significant different between GHD (14.7 ±1.9 years) and non-GHD (14.7 ±1.7 years), p=0.9. Moreover, there was non statistical significant more males (53.1%) than females (50%) in the GHD patients, P=0.9. In addition, there were not statistically significantly different (p=0.9) between GHD (3752.9 ±1295.9mcg/L) and non-GHD (3816.8 ±867.0 mcg/L) patients. The mean peak for GH concentration was significantly lower in patients with GHD than without GHD (2.2 ±1.3 ng/ml vs. 9.9 ±5.6 ng/ml, p<0.0001). Peak GH concentration was not significantly positively correlated with IGFBP-3 concentration (r=0.103, P=0.5) (Figure 1). IGFBP-3 concentration according to GH deficiency status are demonstrated in Figure 2.
| Parameters | Total | |||||
|---|---|---|---|---|---|---|
| Numbers | 40 | |||||
| Age (years) | 14.7 ±1.7 | |||||
| Gender | Male | 32 (80) | ||||
| Female | 8 (20) | |||||
| IGFPB-3 (mcg/L) | 3783.3 ±1099.7 |
Table 1: Demographics [mean±standard deviation or number (%)](IGFBP-3, Insulin-like Growth Factor-binding Protein-3).
Aljabri KS and Bokhari SA. The Relevance of Insulin-Like Growth Factor-Binding Protein-3 Concentrations According to Optimal Cut-Points as a Screening Test for Diagnosis of Growth Hormone Deficiency. J Endocrinol 2019, 3(1): 000136.
| Parameters | GHD | nGHD | P value | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Numbers | 21 ( 52.5 ) | 19 ( 47.5 ) | ||||||||||
| Age (years) | 14.7 ±1.9 | 14.7 ±1.7 | 0.9 | |||||||||
| Gender | Male | 17 ( 53.1 ) | 15 ( 46.9 ) | 0.9 | ||||||||
| Female | 4 ( 50.0 ) | 4 ( 50.0 ) | ||||||||||
| IGFPB-3 (mcg/L) | 3752.9 ±1295.9 | 3816.8 ±867.0 | 0.9 | |||||||||
| GH (Peak) (ng/ml) | 2.2 ±1.2 | 10.1 ±5.7 | <0.0001 |
Table 2: Comparison between patients with growth hormone deficiency (GHD) and non- GHD (nGHD) [mean±standard deviation or number
Aljabri KS and Bokhari SA. The Relevance of Insulin-Like Growth Factor-Binding Protein-3 Concentrations According to Optimal Cut-Points as a Screening Test for Diagnosis of Growth Hormone Deficiency. J Endocrinol 2019, 3(1): 000136.
We plotted a ROC curve of IGFBP-3 concentration according to the diagnosis of GHD using ITT (Figure 3). The AUC was 43.9%. An IGFBP-3 threshold of <3665 mcg/L was selected to emphasize sensitivity rather than specificity. We tested the diagnostic accuracy of several thresholds (Table 3). With a threshold of IGFBP-3 in reference to age and sex, sensitivity was 19%, specificity was 89% and the negative predictive value for the diagnosis of GHD was 50%. With a threshold of IGFBP-3 <3665 mcg/L, sensitivity was 57%, specificity was 58% and the negative predictive value for the diagnosis of GHD was 55%. With a threshold of <3075 mcg/L, the sensitivity was 29% and the specificity was 84%. A threshold of <2175 mcg/L, gave a positive predictive value of 67% but a negative predictive value of 49%.
| IGFPB-3 (mcg/L) | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Statistic | |||||||||||||
| Reference to Age and Sex | <3665 | <3075 | <2175 | ||||||||||
| True positives | 4 | 12 | 6 | 2 | |||||||||
| True negatives | 17 | 11 | 16 | 18 | |||||||||
| False positives | 2 | 8 | 3 | 1 | |||||||||
| False negatives | 17 | 9 | 15 | 19 | |||||||||
| Sensitivity | 19 (5 - 42) | 57 (34 - 78) | 29 (11 - 52) | 10 (1 - 30) | |||||||||
| Specificity | 89 (67 - 99) | 58 (34 - 80) | 84 (60 - 97) | 95 (74 - 100) | |||||||||
| Positive Predictive Value | 67 (29 – 91) | 60 (44 – 74) | 67 (37 - 87) | 67 (16 - 95) | |||||||||
| Negative Predictive Value | 50 (44 - 56) | 55 (40 - 70) | 52 (43 - 60) | 49 (44 - 53) | |||||||||
| Accuracy | 53 (36 - 68) | 58 (41 - 73) | 55 (38 - 71) | 50 (34 - 66) |
Table 3: Diagnostic performance of Insulin-like Growth Factor-binding Protein-3 (IGFBP-3).
11 of the patients with IGFBP-3 concentration above the threshold of <3665 mcg/L (N = 20) were normal and 9 had GH deficiency. These 9 GHD patients had IGFBP-3 concentration that did not differ significantly from those of their GH-sufficient counterparts (4890 ± 1080 vs 4345 ± 609 ng/dl, P=0.2). If IGFBP-3 was used as a screening test (with a concentration threshold <3665 mcg/L) and ITT as a confirmatory test, 00 ( 50%) out of 40 ITT would not have been performed, leading to the misdiagnosis of 9 GH-deficient adults. Thus, in our study population, such a procedure would misdiagnose 9 (43%) out of 21 GHD patients and yield a sensitivity of 57%.
Discussion
Growth is an important objective parameter of health of a child. SS although not a disease per se, may be a manifestation of several diseases. The diagnosis of GHD in Aljabri KS and Bokhari SA. The Relevance of Insulin-Like Growth Factor-Binding Protein-3 Concentrations According to Optimal Cut-Points as a Screening Test for Diagnosis of Growth Hormone Deficiency. J Endocrinol 2019, 3(1): 000136.
children with SS is very important because GHD responds better to GH treatment, compared to other causes of short stature [18]. Furthermore, appropriate replacement therapy enables the GHD child before epiphyseal fusion to achieve a normal adult height. In this 3-year retrospective study, we found that IGFBP-3 concentration was not significantly correlated with peak GH concentration during ITT. We confirmed that IGFBP-3 concentration with a threshold below the reference range for age and sex has a poor positive predictive value for the diagnosis of GHD. Moreover, IGFBP-3 concentration with a thresholds <3665 mcg/L, 3075 mcg/L and 2175 mcg/L have poor positive and negative predictive values for the diagnosis of GHD. Thus, the measurement of IGFBP-3 concentration, followed by a confirmatory dynamic test ITT for patients with an IGFBP-3 concentration below the reference range for age and sex or a threshold <3665 mcg/L or lower, proved to be an invalid approach. We also observed a non-statistical significant negative correlation between age and IGFBP-3 concentration (r= -0.161, P=0.3), as seen in many reports [13, 33, 34].
Serum concentration of IGFBP-3 reflects the endogenous GH secretion in healthy children and exhibit little diurnal variation, which makes it potential candidates for screening of GHD [17]. However, both sensitivity and specificity of serum IGFBP-3 concentration varied greatly in previous studies [16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27]. Measurement of IGFBP-3 was confirmed useful in the diagnosis of GHD children later and suggested to be an excellent method to discriminate between GHD children and short-statured children with normal GH level [20]. IGFBP-3 is particularly useful in young children, in whom serum IGF- 1 levels are in the same range in GHD and non-GHD [17]. But it has been disputed by others for the low sensitivity in spite of high specificity [16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 35, 36]. In our study, the sensitivity and specificity of IGFBP-3 concentration <2175 mcg/L are 10 and 95 %, respectively. The diagnostic characteristics are summarized in the ROC curve. The AUC wase determined to assess the discriminating ability. Rosman in our study, AUC was 0.439 (95% CI; 0.256, 0.621), indicating that IGFBP-3 had poor accuracy in GHD diagnosis.
Since GH testing is time-consuming, invasive, costly, and even hazardous, simple methods are necessary to identify those short children in whom GH testing is most appropriate. Our study indicated that IGFBP-3 concentration <2175 mcg/L had high specificity (95%) but low sensitivity (10%). The high specificity but low sensitivity suggested that in deciding whether or not a short child should be subjected to GH testing, the positive result should undergo provocative tests. Although IGFBP- 3 concentration could not replace the provocative tests in the diagnosis of GHD, it could not be concluded from our finding to be used as an auxiliary method and a complementary tool to avoid repeated provocative tests. The clinical relevance of our diagnostic strategy is of critical importance. This approach could not distinguish individuals with GHD from individuals without. This affects therapeutic options, as GHD adults can be treated with recombinant GH, which may improve their height and quality of life. We are concerned by the imperfect diagnostic performance of the threshold IGFBP-3 concentration <3665 mcg/L; it misdiagnosed 9/21 patients, meaning that these 9 patients would have been denied for recombinant GH treatment. Furthermore, these patients could be the least likely to benefit from recombinant human GH treatment as suggested by their normal IGFBP-3 concentration although this is disputed by others [37, 38]. Interestingly, the diagnostic procedure using a very low threshold for IGFBP-3 concentration <2175 mcg/L is not associated with a 100% positive predictive value (67%). With this threshold, 19 out of 21 patients would have been misclassified as GHD in our study population. We believe that our diagnostic procedure (i.e. IGFBP-3 concentration <3665 mcg/L) is safer than that with the low threshold (<2175 mcg/L) because even if some patients would not have access to GH, despite being potential candidates for this treatment, all candidates for GH treatment identified by the cascade test approach had effective GHD. Conversely, with the low threshold procedure, some patients with normal GH function would receive GH therapy, which is not indicated currently.
Some limitations must be acknowledged. This is a single centre study, with a small number of patients. We had to rely on IGFBP-3 concentration and not on IGF-1. IGF-1 has been reported to be of greater diagnostic value by some, but not all authors [17, 39, 40, 41]. Coupled with ITT in a diagnostic strategy such as what is proposed here, this variability will lead to inappropriate GH therapy. It is very important to know exactly the frequency of various causes of SS from a given population in order to differentiate normal variants of growth from individual cases of short stature who need early diagnosis and treatment. Statistics addressing frequencies of various causes of growth failure in Saudi Arabia are not plentiful. This study may help to set an appropriate detection of treatable causes would be helpful in a better long-term prognosis. In conclusion, many reports have already reported that IGFBP-3 concentration is lower in patients with GHD than in the general population, our study Aljabri KS and Bokhari SA. The Relevance of Insulin-Like Growth Factor-Binding Protein-3 Concentrations According to Optimal Cut-Points as a Screening Test for Diagnosis of Growth Hormone Deficiency. J Endocrinol 2019, 3(1): 000136.
demonstrated the poor negative predictive value of IGFBP-3 concentration for the diagnosis of GHD, making it not possible to minimize the use of the “reference test” method ITT. This observation remains to be validated by population-based studies.
Acknowledgement
The author would like to thank all colleagues from the Department of endocrinology for helping in data collection.
Conflict of Interests
The authors declare no conflict of interests.
References
-
Lam WF, Hau WL, Lam TS (2002) Evaluation of referrals for genetic investigation of short stature in Hong Kong. Chin Med J (Engl) 115(4): 607-611.
-
Rogol AD (2007) Causes of short stature. _In:_ Rose BD (Ed.), Up-to date 15.1 [CD Rom]. Waltham MA: up-to- date.
-
Famuyiwa OO (1992) Short stature at the University College Hospital, Ibadan, Nigeria. West Afr J Med 11(1): 62-71.
-
Shu SG, Chen YD, Chi CS (2002) Clinical evaluation of short children referred by school screening: an analysis of 655 children. Acta Paediatrica Taiwanica 43(6): 340-344.
-
Lindsay R, Feldkamp M, Harris D, Robertson J, Rallison M (1994) Utah growth study: growth standards and the prevalence of growth hormone deficiency. J Pediatr 125(1): 29-35.
-
Kaur A, Phadke SR (2012) Analysis of short stature cases referred for genetic evaluation. Indian J Pediatr 79(12): 1597-1600.
-
Zayed AA, Mustafa Ali MK, Al-Ani MA, Momani MS, Yousef AMF (2014) The prevalence of isolated growth hormone deficiency among children of short stature in Jordan and its relationship with consanguinity. Clin Endocrinol (Oxf) 81(6): 876-882.
-
El Mouzan MI, Al Herbish AS, Al Salloum AA, Foster PJ, Al Omer AA et al. (2011) Prevalence of short stature in Saudi children and adolescents. Annals of Saudi Medicine 31(5): 498-501.
-
Mikki N, Abdul-Rahim HF, Faisal Awartani F, Holmboe-Ottesen G (2009) Prevalence and sociodemographic correlates of stunting, underweight, and overweight among Palestinian school adolescents (13–15 years) in two major governorates in the West Bank. BMC Public Health 9: 485.
-
Consensus guidelines for the diagnosis and treatment of adults with growth hormone deficiency: summary statement of the Growth Hormone Research Society Workshop on Adult Growth Hormone Deficiency. J Clin Endocrinol Metab 83(2): 379-381. _11._ _Martinez MJ (2011) Assessment_ and _diagnosis_ of _short_ _stature. Congress_ of the _Association,_ _Spanish_ _of_ _Pediatrics, AEP 2011-60, Valladolid._
-
Hoffman DM, O’Sullivan AJ, Baxter RC, Ho KK (1994) Diagnosis of growth-hormone deficiency in adults. Lancet 343(8905): 1064-1068.
-
Ghigo E, Masel B, Aimaretti G, Leon-Carrion J, Casanueva FF, et al. (2005) Consensus guidelines on screening for hypopituitarism following traumatic brain injury. Brain Inj 19(9): 711–724.
-
Cansanuev FF, Castro AI, Micic D, Kelestimur F, Dieguez C (2009) New guidelines for the diagnosis of growth hormone deficiency in adults. Horm Res 71(Suppl 1): 112-115.
-
Biller BM, Samuels MH, Zagar A, Cook DM, Arafah BM, et al. (2002) Sensitivity and specificity of six tests for the diagnosis of adult GH deficiency. J Clin Endocrinol Metab 87(5): 2067-2079.
-
Galluzzi F, Quaranta MR, Salti R, Saieva C, Nanni L, et al. (2010) Are IGF-I and IGF-BP3 useful for diagnosing growth hormone deficiency in children of short stature? J Pediatr Endocrinol Metab 23(12): 1273- 1279.
-
Juul A, Skakkebaek NE (1997) Prediction of the outcome of growth hormone provocative testing in short children by measurement of serum levels of insulin-like growth factor I and insulin-like growth factor binding protein 3. J Pediatr 130(2): 197-204. Aljabri KS and Bokhari SA. The Relevance of Insulin-Like Growth Factor-Binding Protein-3 Concentrations According to Optimal Cut-Points as a Screening Test for Diagnosis of Growth Hormone Deficiency. J Endocrinol 2019, 3(1): 000136.
-
Haghshenas Z, Sotoudeh K, Karamifar H, Karamizadeh Z, Amirhakimi G (2009) The role of insulin like growth factor (IGF)-1 and IGF-binding protein-3 in diagnosis of growth hormone deficiency in short stature children. Indian J Pediatr 76(7): 699-703.
-
Audi L, Antonia LM, Luisa GM, Hermoso F, Del Valle J, et al. (2001) Low sensitivity of IGF-I, IGFBP-3 and urinary GH in the diagnosis of growth hormone insufficiency in slowly-growing short statured boys. Med Clin 116(1): 6-11.
-
Blum WF, Ranke MB, Kietzmann K, Gauggel E, Zeisel HJ (1990) A specific radioimmunoassay for the growth hormone (GH)-dependent somatomedin- binding protein: its use for diagnosis of GH deficiency. J Clin Endocrinol Metab 70(5): 1292-1298.
-
Boquete HR, Sobrado PG, Fideleff HL, Sequera AM, Giaccio AV, et al. (2003) Evaluation of diagnostic accuracy of insulin-like growth factor (IGF)-I and IGF- binding protein- 3 in growth hormone-deficient children and adults using ROC plot analysis. J Clin Endocrinol Metab 88(10): 4702-4708.
-
Cianfarani S, Liguori A, Boemi S, Maghnie M, Iughetti L, et al. (2005) Inaccuracy of insulin-like growth factor (IGF) binding protein (IGFBP)-3 assessment in the diagnosis of growth hormone (GH) deficiency from childhood to young adulthood: association to low GH dependency of IGF-II and presence of circulating IGFBP-3 18-kilodalton fragment. J Clin Endocrinol Metab 90: 6028-6034.
-
Darendeliler F, Spinu I, Bas F, Bundak R, Isguven P, et al. (2003) Reevaluation of growth hormone deficiency during and after growth hormone (GH) treatment: diagnostic value of GH tests and IGF-I and IGFBP-3 measurements. J Pediatr Endocrinol Metab 17(7): 1007-1012.
-
Jaruratanasirikul S, Leethanaporn K, Sriplung H (2000) The usefulness of serum insulin-like growth factor-1 (IGF-1) and insulin-like growth factor binding protein-3 (IGFBP-3) for evaluation of children with short stature. J Med Assoc Thai 83(6): 619-626.
-
Mitchell H, Dattani M, Nanduri V, Hindmarsh P, Preece M, et al. (1999) Failure of IGF-I and IGFBP-3 to diagnose growth hormone insufficiency. Arch Dis Child 80(5): 443-447.
-
Ranke M, Schweizer R, Elmlinger M,Weber K, Binder G, et al. (2001) Significance of basal IGF-I, IGFBP-3 and IGFBP-2measurements in the diagnostics of short stature in children. Horm Res Paediat 54: 60-68.
-
Rikken B, van Doorn J, Ringeling A, Van den Brande JL, Massa G, Wit JM (1998) Plasma levels of insulin- like growth factor (IGF)-I, IGF-II and IGF-binding protein-3 in the evaluation of childhood growth hormone deficiency. Horm Res Paediatr 50(3): 166- 176.
-
Lee HS, Hwang JS (2011) Influence of body mass index on growth hormone responses to classic provocative tests in children with short stature. Neuroendocrinology 93(4): 259-264.
-
Aneke-Nash CS, Dominguez-Islas C, Bůžková P, Qi Q, Xue X, et al. (2016) Agreement between circulating IGF-I, IGFBP-1 and IGFBP-3 levels measured by current assays versus unavailable assays previously used in epidemiological studies. Growth Horm IGF Res 26: 11-16.
-
Amato G, Carella C, Fazio S, La Montagna G, Cittadini A, et al. (1993) Body composition, bone metabolism, and heart structure and function in growth hormone (GH)-deficient adults before and after GH repla- cement therapy at low doses. J Clin Endocrinol Metab 77(6): 1671-1676.
-
Shan Kuan Z, Zi Mian W, Stanley H, Moonseong H, Faith M, et al. (2002) Waist circumference and obesity-associated risk factors among whites in the third National Health and Nutrition Examination Survey: Clinical action thresholds. Am J Clin Nutr 76(4): 743-749.
-
Weng X, Liu Y, Ma J, Wang W, Yang G, et al. (2006) Use of body mass index to identify obesity-related metabolic disorders in the Chinese population. Eur J Clin Nutr 60(8): 931-937.
-
Shalet SM, Toogood A, Rahim A, Brennan BM (1998) The diagnosis of growth hormone deficiency in children and adults. Endocr Rev 19(2): 203-223.
-
Toogood AA, O’Neill PA, Shalet SM (1996) Beyond the somatopause: growth hormone deficiency in adults over the age of 60 years. J Clin Endocrinol Metab 81(2): 460-465. Aljabri KS and Bokhari SA. The Relevance of Insulin-Like Growth Factor-Binding Protein-3 Concentrations According to Optimal Cut-Points as a Screening Test for Diagnosis of Growth Hormone Deficiency. J Endocrinol 2019, 3(1): 000136.
-
Hasegawa Y, Hasegawa T, Aso T, Kotoh S, Nose O, et al. (1994) Clinical utility of insulin-like growth factor binding protein-3 in the evaluation and treatment of short children with suspected growth hormone deficiency. Eur J Endocrinol 131(1): 27-32.
-
Phillip M, Chalew SA, Kowarski AA, Stene MA (1993) Plasma IGFBP-3 and its relationship with quantitative growth hormone secretion in short children. Clin Endocrinol 39(4): 427-432.
-
Murray RD, Wieringa GE, Lissett CA, Darzy KH, Smethurst LE, et al. (2002) Low-dose GH replacement improves the adverse lipid profile associated with the adult GH deficiency syndrome. Clin Endocrinol (Oxf) 56(4): 525-532.
-
Ahmad AM, Hopkins MT, Thomas J, Ibrahim H, Fraser WD, et al. (2001) Body composition and quality of life in adults with growth hormone deficiency; effects of low-dose growth hormone replacement. Clin Endo- crinol (Oxf) 54(6): 709-717.
-
Cianfarani S, Boemi S, Spagnoli A, Cappa M, Argiro G, et al. (1995) Is IGF binding protein-3 assessment helpful for the diagnosis of GH deficiency? Clin Endocrinol (Oxf) 43(1): 43-47.
-
Granada ML, Murillo J, Lucas A, Salinas I, Llopis MA, et al. (2000) Diagnostic efficiency of serum IGF-I, IGF- binding protein-3 (IGFBP-3), IGF-I/IGFBP-3 molar ratio and urinary GH measurements in the diagno- sis of adult GH deficiency: importance of an appropriate reference popu- lation. Eur J Endocrinol 142(3): 243- 253.
-
Marzullo P, Di Somma C, Pratt KL, Khosravi J, Diamandis A, et al. (2001) Usefulness of different biochemical markers of the insulin-like growth factor (IGF) family in diagnosing growth hormone excess and deficiency in adults. J Clin Endocrinol Metab 86(7): 3001-3008. Aljabri KS and Bokhari SA. The Relevance of Insulin-Like Growth Factor-Binding Protein-3 Concentrations According to Optimal Cut-Points as a Screening Test for Diagnosis of Growth Hormone Deficiency. J Endocrinol 2019, 3(1): 000136.
- Shaping Healthy Futures: Pediatric Endocrine Breakthroughs of 2025
- Precision Medicine in Obesity: Customizing Treatment for 2025
- The Thyroid Revolution: How 2025 is Redefining Hormone Health
- Editorial- Targeting Immunometabolism for Generating Innovative Therapies for Cancer
- Current Knowledge of Chickenpox
- Correlation of Preinjection Values of Gonadotropins and Estradiol Level with Clinical and Radiologic Evidence of Sufficient Pubertal Suppression in Girls with Central Precocious Puberty