Different Tools Used for Treatment of Chronic Hepatitis B
Introduction
The chronic infection hepatitis B is a greater threat to the people from all over the world. This virus is transmitted when any person is exposed to the infected body secretions or blood. The vertical transmission is the transfer of virus from mother to child and horizontal transmission is the transfer of virus from child to another child [1]. When the contaminated blood products are not sterilized than they can also serve the mode of transmission. The intravenous delivery of drugs is also the mode of transmission. The homosexuality is also mode of transmission but heterosexuality also serves as the mode of transmission if a person is sexing with many partners [2, 3, 4]. There are multiple modes of transmission of this disease so its occurrence in different regions of the world is different and it falls in the category of low, medium and high. Before the vaccination the occurrence of HBsAG was from 2% to 20%. The data was collected from different 161 countries that showed greater ration in Africa with 8.83%. It has also been shown that the persons in the age range of 48 to 52 years are more susceptible to this virus [5, 6].
Natural History
The phases of infection of HBV and their history are being studied. If children get infected by HBV than this will be the chronic stage. The different phases of HBV are age dependent. The different phases of HBV are as follows [7]:
- Immunotolerant phase
- Immunoactive phase
- Reactivated phase
These phases also have other names like HBeAG positive, and HBeAG negative.
In case of young adults and children the rate of replication of virus is high while inflammation is low and the concentration of DNA in serum is high. When the rate of multiplication of HBV is very it is indicating the active phase of infection. In some cases, the disease regrets at the rate of 0.5 to 2% in every year [8].
In these patients the activity of virus can be judged due to the presence of HBcAG in the Treatments
The main goal of treatment in every case is to improve the survival of patients and their quality of life. In case of Hepatitis B treatment, the replication of HBV is stopped and the DNA of HBV is targeted to properly cure the disease. When the virus is suppressed than the chances of liver cancer are reduced. There are some treatment strategies which can be followed for the treatment of Hepatitis B and these treatments are as follows [9, 10].
siRNA Therapy
There is another therapy that can be used for the treatment of this disease. This therapy uses a natural mechanism in which the foreign genes or the genes that are no longer required are suppressed. If in the body any viral gene is present its translation is stopped by this process. The greatest problem in this therapy is that there is also effect on the unneeded organs like kidney [11, 12, 13, 14].
This therapy is given through injections as the siRNA gets digested in the gut. If the injections are given intravenous than there are chances of infusion reactions. Now the subcutaneous injections are given that target liver. These injections are used because they have lower side effects and there is no requirement of frequent dosing [15].
The stable siRNA do not activate the immune system of the host and the risk of off targets is also reduced. The genome of HBV is very compact and the siRNA molecules block many genes and the production of many proteins is also blocked. When we block the replication of HBV than the expression of HBeAG and HBsAG is also reduced [16, 17, 18, 19, 20].
The HBV mRNA is inhibited by this technique and the synthesis of its antigens is blocked. This technique is though effective for the treatment of chronic hepatitis B but in the next coming years the draw backs of this technique can be recovered. This technique will be used for clinical purposes in the next coming years [21, 22].
The areas to be covered are improvement of the route of administration, safety profile and the combination of it with the other antiviral drugs. Many small interfering RNAs has been developed and some of them are ALN-HBV, ARC-520 and ARB-1467.
The ARC-520 knockdowns the HBV DNA and the viral drugs. Like the other techniques the mode of this treatment is different as it suppresses the DNA of virus along with its antigens. This one is also effective technique for the treatment of hepatitis B [23, 24].
LNA Technology
An alternative technique to siRNA is LNA technology. This technique is also used to silence genes. The formation of different proteins is blocked by this technique. The advantage of this technique is that the risk of off target is reduced. The toxicity affects the target only. Now a days many treatments are being in use for the treatment of chronic hepatitis B. One of the methods is Taq man DNA technology but this method is old one and new technology is LNA technology. An experiment was performed by using this method in which 40 micro liters of PCR sample was taken and the composition of sample was 2 micro liter DNA sample, 400 micro liter DUTP, 200 nano mole of every primer, 200 micro mole of dGTP, dATP and dCTP, 2U of HotStarTaq DNA polymerase, 75nM of LNA probe, 0.5U uracil DNA glycosylase and 2 micro liter of DNA sample [25]. The amplification of that sample was performed in iCycler iQ5 and the protocol was:
First of all initially activate UDG at the temperature of 37C for the duration of 5 min. In the next step the UDG becomes inactivated. Than the HotStarTaq DNA polymerase becomes activated and the template is denatured at the temperature of 95C for the time period of 3min. Than 40 cycles are performed in two steps in which temperature of 95C is provided for 5sec and 60C is provided for 30 sec.
For every cycle the standard curves were created and the range of these curves was 40-4X107 IU/ml by the 1:10 serial dilutions of PUCm-T-HBV standard and all the samples were run duplicated. Than in order to create standard curves the threshold cycle was used as Y axis and at the x axis there was log of HBV DNA concentration and the examination of potential sample was performed by using Ct values that is corresponding to HBV DNA.
The efficiency of LNA technology is 100% and it was checked by taking 39 cases of known chronic hepatitis B and all of these were shown positive. The LNA technology is the new technology and it is basically the technology that is based on nucleotide chemical modification. This modification is between O2 and C4 and this modification occurs through 2 methyl sugar link.
With this LNA modification the affinity and stability for the DNA molecules has been increased in PCR reactions. The melting temperature of oligonucleotide has been increased by 9.6C. This technology has made it possible to carry out the complicated experiments in a single test tube. These short probes are more sensitive towards single base mismatches. In order to test fetal DNA the LNA probes are more sensitive as compared to conventional DNA. The efficiency of PCR increases while using short probes rather than the large one and hence these probes are more useful in the PCR reactions [26].
In order to detect Salmonella we can also use LNA probes. In case of HBV DNA the detection performance of LNA probes is greater as compared to the common probes. The LNA probes have the detection limits of upto 40IU/ml. There are many more advantages of LNA technology and it is widely used for the treatment of chronic hepatitis B [27].
CRISPR/Cas9
The problem related to other techniques is that they silence the genes during treatment but when the treatment is discontinued than the genes get activated again and again there is the production of proteins. These methods do not eliminate the virus. The solution is that the complete elimination of DNA of the virus.
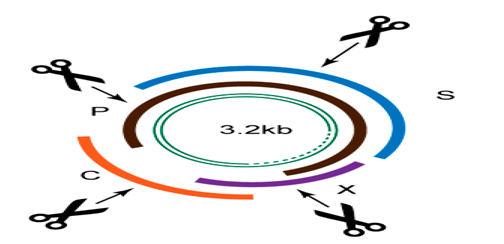
There are different therapies which can be used for the modification of DNA like deacetylase activation and demthylation but the problem in these methods is the risk of off targets. The more beneficial method is the use of CRISPR/ Cas9 which involves the cleavage of DNA. In case of bacteria the CRISPR/Cas9 present in it destroys the genetic material by combining with gRNA. In case of humans their genomes can be edited by the use of CRIPR/Cas9. We can take the example of sickle cell anemia as it is a genetic disorder and it can be cured by using CRISPR/Cas9.
In case of Hepatitis patients this technique reduces the level of DNA and the proteins produced by the host are also reduced. The CRISPR/Cas9 can also be combined with other gene editing tools like siRNA and the DNA is effectively reduced. When we are using this technique we have to follow many challenges and these challenges need to be overcome before we safely apply this to the patients. In this technique there are the chances of off target toxicities. The challenges which we are facing in this technique are overcome than this technique can be applied as the complete treatment of CHB. The chances of reactivation of virus are also reduced in this technique. In this technique the DNA will be completely removed and this can be used as the 100% efficient system. The CRISPER/Cas9 is basically a prokaryotic immune system. This technique is gene editing. In CRISPER many spacer and short regions are present. The type 2 system of CRISPER is widely studied system.
Many of the new spacer regions have been added in the CRISPER as these are more beneficial in case of invading viruses. As the HBV DNA replicates in liver so the CRISPER is than added into the liver. This double stranded DNA of HBV is converted into the single stranded DNA and this one is present on to the surface of liver cells. The complete removal of HBV DNA is very important. The double stranded DNA of HBV is being cut by the CRISPER.
Due to CRISPER the HBV DNA loses its biological activity or even it can be degraded. Its cell content is also reduced. This technique has been checked on the humanized mouse. This CRISPER/Cas9 technique is now used effectively for the treatment of chronic hepatitis B Figure 1 [28].
SBV-specific RNA Targeting Regions
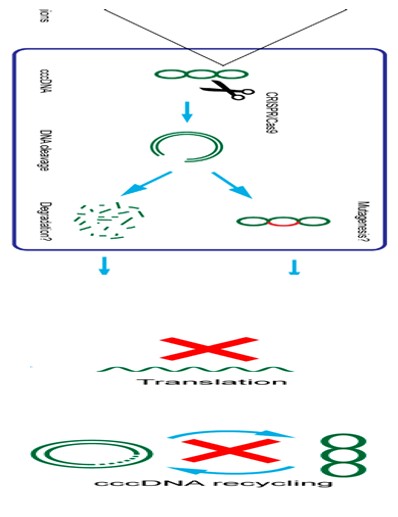
Figure1: Hepatitis B Treating Method of Targeting of Specific ssRNA ToolByCRISPR/Cas9.
Conclusion
Many techniques can be used for the treatment of hepatitis b like siRNA, CRISPER/Cas9 and LNA technology. Each technique has its own benefits and drawbacks. CRISPR/ Cas9 can be the tool that we can use for the treatment of CHB (Chronic Hepatitis B).
References
-
Chan HL, Fung S, Seto WK, Chuang WL, Chen CY, et al. (2016) Tenofoviralafenamide versus tenofovirdisoproxil fumarate for the treatment of HBeAg-positive chronic hepatitis B virus infection: a randomised, double-blind, phase 3, noninferiority trial. Lancet GastroenterolHepatol 1(3): 185-195.
-
Buti M, Gane E, Seto WK, Chan HL, Chuang WL, et al. (2016) Tenofoviralafenamide versus tenofovirdisoproxil fumarate for the treatment of patients with HBeAgnegative chronic hepatitis B virus infection: a randomised, double-blind, phase 3, non-inferiority trial. Lancet GastroenterolHepatol 1(3): 196-206.
-
Arribas JR, Thompson M, Sax PE, Haas B, McDonald C, et al. (2017) Brief Report: Randomized, Double-Blind Comparison of Tenofovir Alafenamide (TAF) vs Tenofovir Disoproxil Fumarate (TDF), Each Coformulated with Elvitegravir, Cobicistat, and Emtricitabine (E/C/F) for Initial HIV-1 Treatment: Week 144 Results. J Acquir Immune DeficSyndr 75(2): 211-218.
-
Raffi F, Orkin C, Clarke A, Slama L, Gallant J, et al. (2017) Brief Report: Long-term (96-week) Efficacy and Safety After Switching from Tenofovir Disoproxil Fumarate (TDF) to Tenofovir Alafenamide (TAF) in HIV-infected, Virologically Suppressed Adults. J Acquir Immune Defic Syndr 75(2): 226-231.
-
Lavanchy D (2004) Hepatitis B virus epidemiology, disease burden, treatment, and current and emerging prevention and control measures. J Viral Hepat 11(2): 97-107.
-
Nelson NP, Easterbrook PJ, McMahon BJ (2016) Epidemiology of Hepatitis B Virus Infection and Impact of Vaccination on Disease. Clin Liver Dis 20(4): 607-628.
-
Weinbaum CM, Williams I, Mast EE, Wang SA, Finelli L, et al. (2008) Recommendations for identification and public health management of persons with chronic hepatitis B virus infection. MMWR Recomm Rep 57(RR- 8): 1-20.
-
Mast EE, Margolis HS, Fiore AE, Brink EW, Goldstein ST, et al. (2005) A comprehensive immunization strategy to eliminate transmission of hepatitis B virus infection in the United States: recommendations of the Advisory Committee on Immunization Practices (ACIP) part 1: immunization of infants, children, and adolescents. MMWR Recomm Rep 54(RR-16): 1-31.
-
Petersen NJ, Barrett DH, Bond WW, Berquist KR, Favero MS, et al. (1976) Hepatitis B surface antigen in saliva, impetiginous lesions, and the environment in two remote Alaskan villages. Appl Environ Microbiol 32(4): 572-574.
-
Ghany MG, Perrillo R, Li R, Belle SH, Janssen HL, et al. (2015) Characteristics of adults in the hepatitis B research network in North America reflect their country of origin and hepatitis B virus genotype. Clin Gastroenterol Hepatol 13(1): 183-192.
-
Schwarz KB, Cloonan YK, Ling SC, Murray KF, Baez NR, et al. (2015) Children with Chronic Hepatitis B in the United States and Canada. J Pediatr 167(6): 1287-1294.
-
Bond WW, Favero MS, Petersen NJ, Gravelle CR, Ebert JW, et al. (1981) Survival of hepatitis B virus after drying and storage for one week. Lancet 1(8219): 550-551.
-
Beasley RP, Huang LY (1983) Postnatal infectivity of hepatitis B surface antigen-carrier mothers. J Infect Dis 147(2): 185-190.
-
Beasley RP, Hwang LY, Lin CC, Leu ML, Stevens CE, et al. (1982) Incidence of hepatitis B virus infections in preschool children in Taiwan. J Infect Dis 146(2): 198- 204.
-
Coursaget P, Yvonnet B, Chotard J, Vincelot P, Sarr M, et al. (1987) Age- and sex-related study of hepatitis B virus chronic carrier state in infants from an endemic area (Senegal). J Med Virol 22(1): 1-5.
-
McMahon BJ, Alward WL, Hall DB, Heyward WL, Bender TR, et al. (1985) Acute hepatitis B virus infection: relation of age to the clinical expression of disease and subsequent development of the carrier state. J Infect Dis 151(4): 599-603.
-
Tassopoulos NC, Papaevangelou GJ, Karayannis AR, Ticehurst JR, Feinstone SM, et al. (1987) Detection of hepatitis B virus DNA in asymptomatic hepatitis B surface antigen carriers: relation to sexual transmission. Am J Epidemiol 126(4): 587-591.
-
Bodsworth N, Cooper D, Donovan B (1991) The influence of human immunodeficiency virus type 1 infection on the development of the hepatitis B virus carrier state. J Infect Dis 163(5): 1138-1140.
-
Centers for Disease Control and Prevention (2011) Use of hepatitis B vaccination for adults with diabetes mellitus: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Morb Mortal Wkly Rep 60(50): 1709-1711.
-
(2016)Division of Viral Hepatitis and National Center for HIV/AIDS Viral Hepatitis STD and TB Prevention. Hepatitis B FAQs for Health Professionals. Atlanta, GA: Centers for Disease Control and Prevention.
-
Raimondo G, Pollicino T, Cacciola I, Squadrito G (2007) Occult hepatitis B virus infection. J Hepatol 46(1): 160- 170.
-
Lok AS, McMahon BJ (2009) Chronic hepatitis B: update 2009. HEPATOLOGY 50(3): 661-662.
-
Gounder PP, Bulkow LR, McMahon BJ (2016) Letter: hepatitis B surface seroclearance does reduce the risk of hepatocellular carcinoma authors’ reply. Aliment Pharmacol Ther 44(6): 650-651.
-
Liu J, Yang HI, Lee MH, Lu SN, Jen CL, et al. (2014) Spontaneous seroclearance of hepatitis B seromarkers and subsequent risk of hepatocellular carcinoma. Gut 63(10): 1648-1657.
-
Nathanson MH, Terrault N (2016) Hepatitis B surface antigen loss: not all that we hoped it would be. Hepatology 64(2): 328-329.
-
Gandhi RT, Wurcel A, McGovern B, Lee H, Shopis J, et al. (2003) Low prevalence of ongoing hepatitis B viremia in HIV-positive individuals with isolated antibody to hepatitis B core antigen. J Acquir Immune DeficSyndr 34(4): 439-441.
-
Terrault NA, Bzowej NH, Chang KM, Hwang JP, Jonas MM, et al. (2016) AASLD guidelines for treatment of chronic hepatitis B. Hepatology 63(1): 261-283.
-
Lok AS, McMahon BJ, Brown RS, Wong JB, Ahmed AT, et al. (2016) Antiviral therapy for chronic hepatitis B viral infection in adults: a systematic review and meta- analysis. Hepatology 63(1): 284-306.
- Shaping Healthy Futures: Pediatric Endocrine Breakthroughs of 2025
- Precision Medicine in Obesity: Customizing Treatment for 2025
- The Thyroid Revolution: How 2025 is Redefining Hormone Health
- Editorial- Targeting Immunometabolism for Generating Innovative Therapies for Cancer
- Current Knowledge of Chickenpox
- Correlation of Preinjection Values of Gonadotropins and Estradiol Level with Clinical and Radiologic Evidence of Sufficient Pubertal Suppression in Girls with Central Precocious Puberty