Management of Indeterminate Thyroid Biopsies, 9-Year Experience in Mexico
Introduction
Thyroid nodules are selected for Fine Needle Aspiration Biopsy (FNAB) based on suspicious ultrasonographic characteristics rather than size alone, as the presence of suspicious ultrasound features is more predictive of malignancy. The American College of Radiology has proposed a system (Thyroid Imaging, Reporting, and Data System [TIRADS]) for selecting nodules for FNAB [1].
When thyroid nodule fine-needle aspiration (FNA) cytologic results show follicular lesion of undetermined significance or atypia of undetermined significance (FLUS/ AUS, Bethesda III) or follicular neoplasm (Bethesda IV), the results are often called indeterminate. The risk of malignancy with these cytological classifications ranges from 10 to 40 percent [2]. Before the introduction of molecular testing, most patients with a cytological result showing FLUS/AUS (confirmed on repeat aspiration) or follicular neoplasm had diagnostic thyroid surgery. However, most patients also had surgery for what was ultimately confirmed to be benign disease [3]. Improvement in the assessment of indeterminate FNAB results with molecular testing allows for better risk stratification and reduces the need for diagnostic thyroid surgery [4].
Material and Methods
We present the results in the follow-up of indeterminate (Bethesda III and IV) cytologies in thyroid nodules, from April 2013 to August 2022, in our research center in the State of Mexico. Patients with a solid thyroid nodule that met FNAB criteria according to the ACR TI-RADS scoring scale (TR3 >2.5 cm, TR4 >1.5 cm and/or TR5 >1cm) were sent to perform ultrasound-guided FNAB, using 25G 1 ½ inch needles, 2 passes per nodule, 1 with aspiration and 1 without aspiration. All the procedures were done by the same team of 2 researchers, one radiologist handling the ultrasound and one endocrinologist doing the biopsies, the ultrasounds were performed with a SonoScape P20 equipment using a 10 Mhertz lineal probe. All the cytology reports were performed by the same cytopathologist.
If the results were Bethesda III or IV, the case was discussed with the patient and the options were given of repeating the FNAB, doing molecular testing, sending to surgery, or doing ultrasonographic follow-up every 6 months.
If the patient chose molecular testing, either and Afirma™ GEC or GSC (depending on the year of the procedure) was performed. If the result came back as “benign” the patient was sent to follow-up, if the result came back as “suspicious for malignancy” the patient was sent to surgery.
Results
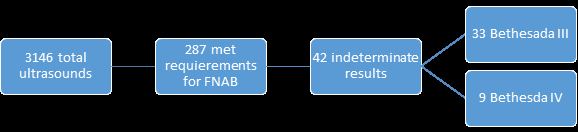
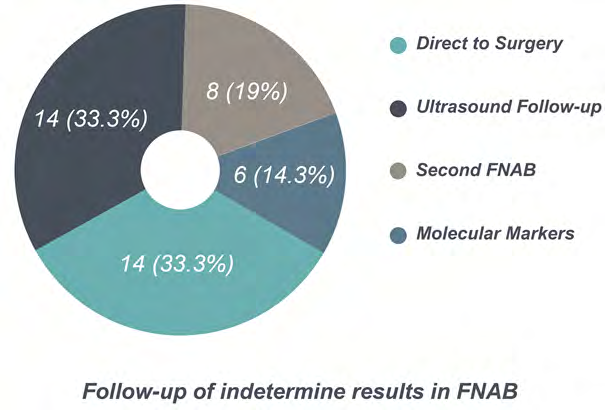
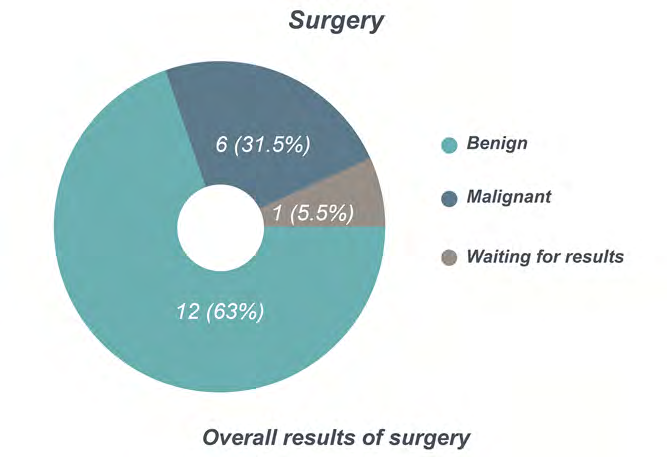
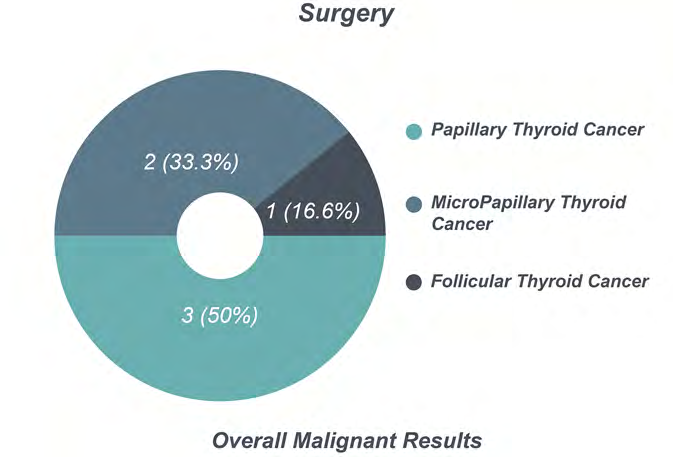
A total of 3146 thyroid ultrasounds and 287 FNAB were performed between January 1st 2013 and August 30th 2022 (Figures 1 and 2). Of these, 42 (14.6%) (Table 1) were classified as either Bethesda III or IV, 14 (33.3%) went directly to surgery, 8 (19%) went for a second FNAB and 6 (15%) underwent molecular marker testing (Figure 3). Overall, a total of 19 patients (45.2%) underwent surgery, 12 had benign results, 6 patients were diagnosed with cancer (1 Follicular, 3 Papillary, 2 micro-Papillary) and 1 result is pending (Figures 4 and 5).
| Patient | Bethesda Score | Sex | Age |
|---|---|---|---|
| 1 | III | M | 40 |
| 2 | III | F | 38 |
| 3 | IV | F | 75 |
| 4 | III | F | 39 |
| 5 | III | F | 24 |
| 6 | III | F | 44 |
| 7 | III | F | 41 |
| 8 | IV | F | 43 |
| 9 | III | M | 56 |
| 10 | IV | M | 60 |
| 11 | IV | F | 49 |
| 12 | III | F | 49 |
| 13 | IV | F | 46 |
| 14 | III | F | 37 |
| 15 | III | F | 38 |
| 16 | III | M | 30 |
| 17 | III | F | 68 |
| 18 | III | F | 41 |
| 19 | III | F | 26 |
| 20 | III | F | 37 |
| 21 | III | F | 49 |
| 22 | III | F | 68 |
| 23 | IV | F | 38 |
| 24 | III | F | 39 |
| 25 | III | F | 32 |
| 26 | III | F | 38 |
| 27 | III | F | 42 |
| 28 | IV | F | 21 |
| 29 | III | F | 41 |
| 30 | III | M | 52 |
| 31 | III | F | 51 |
| 32 | III | F | 61 |
| 33 | IV | F | 53 |
| 34 | III | F | 40 |
| 35 | III | M | 46 |
| 36 | III | F | 77 |
| 37 | III | F | 74 |
| 38 | III | F | 47 |
| 39 | III | F | 37 |
| 40 | III | F | 31 |
| 41 | III | F | 28 |
| 42 | III | M | 75 |
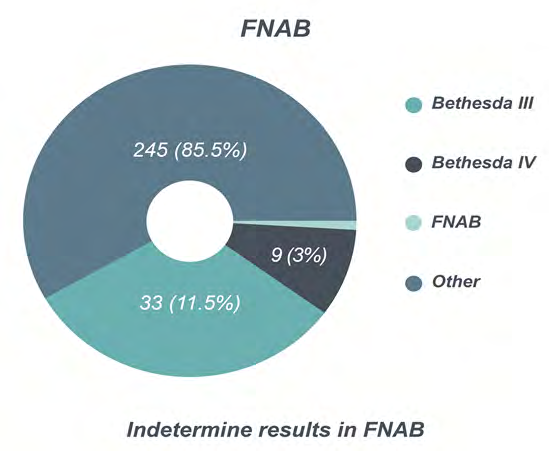
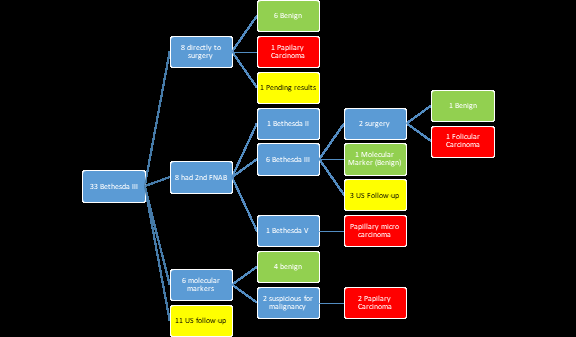
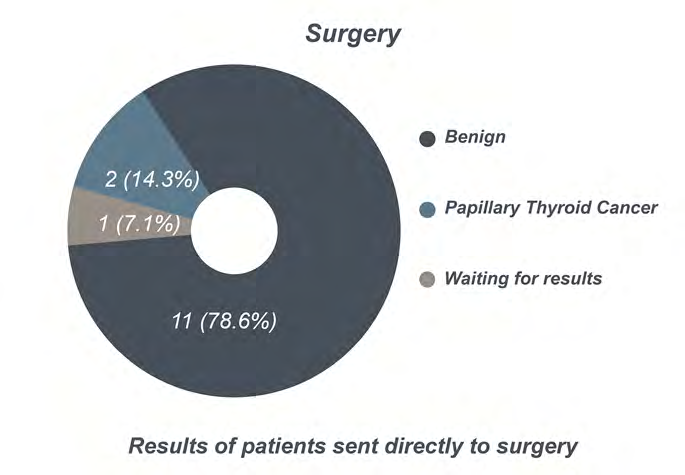
Bethesda III: A total of 33 FNAB were reported as Bethesda III (11.5%). Of these, 8 went directly to surgery (24%), 8 underwent a second FNAB (24%), 6 underwent molecular marker testing (18%) and 11 decided to have their nodules followed by ultrasound every 6 months (34%). Of the patients sent directly to surgery, 6 had a benign report, 1
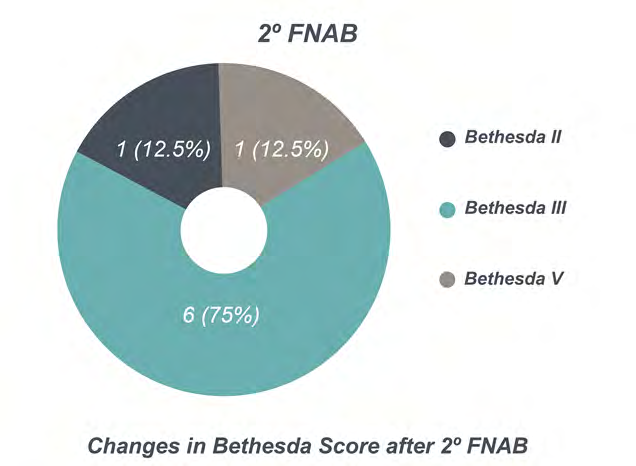
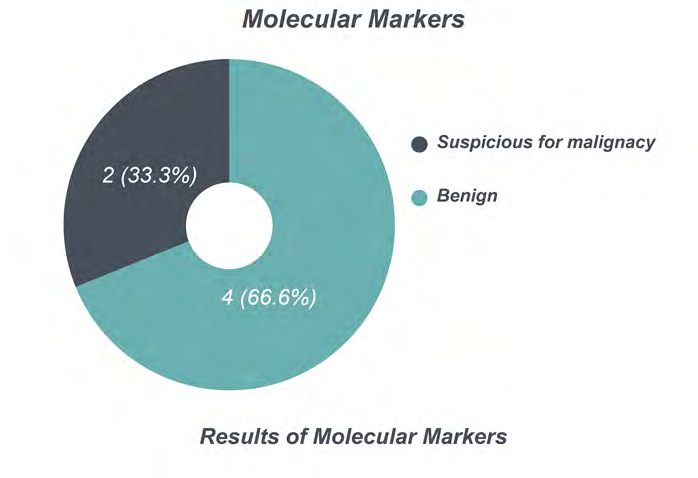
had a Papillary Carcinoma and 1 is pending results. Of the patients who underwent a second FNAB, 1 came back as Bethesda II, 6 as Bethesda III and 1 as Bethesda V (this patient was sent to surgery with a final diagnosis of micro–Papillary Carcinoma). Of the patients that came back as Bethesda III in their 2nd FNAB, 1 underwent molecular markers (with a benign result), 2 were sent to surgery (1 benign result and 1 Follicular Carcinoma) and 3 decided to go to ultrasonographic follow-up. Of the patients who had molecular markers, 4 came back as benign and 2 came back as suspicious for malignancy (these patients were sent to surgery with a final diagnosis of Papillary Carcinoma) (Figure 6).
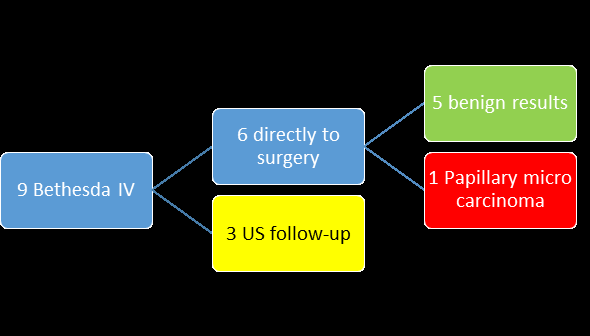
Bethesda IV: A total of 9 FNAB were reported as Bethesda IV (3%). Of these, 6 went directly to surgery (67%), and 3 decided to have their nodules followed by ultrasound every
6 months (33%). The results from surgery were 5 benign tumors and 1 micro–Papillary Carcinoma (Figure 7).
In total, a second FNAB changed the original result in 2 cases (25% of the time) (Figure 8). When the patients went directly to surgery, 14% had a final diagnosis of Cancer (1 Papillary and 1 micro–Papillary Carcinoma) and 79% had benign results (1 result is pending) (Figure 9). Of the 6 patients who underwent molecular marker testing, 4 (67%) had a benign result and 2 (33%) were suspicious for malignancy (Figure 10). Both patients suspected of malignancy underwent surgery and were diagnosed with Papillary Thyroid cancer on both counts (100% PPV).
Discussion
As ultrasonographic equipment becomes a regular standard office practice for many physicians, thyroid nodules are becoming more frequently found on routine examinations, and as ultrasonographic resolution becomes higher, physicians are able to easily biopsy these new found nodules. An increase number of nodule biopsies also implies, just by pure statistics, a greater number of indeterminate (Bethesda III and IV) results.
The most cost-effective follow-up for this patients is essential, in order to avoid as much as possible unnecessary procedures. At the moment, the options for these patients is 1.-Redoe the FNAB, 2.-Doe molecular markers, 3.-Send the patients to surgery, 4.-Follow the patients with periodic (annual or semi-annual ultrasounds).
The aim of our study was to asses, in the context of a developing country with a developing economy, the most cost-effective (even cost-minimizing) protocol to follow-up our indeterminate biopsy patients. We recognize that our study as several limitations: First and foremost, the option of follow-up procedures was determined mainly by the patients’ economic possibilities, as the cost of molecular markers in our country is high (around $3,200 USD) while the average cost of a diagnostic hemi thyroidectomy is much lower than in the United States (around $5,000 USD). Second, the only molecular marker readily available until 2022 was the Afirma™ test, although the ThyroSeq™ test is now also available (at approximately the same cost). Although it is reported that a second FNAB changes the original diagnosis in half the cases, we only found that it did so in 25% of our patients, which renders a second FNAB a poor follow-up choice. Of our patients that went directly to surgery, cancer was detected in 15% of the cases, so that we could argue that 85% of the cases are sent to an “unnecessary” surgery.
Overall, taking into account the patients sent directly to surgery after a first indeterminate result and the patients sent to surgery after a second FNAB also came back as indeterminate, a total of 15 patients underwent surgery with a total of 3 cancers detected (20% of the cases). Of the 6 patients that had molecular markers, 2 were suspicious of malignancy and sent to surgery, resulting in 2 cases of papillary carcinoma, with a positive predictive value of 100%. Finally, of the patients that decided to go to ultrasonographic follow up every 6 months (14 patients, 33% of the whole patient population), more than half were lost-to-follow up after 2 years. These overall results in our population (mixed- race (mestizo) Latino, urban) make us recommend the use of molecular markers as the most cost effective choice in the follow-up of indeterminate thyroid nodules. Finding ways to reduce the cost of commercially available molecular marker testing and coming up with a regional (and race) specific test are high priorities for the adequate treatment of our patients.
Conclusion
The prevalence of Thyroid Nodules meeting the requirements for FNAB in our setting is 1 in every 11 ultrasounds (9%), and our indeterminate biopsy rate is 14.6%. Our malignancy rate is 1 in every 48 nodules (2%). Repeating the FNAB will result in a change in the Bethesda score in 25% of the cases. We found that of the patients that decided not to undergo a second FNAB, molecular markers, or surgery (14 patients), 8 (57%) were lost to follow-up after 2 years. We conclude that taking molecular markers is the most cost-effective option after a first result of an indeterminate thyroid FNAB.
References
-
Tessler FN, Middleton WD, Grant EG, Hoang JK, Berland LL, et al. (2017) ACR Thyroid Imaging, Reporting and Data System (TI-RADS): White Paper of the ACR TI-RADS Committee. J Am Coll Radiol 14(5): 587-595.
-
Cibas ES, Ali SZ (2017) Bethesda System for Reporting Thyroid Cytopathology. 27(11): 1341-1346.
-
Alexander EK, Kennedy GC, Baloch ZW, Cibas ES, Chudova D, et al. (2012) Preoperative diagnosis of benign thyroid nodules with indeterminate cytology. N Engl J Med 367(8): 705-715.
-
Yip L (2014) Use of Molecular Markers for Cytologically Indeterminate Thyroid Nodules to Optimize Surgical Management. Curr Surg Rep.
- Shaping Healthy Futures: Pediatric Endocrine Breakthroughs of 2025
- Precision Medicine in Obesity: Customizing Treatment for 2025
- The Thyroid Revolution: How 2025 is Redefining Hormone Health
- Editorial- Targeting Immunometabolism for Generating Innovative Therapies for Cancer
- Current Knowledge of Chickenpox
- Correlation of Preinjection Values of Gonadotropins and Estradiol Level with Clinical and Radiologic Evidence of Sufficient Pubertal Suppression in Girls with Central Precocious Puberty