Antibiotic Resistance: The Threat of Public Health
The discovery of antibiotics is one of the most significant medical achievements of modern medicine as these agents have become a vital component of clinical practice. Overuse and misuse of these medications lead to the emergence of antibiotic resistance, becoming less effective and has led to the emergence of "superbugs". As superbugs become increasingly common, superbug caused infections are very difficult and sometimes impossible to treat. Patients with and multidrug-resistant organisms infection have an increased risk of death compared to patients with infection due to susceptible strain. The financial risks associated with specific multidrug-resistant organisms are also varying greatly. The current review's main objective is to summarise recent research on the mechanism of antibiotic resistance, therapeutic approaches, and potential new antibiotics being developed to combat superbugs.
Introduction
According to world health organization (WHO) the infectious diseases is the most common cause of deaths accounting more than 25% of total deaths [1]. Both prokaryotes and eukaryotes cause infections. Infection is a process in which bacteria, viruses, fungi or other organisms enter the body, attach to cells, and multiply [2]. To do this, they must overcome the body’s natural defenses at each step. The symptoms vary greatly depending on the part of the body and type of organism involved. The first sign of bacterial infection is often inflammation: fever, pain, swelling, redness, and pus. By contrast, viral infections less commonly cause inflammation but may cause a variety of other symptoms, from a runny nose or sore throat to a rash or swollen lymph nodes [3]. The main treatment is usually medication: antibiotics for bacterial infections; antiviral drugs for some viruses, antifungal medications for fungus infections; and antihelmintic drugs for worms [4]. The current review’s main objective is to summarise recent research on the mechanism of antibiotic resistance, therapeutic approaches, and potential new antibiotics being developed to combat superbugs.
Antibiotic Action
An antibiotic is a selective poison and have been used by the fungi to kill bacteria for many million years. Antibiotic
was first discovered by A. Fleming in 1929. They were brought in to widespread use in 1940’s. Their introduction was the biggest medical breakthrough since sanitation. During 1940’s and 1950’s they were extremely effective. They are widely prescribed often for the medical condition that did not require them. Antibiotics have been used in agriculture, dosing cattle with antibiotics increased yield. By 1970’s the world is flooded with full of antibiotics [5]. Each different type of antibiotic affects different bacteria in different ways to kill them. For example, an antibiotic might inhibit 1) cell wall synthesis (Pencillins and cephalosporins), 2) inhibition of protein synthesis by preventing the translation of mRNA into protein (Chlorophenecol and Erythromycin), 3) inhibition of nucleic acid synthesis by preventing the replication and transcription (Quinolones and Rifampine), 4) by damaging plasma membrane (Polymixin B) and 5) inhibition of synthesis of essential metabolites that required for the survival of bacteria (Sulfanilamide and Trimethoprim). When any of these happens, the bacterium dies instead of reproducing [6]. But, several mechanisms have evolved in bacteria which confer them with antibiotic resistance [7].
Mechanism of Antibiotic Resistance
If a bacterium become resistant to most of the antibiotic drugs and carries several resistance genes, it is called as multidrug resistant (MDR) or, informally, a superbug or super bacterium [8]. A tiny change in one gene or a mutation can turn a bacterial cell into a superbug. One single superbug on its own will not cause much damage but if it reproduces rapidly then it could produce a large population of bacteria which are all resistant to antibiotics [9]. The mechanism of antibiotic resistance can occur by blocking entry of the antibiotic or by inactivating the antibiotic after entering into cell or by altering the target molecule by changing its shape and sometimes efflux of antibiotic before it acts on the bacterial cell is also possible [10].
If bacteria carrying antibiotic resistance genes were ever to cause infection, it would be very difficult for doctors to treat. This antibiotic resistance in bacteria may be an inherent trait of the organism that renders it naturally resistant by lacking a transport system for an antibiotic or the target of the antibiotic molecule, in Gram-negative bacteria, the cell wall is covered with an outer membrane that establishes a permeability barrier against the antibiotic [11]. Bacteria also acquire resistance to antibiotics by means of mutation in its own DNA or by the acquisition of new genetic material from another source [10]. The spontaneous mutation is a very rare event only one bacterium will develop antibiotic resistance in about 10-8 to 10-9 at each infection. The very fast growth rate of bacteria and the absolute number of cells attained means that it doesn’t take long before resistance is developed in a population [12]. Once the resistance genes have developed, they are transferred directly to all the bacteria’s progeny during DNA replication. In the selective environment of the antibiotic, the wild types are killed and the resistant mutant is allowed to grow and flourish [13]. Horizontal gene transfer is another process whereby genetic material contained in small packets of DNA can be transferred between individual bacteria of the same species or even between different species through the conjugation, transformation and transduction processes. Multiple lines of evidence suggested that horizontal gene transfer in the large intestine was the cause of the emergence of resistant infections, and the persistence of antibiotic resistance genes in populations [14].
Superbugs
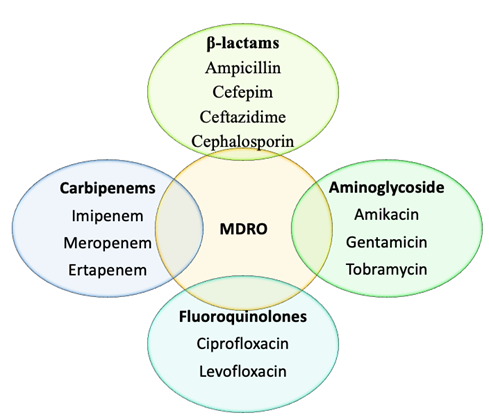
The main cause for the antibiotic resistance is misuse of antibiotics. Misuse includes using outdated or weakened antibiotics, using antibiotics for the common cold and other inappropriate conditions, using antibiotics in animal feed, failing complete the prescribed regimen and using someone else’s leftover prescription [15]. Antibiotic resistance is a serious global public health concern. The first antibiotic- resistant strains of bacteria were identified more than 75 years ago [16]. Multi drug resistant organisms (MDRO) are bacteria that are resistant to several antibiotics. Gram negative MDRO’s (Acintobactor, Pseudomonos and Klebsella) were first identified in 1963 [17]. Later a series of superbugs were reported ex. Methicillin resistant S. aureus (MRSA) (1968), Clostridium difficile (1979) and Vancomycin resistant enterococci (VRE) (1993) [18]. The MDRO gram negative rods are resistant to at least 3 antimicrobial classes shown in Figure 1.
Extended spectrum β-lactamases (ESBL) were identified in 1978. These strains are resistant to all penicillins, cephalosporins, and aztreonam. Many ESBL are also commonly resistant to quinolones, aminoglycosides and trimethoprim [19]. Antibiotic resistance genes in all most all ESBLs are (CTX-M, TEM, SHV) plasmid encoded.ESBL producing organisms include Klebsiella, E coli, Salmonella, Proteus, Pseudomonas. AmpC β-_Lactamases are also similar to the ESBLs and are identified in 1981 [20]. AmpC β-lactamases are cephalosporinases that confer resistance to several β-lactam drugs, β-lactam-β-lactamase inhibitor combinations, and aztreonam. Phenotypically AmpC beta-lactamases producers include several members of the _Enterobacteriaceae [21]. Klebsiella pneumoniae carbapenemase (KPC) was identified in 2001. β-lactamase occurs in Enterobacteriaceae (plasmid encoded) and can confer resistance to all β-lactam agents including carbapenems_. The Modified Hodge Test is a phenotypic confirmatory test for “carbapenemase” activity (VIM, IMP, KPC) and is indicated when there is a positive screening test and resistance to one or more agents in cephalosporin subclass III (i.e., cefotaxime, ceftazidime, and ceftriaxone) [22]. KPC producing organisms are _K pneumoniae, S marcescens, E coli, Enterobacter.
Implications of Superbugs
New Delhi metallo-beta-lactamase (NDM-1) was identified in August 2008. NDM-1 is found in Enterobacteriaceae isolates (plasmid encoded) [23]. Most isolates demonstrate resistance to all antibiotics except tigecycline and colistin. It has showed wider international spread and became endemic to many regions, most isolates worldwide associated with travel to India or Pakistan. Phenotypic screening is molecular confirmation with the presence of 180 kb transmissible genetic element. The clinical consequences of MDROs are mainly, patients with MDRO infection will have limited treatment options compared to those with a more antibiotic-susceptible infection [24]. For some MDRO’s, only 1 or 2 antibiotics are left for treatment, and these often have toxic side effects. The morbidity associated with MDROs is different for several different types of MDROs have shown that MDRO-infected patients also have increased length of hospitalization, increased risk of ICU admission, increased length of ICU stay and increased hospital costs [25]. Patients with and MDRO infection have an increased risk of death compared to patients with infection due to susceptible strain. The financial risks associated with specific MDROs are also varying greatly. Mean cost of care for patients with Methicillin resistant S. aureus surgical site infection is three times higher than for uninfected patients [26]. After controlling for other factors, the total hospital costs for caring for a patient with Vancomycin resistant enterococci infection was 1.4 fold greater than for uninfected patients. Expenses associated with highly resistant gram- negative bacteria infections were 1.5 to 2 times greater than other infections. Studies have demonstrated that the median institutional cost of hospital–acquired infections was 4.6 times greater than the amount budgeted for infection prevention activities [27].
The MDROs has been identified in globally-prevalent infections such as tuberculosis and S. aureus. Emerging antibiotic resistance is now being seen in Gram-negative pathogens including P. aeruginosa [28]. In addition, drug- resistant pathogens that were previously only seen in hospital settings, such as multidrug-resistant Staphylococcus aureus (MRSA), are becoming more common in the community at large [29]. Less than a hundred years ago, our immune system couldn’t handle infections. Later the ‘wonder’ drugs, antibiotics capable of fighting the infections for us. The antibiotic use and misuse led the rise of the ‘Superbugs’ and changed the scenario back to the pre-antibiotic era, threatening our once potent arsenal of antibiotics, rendering them useless and impotent against a variety of re-emerging microbes [30].
Development of New Antibiotics
From 1968 to 200 there are no new classes of antibiotics identified. Since 2000 only four classes were approved by the Food and drug administration (FDA), these are all effective against MRSA and VREs [31]. Apart from Tigecycline no new classes of antibiotics that work against gram negative bacteria were approved. Now there is a pressure to develop newer agents. There is a steady decline in the approval of new antibacterial agents and also a small pipeline for the investigation of antibacterial agents through clinical development, limiting the availability of new agents to treat emerging MDR bacterial strains [32]. High cost involved in antibiotic development and the difficulty of conducting clinical trials to determine the efficacy and safety of investigational antibacterial compounds is limiting the development of antibacterial [33]. Furthermore, the short treatment length with antibiotics compared to medicines used to treat chronic conditions, which reduces the return on investment for developers also contributing to the delay in development of antibacterials [34]. In an effort to remedy these and other concerns, the FDA, the centers for disease control (CDC), and the national institute of health (NIH) released a draft “public health action plan to combat antimicrobial resistance” in March 2011 that includes recommendations and roles for the government agencies in surveillance, prevention and control, research, and product development. It is essential for resources to be invested by all parties, including academic researchers, governmental agencies, policy makers, and pharmaceutical companies, to develop novel, safe and effective treatments for the life- threatening diseases caused by MDR bacteria.
Future Directions
Now faced with the danger of returning to the pre- antibiotic era and shortened life spans, the discovery of new drugs to fight these diseases is gaining ground slowly. Molecular and structural biologists are trying to understand the mechanisms by which microbes can degrade antibiotics. Medicinal chemists are trying to design more potent antibiotics. The National Center for Biotechnology Information (NCBI) has developed a database for the antibiotic resistant genes. Genomic techniques identified 96 genes essential for survival and growth of Staphylococcus aureus. The list of genes presents proteins of all the major metabolic and architectural pathways operative in bacteria. One essential gene described is gcaD, responsible for producing a protein crucial in cell wall synthesis and now a choice candidate for its drug discovery efforts. Now, more than ever, we need to think ‘out of the box’ in order to win the attack against Superbugs. It is truly a grand battle of science, technology and survival, both for bacteria and for mankind.
References
-
Gulati BK, Sharma S, Rao MVV (2021) Analyzing the Changes in Certain Infectious and Parasitic Diseases in Urban Population of India By Using Medical Certification of Cause of Death Data. Indian J Community Med 46(1): 20-23.
-
Cole LA, Kramer PR (2015) Bacteria, Virus, Fungi, and Infectious Diseases. 1st(Edn.), Human Physiology, Biochemistry and Basic Medicine, pp: 193-196.
-
Stevens DL, Bisno AL, Chambers HF, Everett ED, Dellinger P, et al. (2005) Practice Guidelines for the Diagnosis and Management of Skin and Soft-Tissue Infections. Clinical Infectious Diseases 41(10): 1373-1406.
-
Dalhoff A (2015) Antiviral, antifungal, and antiparasitic activities of fluoroquinolones optimized for treatment of bacterial infections: a puzzling paradox or a logical consequence of their mode of action? Eur J Clin Microbiol Infect Dis 34(4): 661-668.
-
Manyi-Loh C, Mamphweli S, Meyer E, Okoh A (2018) Antibiotic Use in Agriculture and Its Consequential Resistance in Environmental Sources: Potential Public Health Implications. Molecules 23(4): 795.
-
Kohanski MA, Dwyer DJ, Collins JJ (2010) How antibiotics kill bacteria: from targets to networks. Nat Rev Microbiol 8(6): 423-435.
-
Munita JM, Arias CA (2016) Mechanisms of Antibiotic Resistance. Microbiol Spectr 4(2): 10.
-
Exner M, Bhattacharya S, Christiansen B, Gebel J, Goroncy-Bermes P, et al. (2017) Antibiotic resistance: What is so special about multidrug-resistant Gram- negative bacteria? GMS Hyg Infect Control 12: Doc 05.
-
Uddin TM, Chakraborty AJ, Khusro A, Zidan BRM, Mitra S, et al. (2021) Antibiotic resistance in microbes: History, mechanisms, therapeutic strategies and future prospects. J Infect Public Health 14(12): 1750-1766.
-
Reygaert WC (2018) An overview of the antimicrobial resistance mechanisms of bacteria. AIMS Microbiol 4(3): 482-501.
-
Wang G, Wilson TJ, Jiang Q, Taylor DE (2001) Spontaneous mutations that confer antibiotic resistance in Helicobacter pylori. Antimicrob Agents Chemother 45(3): 727-733.
-
Peterson E, Kaur P (2018) Antibiotic Resistance Mechanisms in Bacteria: Relationships between Resistance Determinants of Antibiotic Producers, Environmental Bacteria, and Clinical Pathogens. Front Microbiol 9: 2928.
-
Huddleston JR (2014) Horizontal gene transfer in the human gastrointestinal tract: potential spread of antibiotic resistance genes. Infect Drug Resist 7: 167- 176.
-
Ventola CL (2015) The antibiotic resistance crisis: part 1: causes and threats. P T 40(4): 277-283.
-
Davies J, Davies D (2010) Origins and evolution of antibiotic resistance. Microbiol Mol Biol Rev 74(3): 417- 433.
-
Marchaim D, Katz DE, Munoz-Price LS (2013) Emergence and Control of Antibiotic-resistant Gram-negative Bacilli in Older Adults. Current Translational Geriatrics and Experimental Gerontology Reports 2(3): 113-124.
-
Loomba PS, Taneja J, Mishra B (2010) Methicillin and Vancomycin Resistant S. aureus in Hospitalized Patients. J Glob Infect Dis 2(3): 275-283.
-
Paterson DL, Bonomo RA (2005) Extended-spectrum beta-lactamases: a clinical update. Clin Microbiol Rev 18(4): 657-686.
-
Tekele SG, Teklu DS, Tullu KD, Birru SK, Legese MH (2020) Extended-spectrum Beta-lactamase and AmpC beta-lactamases producing gram negative bacilli isolated from clinical specimens at International Clinical Laboratories, Addis Ababa, Ethiopia. PLoS One 15(11): e0241984.
-
Jacoby GA (2009) AmpC beta-lactamases. Clin Microbiol Rev 22(1): 161-182.
-
Tzouvelekis LS, Markogiannakis A, Psichogiou M, Tassios PT, Daikos GL (2012) Carbapenemases in Klebsiella pneumoniae and other Enterobacteriaceae: an evolving crisis of global dimensions. Clin Microbiol Rev 25(4): 682-707.
-
Fazeli H, Norouzi-Barough M, Ahadi AM, Shokri D, Solgi H (2015) Detection of New Delhi Metallo-Beta- Lactamase-1 (NDM-1) in carbapenem- resistant Klebsiella pneumoniae isolated from a university hospital in Iran. Hippokratia 19(3): 205-209.
-
Barrasa-Villar JI, Aibar-Remón C, Prieto-Andrés P, Mareca-Doñate R, Moliner-Lahoz J (2017) Impact on Morbidity, Mortality, and Length of Stay of Hospital- Acquired Infections by Resistant Microorganisms. Clin Infect Dis 65(4): 644-652.
-
Chen YP, Tasi XW, Chang K, Cao XD, Chen JR, et al. (2021) Multi-Drug Resistant Organisms Infection Impact on Patients Length of Stay in Respiratory Care Ward. Antibiotics (Basel) 10(5): 608.
-
Anderson DJ, Kaye KS, Chen LF, Schmader KE, Choi Y, et al. (2009) Clinical and financial outcomes due to methicillin resistant Staphylococcus aureus surgical site infection: a multi-center matched outcomes study. PLoS One 4(12): e8305.
-
Curtis LT (2008) Prevention of hospital-acquired infections: review of non-pharmacological interventions. J Hosp Infect 69(3): 204-219.
-
Cassone M, Mody L (2015) Colonization with Multi- Drug Resistant Organisms in Nursing Homes: Scope, Importance, and Management. Curr Geriatr Rep 4(1): 87-95.
-
Duin DV, Paterson DL (2016) Multidrug-Resistant Bacteria in the Community: Trends and Lessons Learned. Infect Dis Clin North Am 30(2): 377-390.
-
Butt MH, Saleem A, Javed SO, Ullah I, Rehman MU, et al. (2022) Rising XDR-Typhoid Fever Cases in Pakistan: Are We Heading Back to the Pre-antibiotic Era? Front Public Health 9: 794868.
-
Rai J, Randhawa GK, Kaur M (2013) Recent advances in antibacterial drugs. Int J Appl Basic Med Res 3(1): 3-10.
-
Terreni M, Taccani M, Pregnolato M (2021) New Antibiotics for Multidrug-Resistant Bacterial Strains: Latest Research Developments and Future Perspectives. Molecules 26(9): 2671.
-
Silver LL (2011) Challenges of antibacterial discovery. Clin Microbiol Rev 24(1): 71-109.
-
Dutescu IA, Hillier SA (2021) Encouraging the Development of New Antibiotics: Are Financial Incentives the Right Way Forward? A Systematic Review and Case Study. Infect Drug Resist 14: 415-434.
-
Infectious Diseases Society of America (IDSA): Spellberg B, Blaser M, Guidos RJ, Boucher HW, Bradley JS, et al. (2011) Combating antimicrobial resistance: policy recommendations to save lives. Clin Infect Dis 52(Suppl 5): S397-S428.
- Antifungal Activity of New Acetophenone Derivatives
- Interconnected Microbiomes Human Health Within an Environmental Framework
- Silkworm-Based Vaccine Production for H5N1: A One Health Approach to Pandemic Preparedness
- Microbial Diversity and Lipolytic Activity of Bacteria and Fungi from Oil-Contaminated Sites in Makurdi Metroplois
- Antibiotic Resistance Profile of Bacteria Isolated at the Central Laboratory of the National Hospital Center of Nouakchott
- Epidemiology and Sensitivity to Antibiotics of Germs Isolated from Blood Cultures in the Laboratory of the National Hospital Center of Nouakchott-Mauritania