Epidemiology and Sensitivity to Antibiotics of Germs Isolated from Blood Cultures in the Laboratory of the National Hospital Center of Nouakchott-Mauritania
This study aims to examine the results of blood cultures carried out at the National Hospital Center (CHN) of Nouakchott over a 26-month period (2021-2023). The primary objective was to determine the positivity rate and distribution of bacterial isolates. Additionally, this retrospective analysis aimed to evaluate antibiotic resistance patterns among the identified microorganisms to guide clinical decision-making and improve therapeutic strategies. A total of 212 blood cultures were analyzed, of which 45 (21.22%) were positive. Among these, 71.12% were Gram-positive bacteria, while 26.67% were Gramnegative. The majority of affected patients were male (57%), with a sex ratio of 1.3, and pediatric cases were significantly represented. Automated blood culture systems (BACT/ALERT®) and identification by VITEK-2 facilitated pathogen detection. Antibiotic resistance was a major concern, with 44.44% of Staphylococcus aureus strains resistant to penicillin M, while Klebsiella pneumoniae exhibited multidrug resistance, including extended-spectrum beta-lactamase (ESBL) production. A notable case of candidemia was observed in a premature neonate, who presented persistent fever and sepsis unresponsive to antibiotics. Early identification of Candida spp. led to antifungal therapy with fluconazole, resulting in clinical improvement. This highlights the importance of considering fungal infections in high-risk patients. These findings emphasize the critical role of continuous surveillance of bacterial resistance patterns in optimizing empirical antibiotic therapy and infection control strategies. Strengthening antimicrobial stewardship programs and laboratory diagnostic capabilities is essential to improving patient outcomes and limiting the spread of multidrug-resistant organisms.
Abbreviations
CHN: National Hospital Center; ESBL: Extended-spectrum beta-lactamase; CA-SFM: Committee of the French Society of Microbiology; SFP: Sensitive at High Dosage; BLA:
Beta-lactams; LLP: Low-level penicillins; HLP: High-level Penicillins: LLC: Low-level Cephalosporinase; HLC: High- level Cephalosporinase; PM: Penicillin M; FA: Fusidic Acid; PG: Penicillin G; SSUHC: Souro Sanou University Hospital Center; CoNS: Coagulase-Negative Staphylococci; MRSA:
Methicillin-resistant Staphylococcus Aureus; HPC: Hyper- produced Cephalosporinase; CRE: Carbapenem Resistant; PICU: Pediatric Intensive Care Unit.
Introduction
Blood culture is an essential test in medical bacteriology, making it possible to demonstrate the passage of microorganisms in the blood, to identify them and to determine their sensitivity to anti-infectives. It is one of the most frequently performed microbiological tests in hospitals worldwide and remains the gold standard for the detection of bacteraemia [1]. The clinical and epidemiological situations are very varied, but they all have one thing in common: the bacteriological examination for which the relationship between the doctor and the biologist has the most impact in terms of diagnostic strategy and prognosis of the disease. infection [2]. A large number of pathogens can be isolated from blood cultures. They are either of community origin or acquired in hospital, where bacteraemia represents 8 to 10% of nosocomial infections [3]. Infectious diseases actually play a major role in the pathology of tropical areas, with particularly serious consequences in Africa, especially among children [4]. The ability of microorganisms to circulate in the blood and cause bacteraemia and septicaemia is a major concern. Indeed, even in the case of severe septicaemia, these pathogens are often present in quantities too small to be detected directly under a microscope [5].
The introduction of blood culture as a diagnostic technique plays a crucial role in this fight. This method involves culturing a blood sample in an environment conducive to the growth of bacteria or fungi [5]. The major advantage of blood culture lies in its ability to confirm the existence of pathogens in the blood, thus facilitating the prescription of targeted treatment, whether antibiotic or antifungal, against the specific infectious agent identified. This precise diagnostic tool is vital to improve the chances of survival and reduce the morbidity linked to these severe infections [6]. Germs found in blood cultures can vary depending on many factors, such as geographic region, hospital environment, population studied and antibiotic prescribing practices. The most commonly identified germs in blood cultures are Staphylococcus aureus, representing 20-30% of blood infections. Escherichia coli approximately 10-15%. Streptococcus pneumoniae, Klebsiella pneumoniae and Enterococcus spp approximately 5-10% [7].
Currently, sepsis/septic shock and associated bloodstream infections are among the most common causes of morbidity and mortality in both rich and low-income countries, but the causative organisms and risk factors differ; These are diagnostic and therapeutic emergencies where any delay in starting antibiotic therapy or any inappropriate antibiotic therapy puts the vital prognosis at risk [8]. Blood culture is an essential laboratory test for diagnosing bloodstream infections, but false-positive blood culture results caused by inadequate blood culture technique can lead to patient morbidity, unnecessary antibiotic treatment, and additional medical costs. However, the result of this examination requires, depending on the case, from 24 hours to several days [1].
The objective of our work was to study the bacterial epidemiology and the sensitivity to antibiotics of germs isolated from blood cultures in the laboratory of the National Hospital Center (CHN) of Nouakchott, to retrospectively report the data collected at the Bacteriology laboratory of the CHN, to discuss the patients concerned (according to sex, age and hospital department) and analyze the microbiological data (microorganisms isolated and their antibiotic resistance profiles).
Material and Methods
Study Framework
Our study was carried out in the bacteriology laboratory department of the National Hospital Center of Nouakchott.
Type of Study
This is a retrospective descriptive study.
Study Period
Our study took place from October 1, 2021 to November 30, 2023.
Inclusion Criteria
As part of this study, all positive blood cultures were considered, regardless of the requesting department, including both sexes and all age groups.
Non-inclusion Criteria
- Blood cultures outside the study period.
- Unusable data: such as missing or unreadable data.
Microbiological Analysis
Blood cultures are carried out using the vacuum blood collection system allowing 8 to 10 millilitres of venous blood to be injected into aerobic and anaerobic vials of the BACT/ ALERT® system (BioMérieux, France). These vials, enriched with nutrients and growth factors, also contain resins which neutralize antibiotics possibly present in the blood. The
culture results, once validated by a biologist, are transmitted to the clinician for appropriate follow-up.
Conservation and Transportation
After collection, the blood culture bottles correctly identified (patient, department, date and blood culture number) are sent to the laboratory as soon as possible to be loaded onto the BACT/ALERT® machine. The maximum time between collection and introduction of the bottles into the machine is 24 hours.
Detection Method
The BACT/ALERT® system for blood culture detection operates in an automated manner. It ensures the incubation of the vials at an optimal temperature of 35°C, with constant agitation to promote bacterial growth. This system is equipped with sensors for continuous monitoring of each vial, performing scans every 10 minutes to detect the presence of microbial growth. When a culture is recognized as positive, the BACT/ALERT® system alerts laboratory personnel with a light and/or sound signal, signaling the need to examine the vial in question for additional analyses.
Identification of Bacteria
The samples are inoculated according to their nature and the infectious site on suitable culture media. Incubation is done at 37°C for 18 to 24 hours. The identification of bacterial strains was based on the study of morphological, cultural and biochemical characteristics (API 20E Gallery, etc.) or by the vitek-2 automaton (BioMérieux).
Antibiotic Sensitivity Study
The antibiogram is carried out either by the agar diffusion method (disc method), according to the press release from the antibiogram committee of the French Society of Microbiology (CA-SFM) or by the Vitek machine. The agar diffusion method is carried out using a bacterial suspension (Inoculum: 0.5 McFarland) seeded on the agar plates (Mueller-Hinton agar) then the antibiotic disks were placed on the surface of the agar plates, the boxes were incubated at 37°C for 18 to 24 hours. The different diameters of the inhibition zones obtained around the discs were measured using a ruler graduated in (mm) then interpreted as sensitive (S), Resistant (R) or Sensitive at High Dosage (SFP).
Results
Epidemiological Data Frequency
During the 26 months, the bacteriology laboratory of the CHN of Nouakchott received 212 blood cultures from various services with an average of 71 blood cultures per year. A total of 45 patients had positive blood cultures (a rate of 21.22%).
Distribution of Blood Cultures According to Their Type
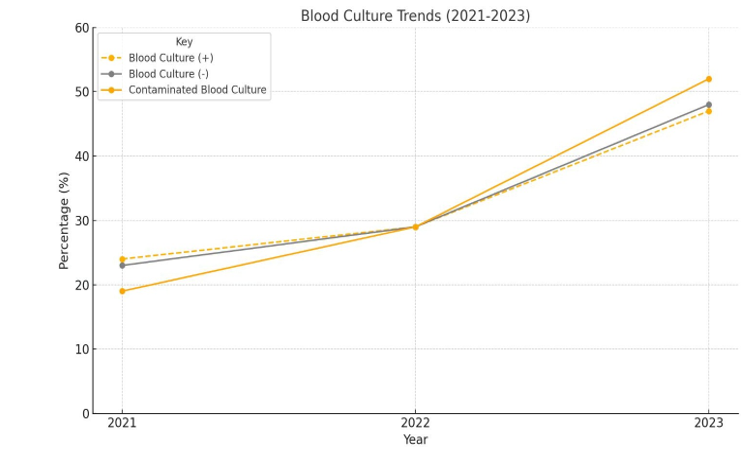
Among the blood cultures performed during the retrospective study, 21.22% were positive, while 68.88% were negative. Finally, contaminated blood cultures were 9.90% (Table 1).
| Year | 2021 | 2022 | 2023 | Total | % |
|---|---|---|---|---|---|
| Blood Culture (+) | 11 | 13 | 21 | 45 | 21.2 |
| Blood Culture (-) | 33 | 43 | 70 | 146 | 68.8 |
| Contaminated Blood Culture | 4 | 6 | 11 | 21 | 9.9 |
| Total | 48 | 62 | 102 | 212 | / |
Table 1: Annual status of blood culture requests and their outcomes.
Distribution of Blood Cultures by Sex
According to our investigation, the blood cultures were distributed between 120 male patients (i.e. a rate of 57%) and 92 female patients (i.e. a rate of 43%), i.e. an overall M/F sex ratio of 1.3. Among the patients with a positive blood culture, 29 patients were male (i.e. 64.4% of BC (+)) and 16 patients were female (i.e. 35.6% of BC (+)), i.e. one sex positive M/F ratio of 1.8. The annual and gender distribution of these blood cultures is shown in Table 2.
| Sex | 2021 | 2022 | 2023 | Global | % |
|---|---|---|---|---|---|
| M | 29 | 38 | 53 | 120 | 57 |
| F | 16 | 33 | 43 | 92 | 43 |
| Total | 45 | 71 | 96 | 212 | / |
Table 2: Annual distribution of blood cultures and their outcomes according to sex.
Positive blood cultures were distributed according to sex as shown in Table 3.
| Sex | 2021 | 2022 | 2023 | Global | % |
|---|---|---|---|---|---|
| M | 8 | 9 | 12 | 29 | 64.4 |
| F | 4 | 5 | 7 | 16 | 35.6 |
| Sex-ratio | 2 | 1.8 | 1.7 | 1.8 | / |
Table 3: Annual distribution of positive blood cultures by sex.
Figure 1 highlights the increase in demand, as well as the growth in vial positivity and contamination.
Bacteriological Data
Bacteriological Profiles
During the 26 months studied, out of the 45 positive blood cultures (representing a positivity rate of 21.22%), we isolated:
- Gram positive bacteria (Gram+) in 32 cases, or 71.12%.
- Gram negative bacteria (Gram-) in 12 cases, or 26.67%.
- Rarer cases of positive blood cultures with yeast, notably cases of candidemia (n = 1; 2.21%).
Table 4 Presents a distribution of microorganisms isolated from positive blood cultures identified in our study.
| Organism Category | Gram Stain | Number of Isolates | % in Group | Total | |
|---|---|---|---|---|---|
| Gram positive (n=32) | Staphylococcus aureus | Gram-positive cocci (GPC) | 18 | 56,25% | 32 |
| Gram positive (n=32) | Coagulase-Negative Staphylococcus (CoNS) | Gram-positive cocci (GPC) | 12 | 37,50% | 32 |
| Gram positive (n=32) | Streptococcus spp | Gram-positive cocci (GPC) | 2 | 6,25% | 32 |
| Gram negative (n=12) | Escherichia coli | Gram-negative bacilli (GNB) | 2 | 16,67% | 12 |
| Gram negative (n=12) | Klebsiella pneumoniae | Gram-negative bacilli (GNB) | 5 | 42.67% | 12 |
| Gram negative (n=12) | Proteus mirabilis | Gram-negative bacilli (GNB) | 1 | 8,33% | 12 |
| Gram negative (n=12) | Salmonella spp | Gram-negative bacilli (GNB) | 4 | 33,33% | 12 |
| Fungi (n=1) | Candida spp | Yeast | 1 | / | 1 |
Table 4: Groups of microorganisms isolated from positive blood cultures (n=45).
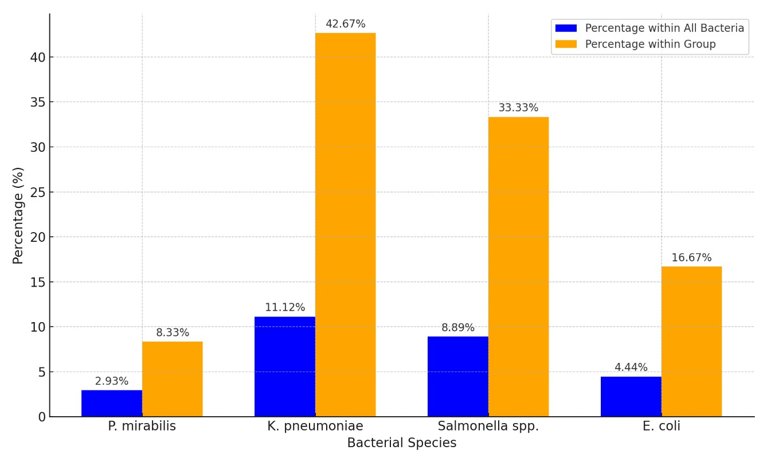
The reappearance of isolated enterobacteria is shown in Figure 2.
Distribution of Isolates by Sex
Table 5 shows the distribution of the different isolates between men and women with a sex ratio favoring men.
| Sex M | Sex F | M/F | |
|---|---|---|---|
| Staphylocoques aureus | 12 | 6 | 2 |
| Coagulase-Negative Staphylococcus | 7 | 5 | 1.4 |
| Streptococcus spp | 2 | 0 | / |
| E. coli | 1 | 1 | 1 |
| Klebsiella pneumoniae | 3 | 2 | 1.5 |
| Proteus mirabilis | 0 | 1 | / |
| Salmonella spp | 3 | 1 | 3 |
| Yeast | 0 | 1 | / |
Table 5: Distribution of the main bacterial groups according to sex.
Distribution of Blood Cultures According to Hospitalization Department
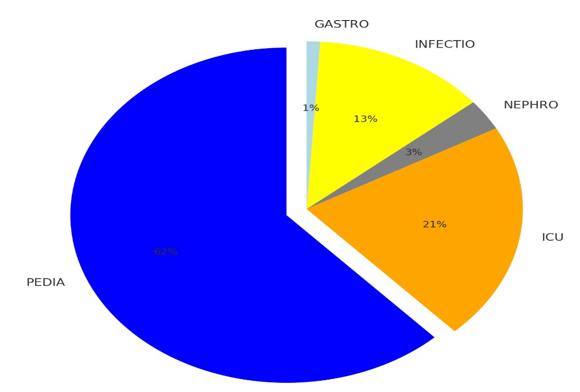
Table 6 represents the different origins of prescriptions depending on the clinical specialty, with individualization of high-demand services (Pediatrics, Intensive Care Unit, Infectious Diseases, Nephrology and Gastroenterology).
| Pediatrics | Intensive Care Unit (ICU) | Nephrology | Infectious Diseases | Gastroenterology | Total | |
|---|---|---|---|---|---|---|
| All BC | 132 | 44 | 6 | 27 | 3 | 212 |
| BC (+) | 28 | 9 | 2 | 5 | 1 | 45 |
| Percentage | 21,21% | 20,45% | 33,33% | 18,51% | 33,33% | 21,22% |
Table 6: Distribution of patients according to hospitalization department.
The distribution of services is shown in Figure 3.
Distribution of Blood Cultures According to Age
As part of our study on blood cultures performed, we identified a total of 212 cases. This population is divided into two main categories: 124 cases concern children (i.e. a rate of 58.5% of the study population), defined here as individuals aged from 1 day to 16 years and 88 cases concern adults (i.e. a rate of 41.5% of the study population).
Analysis of the positivity of blood cultures reveals that of the 45 positive cases, 28 cases were children (i.e. a rate of 62.2% of positive HC), while 17 cases were adults (i.e. a rate of 37.8% of positive BC).
Antibiotic Resistance Profile
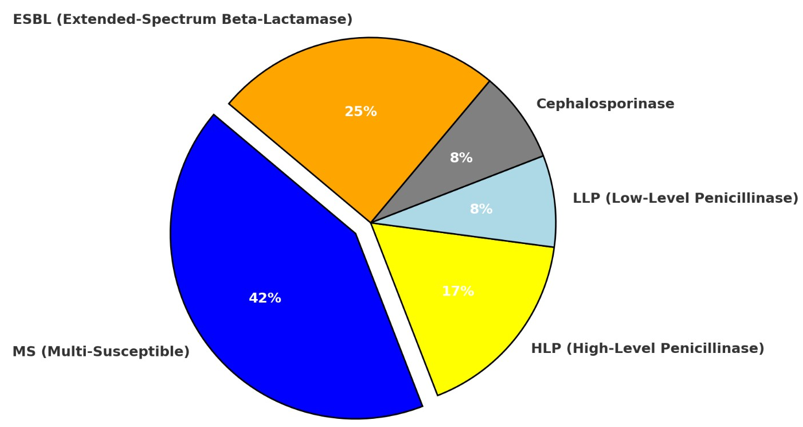
Enterobacteriaceae (n=12) presented variable resistance profiles to beta-lactams (BLA). The acquired enzymatic resistance was as follows: Low-level penicillins (LLP): 1; High-level penicillins (HLP): 2; Low-level cephalosporinase (LLC): 1; High-level cephalosporinase (HLC): 0 and ESBL: 3 strains. A total of 5 strains were fully susceptible (4 Salmonella spp and 1 E. coli) (Table 7).
| E coli | Klebsiella Pneumoniae | Proteus Mirabilis | Salmonella Spp | Total | |
|---|---|---|---|---|---|
| ESBL (Extended-Spectrum Beta-Lactamase) | 1 | 2 | 0 | 0 | 3 |
| Cephalosporinase | 0 | 1 | 0 | 0 | 1 |
| LLP (low-level penicillinase) | 0 | 0 | 1 | 0 | 1 |
| HLP (high-level penicillinase) | 0 | 2 | 0 | 0 | 2 |
| MS (Multi-Susceptible) | 1 | 0 | 0 | 4 | 5 |
| Total | 2 | 5 | 1 | 4 | 12 |
Table 7: Distribution of EB resistance profiles to beta-lactams.
Figure 4 shows the distribution of EBs according to their BLA resistance profiles.
The resistance rate of Staphylococci aureus to penicillin M (PM) was on average 44.44%, or 8 out of 18 cases. No resistance was detected against glycopeptides, aminoglycosides or fusidic acid (FA). On the other hand, 88.88% of the strains presented resistance to penicillin G (PG), or 16 out of 18 cases.
Figure 5 illustrates the rates of staphylococcus aureus resistance to antibiotics.
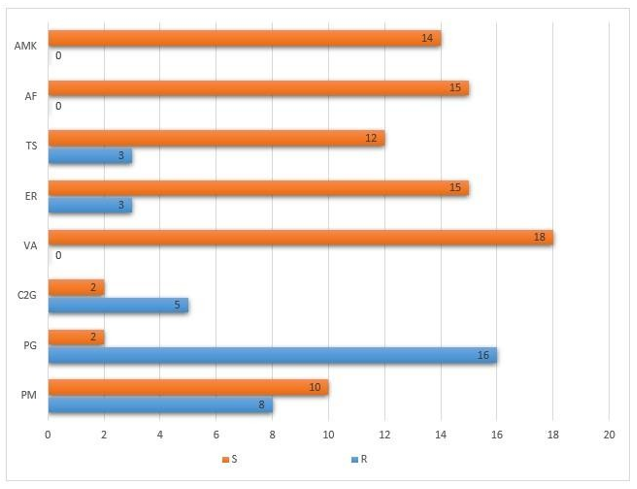
Legend: PG: penicillin G; PM: penicillin M; ER: erythromycin; A.F:(fusidic acid); C2G (2nd generation cephalosporins); AMK: (amikacin); VA: (vancomycin); TS: (trimethoprim/sulfamethoxazole).
Discussion
On the Epidemiological Level Distribution of Blood Cultures According to Their Type
During the 26 months of our study, 212 blood cultures were performed and recorded at the CHN bacteriology laboratory. The proportion of positive blood cultures was 21.22%, while that of negative blood cultures was 68.88% and contamination represented only 9.90%. Our positivity rate was superimposable with that reported in a study conducted in Morocco in 2020 by LIGATI A [9], where the positivity rate was 21.1%; while it was higher than the rates noted in other regions, such as at the Souro Sanou University Hospital Center (SSUHC) of Bobo-Dioulasso in Burkina Faso, where Lankoande [10] reported a rate of 13.58% in 2002 and also a study in Cameroon carried out between 2006 and 2011 by Ebongue, et al. [11] who recorded a positivity rate of 12.8%.
Previous studies at Dakar University Hospital revealed variable rates over the years, with 24.5% in 1980 [12], 14.7% in 1986 [13], 19.81% in 1988 [14], and a decreased to 12.6% in 2002 [15]. These variations highlight the evolution of epidemiological profiles and diagnostic capabilities over time. In contrast, a study conducted in Algeria in 2017 found a considerably high positivity rate of 31.48% [16]. These variations in positivity rates could be attributable to the difference in the method used to obtain blood cultures in the various studies. Automated systems appear to produce more positive results than traditional manual methods [10].
In our study, there were many more isolates in 2023. This could be explained by an improvement in the conditions for practicing blood cultures and especially by the large number of samples taken during this year.
Table 8 represents the positivity rate compared to the literature.
| Pays | Year | Positivity Rate | |
|---|---|---|---|
| Boukerouaz A, et al. [16] | Algeria | 2017 | 31,48% |
| Akkoua-Koufi C, et al. [17] | Ivory Coast | 2015 | 22.50% |
| Gupta S, et al. [18] | India | 2016 | 16,50% |
| Bhandari P, et al. [19] | Nepal | 2015 | 15,40% |
| Eshetu S BitewA, et al. [20] | Ethiopia | 2018 | 15,20% |
| Banik A, et al. [21] | India | 2018 | 14,24% |
| Mnif C [22] | Ethiopia | 2017 | 10% |
| Lakhe N, et al. [23] | Senegal | 2018 | 4,10% |
| Our Study | Mauritania | 2023 | 21,22% |
Table 8: Positivity rate compared to literature.
During our study period, the rate of negative blood cultures was significant, with 146 cases, representing 68.88% of all blood cultures performed. This result was lower than those reported by the study conducted by Ebongue, et al. [11] in Cameroon between 2006 and 2011, where a negativity rate of 75% was reported. Similarly, in the study by Sangare SA, et al. [24] carried out at a pediatric hospital in Bamako in Mali, the blood culture negativity rate was 80.04%. These high levels can be due to several factors, including the absence of bacteria in the blood, sepsis caused by an etiology other than bacterial (viral, tuberculous, rickettsiae, chlamydia, etc.) or even causes of failure in the blood culture procedure:
- Sample taken too late in the course of the illness.
- A poorly made diagnosis.
- Failure to comply with quality sampling conditions.
- Quantity of blood seeded in the medium too low.
- Culture media or conditions that do not cover a germ in question.
- Insufficient observation time for culture media: an observation period of 10 days is necessary to declare a blood culture negative.
- Blood cultures neutralized by antibiotics: antibiotic therapy introduced before taking blood cultures represents a major cause of their negativity. Its frequency is high in all series [25].
The contamination rate at the CHN bacteriology laboratory in our study was 9.9%. One of the most common challenges observed was contaminated samples due to improper aseptic techniques during blood collection. For example, in multiple cases, Coagulase-Negative Staphylococci (CoNS) were isolated from cultures but later identified as likely contaminants due to their presence in repeated samples. This resulted in delayed diagnosis and unnecessary antibiotic treatments, emphasizing the need for better sterile techniques during sample collection.
Additionally, some samples contained insufficient blood volume, reducing the detection sensitivity for low- bacterial- load infections. In at least five instances, patients initially tested negative due to small sample sizes but later had positive cultures when blood volume collection was increased. This highlights the importance of ensuring adequate blood sample volume to enhance diagnostic accuracy.
Finally, delayed transport of blood cultures to the laboratory was another issue identified. In a few cases, samples were stored for prolonged periods before processing, leading to false-negative results. To mitigate this, strengthening logistics for faster sample transport and immediate incubation in the BACT/ALERT® system is essential to improve culture efficiency.
This rate is above that recorded by Samson AB [26] at the Rouen University Hospital Center, which was 1.30%. Studies carried out in Algeria in 2019 by Aidoun M, et al. [27], as well as in Morocco by Ligati A [9] in 2020, respectively reported contamination rates of 3% and 4%. Furthermore, research carried out in Mali by Sangare SA, et al. [24] identified a rate of 12.8%. These data highlight the importance of adopting optimal practices in the collection and processing of samples for bacteriological culture to reduce the risk of contamination.
Incidents of contamination remain common and mainly come from bacteria belonging to the resident flora of the patient, that of the staff taking the samples, or even the environment. Among the microorganisms frequently involved, although some can be pathogenic in specific contexts, include coagulase-negative Staphylococcus, Bacillus species, Corynebacterium, as well as Propionibacterium acnes. This reality highlights the crucial importance of adopting rigorous sample collection and handling methods, in order to minimize the risks of contamination when carrying out bacteriological cultures [26].
Distribution of Cases of Bacteremia According to Sex
In our study, the observation of a male predominance among the cases analyzed is manifested by a sex ratio of 1.3 men for each woman. This finding resonates with similar research findings. Notably, the study conducted by Boukerouaz, et al. [16], in 2017, at the Benabadji University Hospital Center in Constantine, highlighted a sex ratio of 1.28, highlighting a trend comparable to ours. By elsewhere, this male predominance also aligns with the results of a survey carried out in 2020 at the military hospital of Meknes, Morocco by Ligati A [9], which revealed a sex ratio of 2.1, and another study in Ivory Coast, reporting a sex ratio of 1.9. Although the general trend reveals a predominance of men, variations in sex ratio as well as cases of slight female predominance in the work of Lakhe N, et al. [23] in Senegal and Eshetsu S, et al. [20] in Ethiopia, with sex ratios of 0.79 and 0.83 respectively, illustrate the complexity and diversity of factors influencing the distribution of infectious diseases between sexes.
Indeed, most infectious diseases appear to be distributed unequally between the two sexes. This sexual dimorphism is confirmed by several epidemiological studies highlighting a male predominance among patients with sepsis. However, differences related to occupational exposures and lifestyle are important factors explaining this dimorphism between the two sexes. Additionally, genetic and hormonal variations also play a significant role [19].
On the Bacteriological Level
Distribution of Blood Cultures According to the Causative Agent
As part of our research, it was found that cases of sepsis are mainly caused by bacteria, representing 97.78% of occurrences, while yeasts are responsible for a minority of cases, i.e. 2.22%. This trend is corroborated by the results of previous studies, notably those carried out by Lakhe N, et al. [23]. in 2016, Ligati A [9] in 2020., as well as by Aidoun M and Boulazerg AF in 2019 [27], who all highlighted a dominance of bacterial agents in cases of sepsis.
Overall Distribution of Positive Blood Cultures According to Bacterial Strains
In our study, Staphylococcus aureus was identified as the most frequently encountered pathogen in blood culture, with a prevalence of 40%. This rate is significantly higher than that observed in a study conducted in Algeria in 2019 by Aidoun M and Boulazerg AF [27], where the rate was only 22.8%. However, comparing our results to those obtained in other studies in Morocco, although our rates are different, we observe a similar trend regarding the predominance of Staphylococcus aureus in blood cultures. Indeed, the study by Ligati A [9] in 2020 revealed a prevalence of 31%, and that of Zougaghi, et al. [28] in 2011 reported a rate of 21.3%. Other studies, such as those of Lakhe N, et al. [23] and Gupta S, et al. [18] showed even lower rates of 10.75%
and 18.30% respectively, while Banik A, et al. [21] recorded a slightly higher rate of 42.14%. These observations highlight the marked predominance of Staphylococcus aureus in bacteremic infections across different regions, although the frequency may fluctuate slightly between studies. Staphylococcal isolates were dominated by S. aureus, followed by coagulase-negative Staphylococcus CoNS (26.66%). Other studies reported a predominance of S. aureus 49.1% compared to CoNS 27.2% [29]. In Cameroon, staphylococcal isolates consisted of 36% CoNS and 64% S. aureus [11]. The difference observed may also be linked to the fact that some studies only focus on one service, while others focus on all the services of a hospital [11].
As part of our study on enterobacteria, Klebsiella pneumoniae was found to be the dominant species, with a rate of 11.12%. This result is close to that reported by Agnihotri [30], who found a rate of 12.3% for this same species. Research carried out in Mali by Maïga, et al. [29] revealed a slightly higher rate of 15.43% for K. pneumoniae, while the study by Aidoun M and Boulazerg AF [27] documented an even higher rate of 17.54%. Unlike our study, Boukerouaz in 2017 [16] noted a predominance of E. coli (19.1%) followed by K. pneumoniae (6.1%). In France, Krir, et al. in 2019 [31] noted a frequency of 9.6% for K. pneumoniae.
Distribution of Bacterial Strains According to their Gram
In our microbiological analysis, bacterial cultures revealed a significant predominance of Gram-positive bacteria, constituting 73% of the isolates, compared to 27% for Gram-negative bacteria. This distribution However, our observations agree with those of Derabli, et al. [32] in 2016 who documented a distribution of 64% for Gram-positive bacteria compared to 36% for Gram-negative bacteria. On the other hand, studies by Radha Rani, et al. [33] in 2017 and Maïga, et al. [29] in 2004 in Mali highlighted a prevalence of Gram-negative bacteria, with respectively 53.8% and 59.51% of isolates, as opposed to 46.1% and 39.45% for Gram-positive bacteria. This divergence in the predominance of bacterial groups highlights the variability of microbiological profiles depending on geographic and temporal contexts.
The disparity observed between these different studies highlights the importance of continuous microbiological monitoring adapted to each context for a better understanding of infectious dynamics. The predominance of Gram-positive bacteria in our study compared to other regions may reflect local epidemiological specificities, differences in clinical practices or the populations studied. In conclusion, these results contribute to enrich the global database on the distribution of bacterial pathogens, providing essential insights for the development of strategies for the prevention and treatment of bacterial infections.
Distribution of Blood Cultures According to Hospitalization Department
In our study, we observed a different distribution of positive blood cultures among hospital departments compared to the study by Ebongue, et al. [11] in 2014. While in our research, the pediatric department represented a higher prevalence, with 62% of cases, followed by intensive care with 21%, infectious diseases with 13%, nephrology with 3%, And gastrology with 1%, the previous study indicated that 49.7% of cases came from the pediatrics department, 22.4% from the internal medicine department, and 8.4% from the intensive care unit. These discrepancies in the distribution of positive blood cultures particularly highlight a high prevalence of bloodstream infections in the pediatric department in our research, potentially reflecting significant dynamics of exposure to pathogens among children in our hospital setting.
Antibiotic Resistance Profile
The resistance of the different bacterial strains isolated was evaluated against a variety of antibiotics. This resistance varies depending on the intensity of antibiotic use in each health establishment and the presence in the environment of genetic material favoring the emergence of resistant strains [34].
Staphylococcus Resistance
Staphylococci are well known to be difficult pathogens to treat due to their ability to develop various antibiotic resistance mechanisms, making them a constantly growing public health problem [35]. The results of our study reveal that 40% of cases of bacteremia were attributable to Staphylococci aureus. Methicillin-resistant Staphylococcus aureus (MRSA) represented 44.44% of AS isolated in our study. This rate is higher than the results obtained in the study carried out in 2020 at the Avicenne military hospital in Marrakech by Safi J [36], which had established a MRSA rate of 17.82%. Comparing our result to that of work carried out in Morocco, we note a slight drop in the MRSA rate, going from an overall rate of 33.33% between 2011 and 2013 to 29.6% between 2015 and 2018 [37]. In various international studies, MRSA rates exceed 40% [12, 20, 23]. In France, information collected by the EARSS-Net (European Antimicrobial Resistance Surveillance Network) corroborates this trend by showing a constant decline in methicillin resistance in Staphylococcus aureus, going from 33% in 2002 to 13% in 2017 [38]. These data highlight the increased effectiveness of initiatives put in place at European level to reduce the rate of MRSA.
In our study, Staphylococci aureus showed high resistance to penicillin G (88.88%). A low rate of resistance was recorded for cotrimoxazole and erythromycin. These bacteria are sensitive to vancomycin, amikacin and fusidic acid, with sensitivity results of 100% for each of these antibiotics. Lankonade H [10] from Burkina Faso noted similar results for penicillin G (86.5%) and high sensitivity to fusidic acid. The sensitivity rates to 2nd generation cephalosporins and pristinamycin are very close to our results. Furthermore, Decousser, et al. [39] from Madagascar in 1999 reported that more than 80% of strains of Staphylococci aureus are resistant to penicillin Derabli G, et al. [32] in 2016 recorded a sensitivity of 100% for vancomycin, with a resistance rate of 70% for erythromycin. The high rates of resistance to penicillin G are explained by the fact that currently most Staphylococci aureus possess penicillinase, an enzyme capable of hydrolyzing all penicillins except oxacillin and cloxacillin [31].
Enterobacteriaceae Resistance
Enterobacteriaceae are dominated in our study by Klebsiella pneumoniae with a frequency of 11.11%, or 5 out of 45, followed by Salmonella spp at 8.89%, or 4 out of 45. Escherichia coli has a frequency of 4.44%, i.e. 2 in 45, and finally, Proteus mirabilis has a frequency of 2.22%, i.e. 1 in 45. These results differ of those obtained by Boukerouaz, et al. [16] in 2017, who found that 19.1% are E. coli and 16.6% are K. pneumoniae. The rate of ESBL-producing enterobacteria (ESBL-E) is close to 25% in our study. The rate of ESBL- producing E. coli that we observed (50%) is higher than that reported by Maman R, et al. In Meknes who found a rate of 23.52% in his study in 2015 [37], and also higher than that identified by Zidouh. A in Marrakech 14.28% in 2019 [40]. This rate also exceeds that recorded by EARS-Net in France (10.2%) in 2017 [38]. However, studies carried out in other countries have revealed rates higher than ours, notably in India (68.8%) [18] and Senegal (71.5%) [23].
In our survey, the prevalence of ESBL-producing Klebsiella strains was 40%. This rate is lower than that observed in other research studies, where significantly higher prevalences have been documented: 60% in Marrakech according to data from Zidouh [40], 59% in France according to figures published by the EARS-Net in 2017 [38], and rates above 80% were recorded in Algeria, India, and Ethiopia [18, 20, 32]. This shows that in our establishment, E. coli is mainly concerned by the production of ESBLs, which corresponds to the observations made by Ligatti in Morocco in 2020 [9]. On the other hand, the previously mentioned research mainly highlights the prevalence of K. pneumoniae. High-level resistance to cephalosporins by hyper-produced cephalosporinase (HPC) was not noted in this study, particularly in Enterobacteria. High rates are reported by other studies: 27.27% in Morocco (Marrakech) [40], 50% in Senegal [23] and India [18] and 80% in Ethiopia [20]. Therefore, the HLC profile is not a problem in our establishment. High-level resistance to penicillins by hyper- produced penicillinase (HPP) was 40% for K. pneumoniae in other countries the resistance of the main enterobacteria to HLP exceeds 50% [20, 23, 32]. The Salmonella spp strains isolated (33.33% of EBs and 8.89% of all bacteremias) are all multi-susceptible.
No Enterobacteriaceae strain in our study was carbapenem resistant (CRE). Carbapenems are the molecules of choice in the treatment of E-ESBL infection in combination with amikacin. However, it is essential to emphasize their careful use [40].
The Streptococcal isolates do not present any acquired resistance, the results of this work match those found by Maman R in 2015 [41]. In our research, we detected only one case of candidemia caused by Candida spp, representing a rate of less than 3%. This result is consistent with that of a study carried out in Meknes in 2015 [41]. The patient, a premature neonate in the Pediatric Intensive Care Unit (PICU), presented with persistent fever and signs of septicemia, unresponsive to broad-spectrum antibiotics. Following blood culture confirmation of Candida spp., systemic antifungal therapy with fluconazole was initiated, leading to clinical improvement. This highlights the need for clinicians to consider fungal infections in high-risk patients, such as neonates, immunocompromised individuals, and those with prolonged hospital stays. Early recognition and targeted antifungal therapy are crucial to improving patient outcomes and reducing morbidity associated with candidemia. The presence of Candida spp in a blood culture is considered a direct indicator to initiate systemic antifungal treatment without delay [38, 42].
Conclusion
Bloodstream infections play a major role in increasing mortality and morbidity rates, particularly in hospital settings. Their progression can prove fatal without the intervention of immediate and well-targeted antibiotic therapy. Furthermore, faced with the growth of antibiotic resistance, it becomes essential to regularly update the epidemiological profile of pathogens and evaluate their resistance to treatments. This step is crucial to adjust and optimize the use of antibiotics from the early stages of bacteraemia management, thereby improving health outcomes for patients. Our study made it possible to produce a description of the bacteriological profile and resistance of the bacteria responsible for bacteraemia at the bacteriology laboratory level of the Nouakchott CHN over a period of 26 months (ranging from 2021 to 2023). The retrospective study of blood cultures at the CHN bacteriology laboratory reveals that:
- Positive blood cultures represent 21.2% of all blood cultures;
- Positive samples mainly concern male subjects (64.4%) and subjects hospitalized in the pediatric department (62%);
- The bacteriological (etiological) study of blood cultures made it possible to identify 45 bacterial strains:
- For Gram-positive bacteria, the highest rates were observed with Staphylococcus aureus and coagulasenegative Staphylococcus with percentages of 40% and 26.67% respectively.
- The Klebsiella pneumoniae species is dominant for Gram-negative bacteria with a rate of 42.67%;
- In terms of sensitivity of germs to antibiotics:
- Staphylococci have high resistance to penicillin G and fairly high sensitivity to glycopeptides; aminoglycosides and fusidic acid.
- Enterobacteriaceae show high resistance to many antibiotics but good sensitivity to imipenem and colistin.
Knowledge of the epidemiology and antibiotic sensitivity of blood culture isolates is essential for the implementation of first-line antibiotic therapy adapted to resistance phenotypes. Indeed, in practice, the initial treatment often remains probabilistic while awaiting guidance on the first results of the blood culture and then the antibiogram.
Recommendations
At the end of this work, we recommend: To Prescriptors: When to Prescribe Blood Culture
- Any fever of undetermined origin, especially if it is accompanied by signs suggestive of infection, should give rise to blood cultures.
- In particular, they will be carried out in the following circumstances:
- If the patient’s temperature is above 38.5°
- If the temperature is below 36.5°
- If there are chills, sweats
- Faced with an unexplained shock
- Systematically in certain contexts such as the notion of infectious risk in the newborn or in profoundly immunocompromised patients (neutropenic for example)
- In certain cases, to monitor the effectiveness of an anti- infective treatment
- Blood cultures should be collected if possible, before any treatment.
- It is unnecessary, and a source of waste, to multiply the number of blood cultures. In practice, you should limit yourself to 2 or 3 samples per 24 hours, taken at the time of fever peaks or chills. It is recommended to wait 15 to 60 minutes between 2 samples.
How to Do A Blood Culture
- Take during a febrile peak or the chill that precedes it, if possible, before any antibiotic treatment.
- There is no indication to repeat the samples before 48 hours of incubation of the first series of blood cultures taken unless a new clinical outbreak appears.
- Blood culture is a blood sample requiring rigorous asepsis.
- Paste the bottle barcodes on the request sheet.
- Note the date and time of the blood culture and the collection site on the request sheet.
- In the event of sampling from a catheter or any other implantable material, it is imperative to report this on the examination request form.
- Perform antisepsis on the bottle caps.
- Fill each bottle with 5 to 10 ml of blood: there are marks on the bottles, do not exceed the upper mark.
- Note essential clinical information (allows the laboratory to optimize culture conditions):
- Patient temperature
- Any current antibiotic treatment
- Suspicion of possible endocarditis
- Each stage of the examination (positive microscopic examination, identification, sensitivity assessment) must be transmitted in real time to the clinician as soon as they are validated.
- Do not hesitate to ask the laboratory for the follow- up given to a blood culture. This incentive means that everyone (clinicians and biologists) must carry out their task, within a framework of mutual respect, of course.
Prescription of Antibiotics and Avoidance of Self- Medication
- Reasoned prescription of antibiotics: Antibiotics must be prescribed only in cases of clear and confirmed indication, in order to prevent the emergence of bacterial resistance.
- Avoid self-medication: make your patients aware of the risks associated with the inappropriate use of antibiotics, such as ineffectiveness, bacterial resistance and side effects.
- Any decision on antibiotic treatment must be based on clinical data, additional examinations (including blood cultures), and current national recommendations.
To Health Authorities To improve blood cultures, health authorities should recommend strict methods for sample collection and analysis, regularly train medical staff in good sterile collection practices, and facilitate communication between clinicians and laboratories. It would also be important to make blood culture bottles available in all health structures and to equip hospitals with machines. This would ensure accurate and rapid results, benefiting patients with potentially serious infections.
References
-
Bool M, Barton MJ, Zimmerman PA (2020) Blood culture contamination in the emergency department: An integrative review of strategies to prevent blood culture contamination. Australas Emerg Care 23: 157-165.
-
Gunvanti R, Lakshmi JT, Kamlakar S, Sakthivadivel V, Archana G, et al. (2022) Blood culture contamination rate as a Quality Indicator - a Prospective Observational Study. Maedica 17: 311-316.
-
Fabre V, Carrol KC, Cosgrove SE (2022) Blood culture utilization in the Hospital Setting: A Call for Diagnostic Stewardship. J Clin Microbiol 60: e0100521.
-
Lippi G, Cervellin G (2018) Diagnosis and management of bloodstream infections: A Paradigm Shift. J Clin Pathol 71: 781-785.
-
Luz ZMP (1999) Changes in the haemoculture methodology improve the test positivity. Mem Inst Oswaldo Cruz 94: 295-298.
-
Hagiya H, Yoneda N, Kimura K, Mitsui T, Ueda T (2019) Clinical impact of extended blood culture examination: Too much of a good thing. J Infect Chemother 25: 559- 562.
-
Velasco R, Fernandez JL, Campo MN, Puente S (2014) Evaluation of haemoculture extraction technique in an emergency department: Nursing Staff Self-Perception and Reality. J Emerg Nurs 40: 36-38.
-
Gonzalez MD, Chao T, Pettengill MA (2020) Modern blood culture: Management Decisions and Method Options. Clin Lab Med 40: 379-392.
-
Lankonade H (2002) Epidemiological, diagnostic, therapeutic and prognostic aspects of septicemia at the C.H.N.S.S of Bobo Dioulasso about 522 cases. Medicine thesis: The Ouagadougou University, Burkina Faso 167: 81.
-
Akoua KC, Tia H, Plo JK, Monemo P, Cissé A, et al. (2015) Epidemiology of community-onset bloodstream infections in Bouaké, central Côte d’Ivoire. New microbes and new infections 7: 100-104.
-
Ebongue CO, Mefoo JN, et al. (2006) Bacteriological profile and antibiotic sensitivity of blood culture isolates in Douala, Cameroon. Malian Journal of Infectiology and Microbiology 8: 27-39.
-
Djoffon O (1980) Assessment of bacterial samples in the Dakar university hospital environment. Medicine thesis: CHU-Dakar 33: 67.
-
Dourwe JC (1986) Computerized assessment of the activities in 1985 of the Le Dantec University Hospital laboratory. Pharm thesis: CHU-Dakar 56: 58.
-
Thioub C (1988) Sepsis at the C.H.U. by Fann. 3-year review of the Bacteriology - Virology Laboratory. Medicine thesis: CHU-Dakar 79: 86.
-
Diallo HM (2002) Bacteremia: epidemiological and bacteriological aspects of the germs responsible for bacteremia in the bacteriology - virology laboratory of the Fann University Hospital from 1996 - 2000. Medicine thesis: University Hospital-Dakar 56: 66.
-
Lakhe NA, Sylla K, Mbaye KD, Ndiaye R, Diallo V, et al. (2018) Bacteremia: Profile and Antibiotic Resistance at the Infectious and Tropical Diseases Clinic in Fann Hospital, Dakar, Senegal. J Infect Dis Ther 6: 348.
-
Sangare SA, Maiga AI, Dicko TF, et al. (2014) Evaluation of the Binax NOW® ICT Streptococcus pneumoniae screening test from blood cultures performed in children with invasive bacterial infections in Bamako, Mali. Malian Journal of Infectiology and Microbiology 11: 38-47.
-
Ligati A (2020) Microbiological aspects and antibiotic resistance of bacteria isolated from blood cultures at the Moulay Ismail military hospital. Medicine thesis: HMMI- Meknes 78/20: 88.
-
Bhandari P, Manandhar S, Shrestha B, Dulal N (2016) Etiology of bloodstream infection and antibiotic susceptibility pattern of the isolates. Asian Journal of Medical Sciences 7: 71-75.
-
Boukerouaz A, Benmehidi R (2017) Bacteriological profile of Gram-negative bacilli bacteremia. Master’s thesis: University of the Mentouri Constantine Brothers - Faculty of Natural and Life Sciences, pp: 112.
-
Banik A, Bhat SH, Kumar A, Palit A, Snehaa K (2018) Bloodstream infections and trends of antimicrobial sensitivity patterns at Port Blair. Journal of laboratory physicians 10: 332-337.
-
Martin C, Denis F, Poly MC, Bingen E, Quentin R (2011) Medical microbiology. Elsevier Masson 78: 631-638.
-
Manif B (2017) Positive blood cultures: results of the prospective multicenter study. Antibiotic resistance in Tunisia (LART) 7: 22-43.
-
Bitew A (2018) Multi-Drug resistance profile of bacteria isolated from blood stream Infection at Tikur Anbessa Specialized Hospital, Addis Ababa, Ethiopia. EC Microbiology 149: 119-126.
-
Gupta S, Kashyap B (2016) Bacteriological profile and antibiogram of blood culture isolates from a tertiary care hospital of North India. Too J Med Res 19: 94-99.
-
Samson AB (2018) Retrospective study of blood cultures performed at the University Hospital of Rouen between January and June 2017 and analysis of different quality indicators. Pharmacy Doctorate Thesis: University of Rouen Normandy, France, pp: 132.
-
Bannik A, Bhat SH, Kumar A, Palit A, Snehaa K (2018) Bloodstream infections and trends of antimicrobial sensitivity patterns at Port Blair. Journal of laboratory physicians 10: 332-337.
-
Aidoun M, ET Boulazerg AF (2020) Retrospective study of positive blood cultures at HMRUC: review of the year 2019 of the bacteriology laboratory. Master’s thesis: University of the Mentouri Constantine Brothers - Faculty of Natural and Life Sciences, pp: 110.
-
Krir A, Dhraief S, Messadi A, Thbat L (2019) Bacteriological profile and antibiotic resistance of bacteria isolated in an intensive care unit over seven years. Annals of browns and fire disasters 23(3): 197-202.
-
EL-Khiyat M (2017) Neonatal bacteremia. Bacteriological profile and antibiotic resistance. Medical diploma thesis in Medical biology: Sidimohammed Ben Abdellah University, Morocco 98: 50.
-
Agnihotri N, Kaistha N, Gupta V (2004) Antimicrobial susceptibility of isolates from neonatal septicemia. Jpn J Infect Dis 57: 273-275.
-
Derabli B, Tiaounine M (2016) Epidemiological profile of nosocomial sepsis at the University Hospital and HMC 2014-2016. Master’s thesis in General Microbiology and Molecular Biology of Microorganisms. Constantine: University of the Mentouri Brothers Constantine, Algeria, pp: 74.
-
Maiga I, Sidebe M, Maiga A, Rochereau A (2004) Bacteria isolated by blood cultures at the “G” point hospital. Medical Mali 333: 18-23.
-
Dumitrescu O, Dauwalder O, Vandenesch F (2010) Résistance aux staphylococcus aureus. Med Sci Paris 26: 943-949.
-
Zougaghi L, Soraa N, Zahlane K, et al. (2011) Epidemiology and sensitivity profile of blood culture isolates in a Moroccan university hospital center. Tunisian Journal of Infectiology 5: 78-81.
-
Safi J (2018) Antibiotic consumption and bacterial resistance at Ibn Tofail Hospital. Thesis Doctorate in medicine, Faculty of Medicine and Pharmacy of Marrakech 93: 114.
-
Maman R, Louzi L (2015) Epidemiological profile of bacteremia at the My Ismail military hospital in Meknes. Retrospective study over three years (2011-2013). Doctoral thesis in pharmacy from the Faculty of Medicine and Pharmacy of Rabat- Mohamed V University, Morocco.
-
Décousser JW, Pfister P, Xueref X, Rakoto-Alson O, Roux JF (1999) Acquired antibiotic resistance in Madagascar: first evaluation. Med Trop (Mars) 59(3): 259-265.
-
Zidouh A, Arsalane L (2019) The bacteriological profile of bacteremia and the state of antibiotic resistance. Doctoral thesis in medicine: Faculty of Medicine and Pharmacy, Cadi Ayyad University Marrakech, Morocco 219: 108.
-
Maman R, Louzi L (2015) Epidemiological profile of bacteremia at the My Ismail military hospital in Meknes. Retrospective study over three years (2011-2013): Doctoral thesis in pharmacy from the Faculty of Medicine and Pharmacy of Rabat- Mohamed V University, Morocco.
-
Rani DR, Chaitanya BS, Rajappa JS, Kumar RB, Prabhakar KK, et al. (2017) Retrospective Analysis of Blood Stram Infections and Antibiotic Susceptibility Pattern of Gram- Negative Bacteria in a Tertiary Care Cancer Hospital. International Journal of Medical Research & Health Sciences, pp: 19-26.
-
Achekour Z (2012) Emergence of resistance to carbapenems in gram-negative bacilli. Doctorate thesis in pharmacy: Mohammed V University of Casablanca, Morocco 87: 60.
- Antifungal Activity of New Acetophenone Derivatives
- Interconnected Microbiomes Human Health Within an Environmental Framework
- Silkworm-Based Vaccine Production for H5N1: A One Health Approach to Pandemic Preparedness
- Microbial Diversity and Lipolytic Activity of Bacteria and Fungi from Oil-Contaminated Sites in Makurdi Metroplois
- Antibiotic Resistance Profile of Bacteria Isolated at the Central Laboratory of the National Hospital Center of Nouakchott
- Immobilization of Trametes Versicolor Laccase onto Silica Aerogel via Covalent Attachment Method