Antibiotic Resistance Profile of Bacteria Isolated at the Central Laboratory of the National Hospital Center of Nouakchott
This retrospective study aims to analyze the antibiotic resistance profiles of bacteria isolated at the central laboratory of the National Hospital Center of Nouakchott, Mauritania, over a period of two years (January 2020 - December 2021). A total of 511 non-duplicated clinical isolates were examined, from a diverse range of biological samples, including urine, pus, genital swabs, puncture fluids and blood cultures. All samples were taken from hospitalized and ambulatory patients in Nouakchott and only those with complete identification and sensitivity profiles were included. Gram-negative bacteria (GNB) accounted for 78.3% of isolates, while Gram-positive cocci (GPC) accounted for 21.7% of strains. GNB were mainly represented by enterobacteria (98.0%), and Escherichia coli was the most frequently isolated species (54.8%). The Gram-positive cocci were mainly Staphylococcus aureus (17.8%). Susceptibility testing was performed using the VITEK® 2 system and agar diffusion methods in accordance with EUCAST and CA-SFM recommendations. They revealed alarming levels of resistance to commonly used antibiotics. E. coli showed 80.1% resistance to extended spectrum beta-lactamases (ESBLs) and 33.6% resistance to ciprofloxacin, with 13.2% of isolates producing extended- spectrum beta-lactamases (ESBLs). K. pneumoniae showed an increasing prevalence and increasing resistance to third-generation cephalosporins and carbapenems. It also showed reduced efficacy on all methicillin species. The prevalence of ESBL in this species was 23.9% and its resistance to third-generation cephalosporins and carbapenems increased (4.8%). In the face of rising resistance, the study recommends rational use of antibiotics, reinforced microbiological surveillance and awareness-raising among medical staff and the general public to limit self-medication and the spread of multi-resistant bacteria.
Introduction
Antibiotics are drugs used to treat and prevent bacterial infections. Antibiotic resistance in a bacterium is defined as the absence of effect of an antibiotic to which the bacterial species is naturally susceptible, i.e. for which a therapeutic effect is expected during treatment at the usual dose [1, 2]. Bacterial resistance to antibiotics is a major public health issue. Bacterial resistance has been on the rise for several decades, making it difficult to treat patients. It increases the length of treatment and morbidity associated with infections, and can be life-threatening. In parallel with this increase in resistance, the number of new antibiotics available has fallen drastically over the last few decades, particularly those with new classes or mechanisms of action [3]. The aim of this study was to evaluate the resistance profile of the various germs isolated at the central laboratory of the Centre Hospitalier National de Nouakchott.
Materials and Methods
Sample Collection
Our samples were collected at the bacteriology laboratory of the Centre Hospitalier National de Nouakchott;
Patients come from all the medical facilities in the city of Nouakchott: private facilities, outpatient clinics and the hospitalization departments of the various hospitals. Study period: Our study was spread over a two-year period from the beginning of January 2020 to the end of December 2021. Type of study: Our study was retrospective. Data were collected from the department’s registers. Sampling: Strains were isolated from a variety of samples: urine, suppuration, genital swabs, puncture fluid and blood cultures. Study population: All patients of either sex and of any age who presented to the above laboratory for antibiotic susceptibility testing during this period. Inclusion criteria: All patients with a positive culture and antibiogram were included in our study. Exclusion criteria:
- All patients with negative culture or incomplete antibiogram.
- Duplicate strains isolated in the same patient from the same anatomical site.
- Incomplete or poor-quality samples.
Bacterial identification: Depending on their nature and site of infection, samples are inoculated onto culture media (CLED, EMB, blood agar, Chapman agar). Identification of bacterial strains was based on morphological, cultural and biochemical characteristics. For biochemical identification, bacterial strains were identified by VITEK® 2 (Biomerieux®) or API 20 E (Biomerieux)® Antibiogram: Antimicrobial susceptibility testing was performed using VITEK® 2 Compact or the agar diffusion technique, in accordance with the recommendations of the French Microbiology Society’s Committee on Antimicrobial Susceptibility Testing (CA-SFM) and the European Committee on Antimicrobial Susceptibility Testing (EUCAST) [4].
Results
Distribution of Germs by Species and Site of Infection
Gram-negative bacteria (GNB) accounted for 78.3% of isolates, while Gram-positive cocci (GPC) accounted for 21.7% of strains. GNB were mainly represented by enterobacteria (98.0%), and Escherichia coli was the most frequently isolated species (54.8%). The Gram-positive cocci were mainly Staphylococcus aureus (17.8%). The 511 strains isolated were distributed as follows: 387 from urine, 99 from suppurations, 18 from vaginal swabs, 5 from punctures and 2 from blood cultures: The distribution of species according to the pathological product is presented in Table I The distribution of germs by infectious site is shown in Table I.
| Urine | Suppuration | Vaginal Swabs | Puncture | BC | |
|---|---|---|---|---|---|
| Escherichia coli | 264 | 11 | 5 | 0 | 0 |
| Klebsiella pneumoniae | 62 | 7 | 2 | 0 | 0 |
| Proteus mirabilis | 7 | 4 | 0 | 0 | 0 |
| Serratia marcescens | 3 | 1 | 0 | 0 | 0 |
| Enterobacter cloacae | 20 | 2 | 0 | 0 | 1 |
| Citrobacter sp | 2 | 1 | 0 | 0 | 0 |
| Acinetobacter baumannii | 4 | 0 | 0 | 0 | 0 |
| Pseudomonas aeruginosa | 11 | 6 | 0 | 0 | 0 |
| Stenotrophomonas maltophilia | 1 | 0 | 0 | 0 | 0 |
| Staphylococcus aureus | 21 | 60 | 6 | 3 | 1 |
| Streptococcus spp | 1 | 7 | 4 | 2 | 0 |
| Enterococcus faecalis | 5 | 0 | 1 | 0 | 0 |
Table 1: Distribution of germs by infectious site.
Antibiotic Resistance in Bacteria
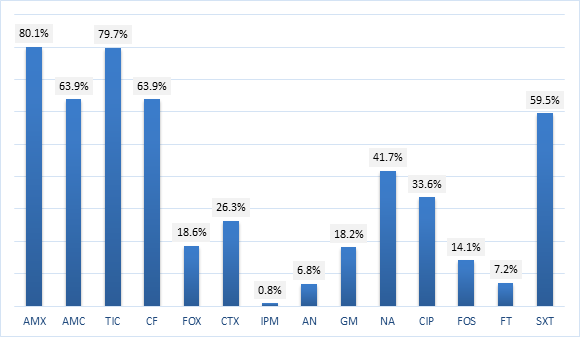
Escherichia coli: Antibiotic resistance rates in Escherichia coli strains: The rate of antibiotic resistance in Escherichia coli is shown in Figure 1.
Antibiotic Resistance Rates of Klebsiella Pneumoniae Strains
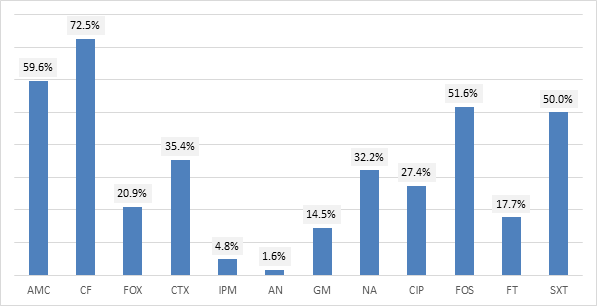
The rate of antibiotic resistance in Klebsiella pneumoniae is shown in Figure 2.
Other Germs
Resistance rates for Enterobacter cloacae, Proteus mirabilis, Serratia marcescens and Citrobacter sp are shown in Table 2.
| Enterobacter Cloacae | Proteus Mirabilis | Serratia Marcescens | Citrobacter | |
|---|---|---|---|---|
| Amoxicillin | (23/23) | (9/11) | (4/4) | (3/3) |
| Amx + ac clavulanique | (19/23) | (7/11) | (4/4) | (3/3) |
| Ticarcillin | (23/23) | (9/11) | (4/4) | (3/3) |
| Cephalotin | (23/23) | (8/11) | (4/4) | (2/3) |
| Cefoxitin | (18/23) | (2/11) | (2/4) | (3/3) |
| Cefotaxime | (13/23) | (3/11) | (2/4) | (1/3) |
| Imipenem | (2/23) | (0/11) | (1/4) | (0/3) |
| Amikacin | (4/23) | (0/11) | (0/4) | (0/3) |
| Gentamicin | (4/23) | (1/11) | (0/4) | (0/3) |
| Nalidixic acid | (7/23) | (6/11) | (2/4) | (1/3) |
| Ciprofloxacin | (4/23) | (4/11) | (2/4) | (1/3) |
| Cotrimoxazole | (12/23) | (6/11) | (2/4) | (1/3) |
| Fosfomycin | (14/23) | (4/11) | (1/4) | (2/3) |
| Nitrofurans | (11/23) | (4/11) | (1/4) | (2/3) |
Table 2: Antibiotic resistance rates of Enterobacter cloacae strains and Proteus mirabilis and Serratia marcescens and Citrobacte
BLSE-secreting Enterobacteria
Of 392 enterobacterales isolated, ESBL-secreting enterobacterales accounted for 14.5%. The percentage of ESBL strains within each enterobacterium is shown in Table 3.
| Germs | ESBL | Numbers | Percentage |
|---|---|---|---|
| Klebsiella pneumoniae | 17 | 71 | 23,9 % |
| Escherichia coli | 37 | 280 | 13,2 % |
| Proteus mirabilis | 1 | 11 | 9,1 % |
| Enterobacter cloacae | 2 | 23 | 8,7 % |
| Serratia marcescens | 0 | 4 | 0% |
| Citrobacter sp | 0 | 3 | 0% |
| Total | 57 | 392 | 14,5 % |
Table 3: The distribution of extended-spectrum beta-lactamase (ESBL)-producing strains among different enterobacterales.
Pseudomonas Aeruginosa, Acinetobacter Baumannii and Stenotrophomonas Maltophilia
Antibiotic resistance rates for strains of Pseudomonas aeruginosa, Acinetobacter baumannii and Stenotrophomonas maltophilia are shown in Table IV.
| Pseudomonas Aeruginosa | Acinetobacter Baumannii | Stenotrophomonas Maltophilia | |
|---|---|---|---|
| Ticarcillin | (12/17) | - | - |
| Pipiracillin/Tazobactam | (1/17) | (1/4) | (0/1) |
| Ceftazidime | (1/17) | (0/4) | (0/1) |
| Aztreonam | (1/17) | (0/4) | (0/1) |
| Imipenem | (0/17) | (0/4) | (0/1) |
| Amikacin | (0/17) | (0/4) | (0/1) |
| Gentamicin | (0/17) | (0/4) | (0/1) |
| Tobramycin | (1/17) | (0/4) | (0/1) |
| Ciprofloxacin | (5/17) | (0/4) | (0/1) |
| Colistin | (0/17) | (0/4) | (0/1) |
| Cotrimoxazole | (17/17) | (4/4) | (0/1) |
Table 4: Antibiotic resistance rates of Pseudomonas aeruginosa strains, Acinetobacter baumannii and Stenotrophomonas maltophili.
Staphylococcus Aureus
Resistance rate of Staphylococcus aureus strains
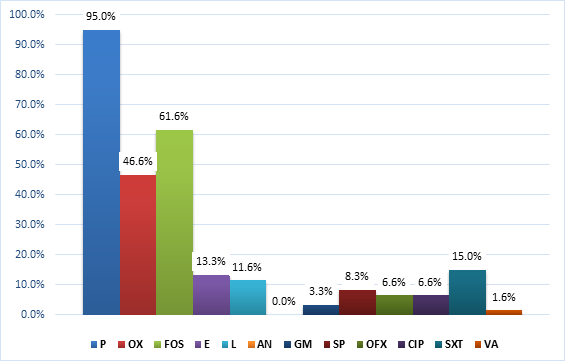
Staphylococcus aureus resistance rates are shown in Figure 3.
Streptococcus spp and Enterococcus faecalis Antibiotic resistance rates for Streptococcus spp and Enterococcus faecalis are shown in Table 5.
| Streptococcus spp | Enterococcus faecalis | |
|---|---|---|
| Ampicillin | (3/ 14) | (2/6) |
| Cefotaxime | (0/14) | - |
| Penicillin | (7/14) | (3/6) |
| Oxacillin | (1/14) | - |
| Erythromycin | (3/14) | (2/6) |
| Lincomycin | (0/14) | - |
| Pristinamycin | (0/14) | - |
| Spiramycin | - | (3/6) |
| Gentamicin | (12/14) | (2/6) |
| Ciprofloxacin | (5/14) | (2/6) |
| Fosfomycin | (1/14) | - |
| Vancomycin | (0/14) | (0/6) |
Table 5: Antibiotic resistance rates of Streptococcus spp and Enterococcus faecalis strains:
Discussion
In our study, Gram-negative bacteria (GNB) accounted for 78.3% (400/511) of isolates, while Gram-positive cocci (GPC) represented 21.7% (111/511) of strains. BGN were predominantly represented by Enterobacterales (98.0%, 392/400), while Escherichia coli was the most frequently isolated species (280, 54.8%). Gram-positive cocci were predominantly represented by Staphylococcus aureus (91/111), a result in line with that of Sekhokh, et al. [5]. The majority of strains came from urine (387 or 75.7%), followed by suppurations (99 or 19.4%). This result concurs with that of Ebongue, et al. [6].
Enterobacterales Resistance Profile
Of all the enterobacterales (strains) isolated, Escherichia coli was the most frequently isolated species (280/392) or 71.4%, followed by Klebsiella pneumoniae (71/392) or 18.1%. These results were comparable with those reported by Nadmia, et al. in Morocco, where Escherichia coli was the most frequently isolated species (80%), followed by Klebsiella (13%) [7], and with those reported by Nijssen, et al. in Europe, Escherichia coli (3325/5000) followed by Klebsiella pneumoniae (505/5000) [8]. Of the 392 enterobacterales identified, 57 (14.5%) were ESBL-producing strains. Our results were lower than those reported by Zahir, et al. (39%) in Morocco [9], and higher than those reported by Baizet, et al. (5.1%) in France [10]. In our study, the proportion of ESBL-producing strains of Klebsiella pneumoniae (17/71 or 23.9%) was higher than that of ESBL-producing strains of Escherichia coli (37/280 or 13.2%), a result in line with that of Baizet, et al. [10] and that reported by Guillard, et al. [11].
Resistance Profile of Escherichia coli Strains
Amoxicillin and clavulanic acid: Amoxicillin resistance for Escherichia coli was 80.1%. This result was comparable with the result of Hailaji, et al. 2014 in Nouakchott-Mauritania, 82.1% [12]. and 80% the studies of Zahir H, et al. in Morocco
2017 [9].
In the presence of clavulanic acid, resistance fell to 63.9%. Our study showed an increase in resistance compared with the study by Hailaji, et al. where resistance to AMC for Escherichia coli in 3 medical analysis laboratories in the city of Nouakchott, including CHN, in 20014 was 28.2% [12]. This increase in resistance was probably linked to the more frequent use of this antibiotic.
Cephalosporins: In our study, Escherichia coli resistance rates were 63.9%, 18.6% and 26.3% respectively for cefalotin, cefoxitin and cefotaxime. This rate was comparable with that reported by Hailaji, et al. for cefalotin and cefoxitin: 60.9% and 19.8% respectively, and lower than the 18.4% resistance rate for cefotaxime. The number of ESBL-producing strains in our study was 14.0% versus 10.4% in the Hailaji, et al. survey [12].
3rd-generation cephalosporins (C3G) remain active, and resistance is mainly due to ESBL production. However, in terms of antibiotic sparing, they are only indicated for probabilistic treatment of acute pyelonephritis [13].
Carbapenems: Escherichia coli were resistant to imipenem in 0.8% of cases, a result comparable with the 1.0% reported by Hailaji, et al. [12]. Our result was superior to that reported by Baizet, et al. France 2014, who found no imipenem- resistant strains [10].
Carbapenem-resistant enterobacteriaceae are a global concern in both hospital and community settings. Patients with carbapenem-resistant enterobacterial infections are three times more likely to die than patients with non- carbapenem-resistant enterobacterial infections [14] with an estimated mortality of 70% [15]. Rapid and accurate identification of carbapenem-resistant enterobacteriaceae is essential for infection prevention, as well as for guiding appropriate treatment. Once a patient has a confirmed carbapenem-resistant enterobacterial infection, additional precautions, including patient isolation, screening of other at-risk patients and monitoring of the spread of infection are warranted [16].
Aminoglycosides: In our study, the aminoglycosides remained active, mainly amikacin and to a lesser extent gentamicin, with resistance rates of 6.8% and 18.2% respectively. This result was superior to that of Hailaji, et al. 2014 in Nouakchott-Mauritania with a resistance rate of around 1% to amikacin and 13.5% to gentamicin [12]. and that of Smaoui, et al. in Tunisia, with a resistance rate of 1.1% to amikacin and 7.7% to gentamicin [17]. Our results were lower than those reported by Ebongue, et al. 27.5% for gentamicin and 14.1% for amikacin [6].
However, the activity of amikacin was better than that of gentamicin. This result is in line with the findings of some authors Hamouche, et al. [6, 18].
Quinolones: In our study, resistance to nalidixic acid was 41.7%. This result was comparable to the 40.6% reported in the 2014 study by Hailaji et al. in Nouakchott-Mauritania [12]. This rate is higher than 19.4% and 20.9% reported respectively by Garnotel, et al. in France [13]. and Smaoui, et al. in Tunisia [17]. Fluoroquinolones were more active: with a resistance rate of 33.6% for ciprofloxacin. This result was higher than that reported by Hailaji, et al. 28.6% [12], Smaoui, et al. 16.2% [17] and Guillard, et al. 15.9% [11]. Our rates remain low compared with those reported by Goro, et al. 65.92% [19]. Acquired resistance to quinolones is essentially linked to chromosomal mutations [20]. Resistance to fluoroquinolones is cross-linked between the different molecules, but its level of expression can vary for each molecule. Escherichia coli strains sensitive to nalidixic acid are also sensitive to other fluoroquinolones. On the other hand, resistance to nalidixic acid is frequently accompanied by reduced sensitivity to fluoroquinolones. This may correspond to low-level resistance mutants that can easily evolve to high-level resistance under the selection pressure exerted by this class of antibiotics. The appearance of resistance to nalidixic acid therefore appears to be a step in the evolution towards fluoroquinolone resistance, with a consequent risk of therapeutic failure [21].
Cotrimoxazole: Cotrimoxazole, a widely prescribed antibiotic, was resistant in 59.5%. This rate is comparable to 58.4% Hailaji, et al. in Mauritania in 2014 [12]. and lower compared to Fabre, et al. in France 19.3% [22]. The EAU (European Association of Urology) recommendations state that cystitis in men without prostate involvement is rare. Consequently, treatment with prostate-penetrating antimicrobials such as cotrimoxazole and fluoroquinolones is required in men with signs of UTI [23].
Nitrofurans, fosfomycin: In this context, molecules with urinary specificity are of particular interest. Indeed, they are effective: nitrofurans and fosfomycin (resistance 7.2% and 14.1% respectively for the two molecules). This rate was higher than that reported by Fabre, et al. in France (1.9% and 4.3% respectively [22]) and by Smaoui, et al. [17] in Tunisia (1% and 0% respectively. Our results differed from those reported by de Hailaji, et al. in 2014: nitrofurans were resistant in 7.2% versus 38.9% and fosfomycin in 14.1% versus 4.3% [12].
Nitrofurantoin, due to its limited use and highly specific mechanism of action (reduction of NO2 groups, leading to bacterial DNA damage), prevents cross-resistance. It retains good activity.
Fosfomycin also retains its activity for the same reasons. It is frequently prescribed because of its ease of use in single- dose form and good tolerance.
The characteristics of these antibiotics make them first-line probabilistic treatments for uncomplicated and gestational cystitis [23, 24].
Resistance profile of Klebsiella pneumoniae strains: In our study we observed an increase in Klebsiella pneumoniae resistance to amoxicillin-clavulanic acid 59.6% versus 35.1% in the survey by Hailaji, et al. in Nouakchott 2014 [12]. This rate was higher than the 23.6% reported by Smaoui, et al. in Tunisia [17].
Resistance to 3rd generation cephalosporins was 35.4% for cefotaxime, comparable with 37.9% in the study by Hailaji, et al. in Nouakchott 2014 [12] and with that of Hamouche, et al. in 2009 in France 32.3% [18] and higher than that of Smaoui, et al. in Tunisia 17.3% [17].
In our study ESBL-producing Klebsiella pneumoniae strains were 23.9% versus 20.4% isolated in 2014 [12].
In our study we noted imipenem resistance of 4.8% this result was higher than that reported by Hailaji, et al. in 2014 who reported no imipenem resistance in Klebsiella pneumoniae strains [12].
Aminoglycosides maintained good activity in our study, with the rate of resistance to amikacin and gentamicin reaching 1.6% and 14.5% respectively, a result comparable to that of Smaoui, et al. (3% and 16.2%) respectively [17]. Our result was lower than the rate reported by Hailaji, et al. in 2014 (19.5%) of gentamicin resistance [12].
In our study, the rate of quinolone resistance was lower than the results reported by Hailaji, et al. in 2014 in Nouakchott, with nalidixic acid resistance at 32.2% versus
48.0% in 2014 and ciprofloxacin resistance at 27.4% versus 33.6% in 2014 [12].
In our study, Klebsiella pneumoniae had a cotrimoxazole resistance rate of 50.0%. This rate was higher than the 44.6%, 40.0% and 40.1% reported respectively by Haylaji, et al. [12]. Hamouche, et al. in 2009 in France [18] and Smaoui, et al. Tunisia [17].
Resistance profile of Staphylococcus aureus strains: In our study, the penicillin G resistance rate was 95.0%, comparable to 97.2% reported by Salem, et al. [25] and higher than that found by Elhamzaoui, et al. in Morocco (86.8%) [26].
The rate of methicillin resistance in S. aureus was 46.6%, higher than that found in the study by Salem et al. 26.3% and Elhamzaoui, et al. in Morocco 19.3% [25, 26].
In our study, gentamicin resistance was found to be 3.3%, a lower rate than that reported by Salem, et al. in Nouakchott, Mauritania (6.85% [25]) and by Maiga, et al. in Mali (5.1% [27]).
In our study, cotrimoxazole was resistant in 15.0% of cases. this rate was lower than that noted by Salem, et al. with a resistance of 75% [25] and higher than that reported by Maiga, et al. 8,5% [27].
Resistance to fluoroquinolones was 6.6%, which is high compared with Salem, et al. in Nouakchott [25].
In our study, resistance to erythromycin and lincomycin was 13.3% and 11.6% respectively, higher than that reported by Maiga, et al. [27].
The diminished sensitivity of Staphylococcus aureus to glycopeptides is a current problem. In our study, we found 1.6% resistance to vancomycin. Our results differ from those reported by Salem, et al. in Mauritania, Nouakchott [25], and Elhamzaoui, et al. in Morocco [26], where all strains were sensitive to vancomycin.
It should be noted that this resistance of staphylococci to glycopeptides needs to be confirmed in staphylococci reference centers.
Conclusion
Antibiotic resistance is one of the most serious threats to global health today. It is at the root of prolonged hospitalization, increased medical expenses and higher mortality. This study of the state of bacterial resistance to antibiotics has highlighted certain epidemiological features.
During the study period, Gram-negative bacteria accounted for 78.3% of isolates, Gram-positive cocci for 21.7%. BGN were mainly represented by Enterobacterales (98.0%). Escherichia coli was the most frequently isolated species, accounting for 54.8%. CGPs were mainly represented by Staphylococcus aureus 82%. The majority of strains came from urine (75.7%), followed by suppurations (19.4%). Of the 392 enterobacteria identified, 14.5% were ESBL- producing strains. For Escherichia coli strains, the highest rate of resistance was to amoxicillin, ticarcillin and amoxicillin clavulanic acid. Imipenem was the most active molecule. For Klebsiella pneumoniae strains, cefalotin was the least active molecule, followed by amoxicillin clavulanic acid. For Staphylococcus aureus strains, penicillin was the least active antibiotic. Amikacin was active on all strains isolated.
Recommendations
In the light of our study and its comparison with the literature, we recommend literature, we recommend:
To the Authorities Support research into antibiotic resistance, and improve surveillance systems for infections caused by resistant bacteria.
Health care personnel Apply rules to prevent the transmission of infectious diseases, particularly in hospitals; improve antibiotic consumption (reduction and rational use).
To the public Avoid self-medication.
Authors’ Declarations and Contributions
Human and Animal Rights The authors declare that the work described in the article was carried out in accordance with ethical principles, in accordance with current recommendations.
Funding
This work has not received any grant from public, commercial or non-profit organizations.
Authors’ Contribution
Mohamed Ahmed Mohamed Mahamoud Sidya and Mohamed Lemine Salem, design, production and writing.
Declaration of Interests
The authors declare that they have no conflicts of interest.
All authors have read and approved the final version of the article.
References
-
Walsh C (2003) Antibiotics: actions, origins, resistance. American Society for Microbiology.
-
Waglechner N, Wright GD (2017) Antibiotic resistance: it’s bad, but why isn’t it worse? BMC Biology 15: 1-8.
-
Carlet J (2016) Wake up, antibiotic resistance is becoming a dramatic public health problem. Journal Des Anti-Infectieux 18: 37-39.
-
CASFM / EUCAST APRIL 2021 V1.0. Société Française de Microbiologie 2021.
-
Sekhsokh Y, Chadli M, El Hamzaoui SA (2008) Frequency and antibiotic susceptibility of bacteria isolated from urine. Médecine et Maladies Infectieuses 38: 324-327.
-
Ebongue CO, Tsiazok MD, Mefo’o JPN, Ngaba GP, Beyiha G, et al. (2015) Evolution of antibiotic resistance in enterobacterales isolated at Douala General Hospital from 2005 to 2012. The Pan African Medical Journal 20.
-
Nadmi H, Elotmani F, Talmi M, Zerouali K, Perrier-Gros- Claude JD, et al. (2010) Antibiotic resistance profile of community uropathogenic enterobacterales in El Jadida (Morocco). Médecine et Maladies Infectieuses 5: 303- 305.
-
Nijssen S, Florijn A, Bonten MJM, Schmitz FJ, Verhoef J, et al. (2004) Beta-lactam susceptibilities and prevalence of ESBL-producing isolates among more than 5000 European Enterobacteriaceae isolates. International Journal of Antimicrobial Agents 24: 585-591.
-
Zahir H, Draiss G, Rada N, Abourrahouat A, Sbihi M, et al. (2019) Microbial ecology and antibiotic susceptibility of bacteria isolated from urinary tract infections in children in Morocco. Revue Francophone Des Laboratoires pp: 65-70.
-
Baizet C, Ouar-Epelboin S, Walter G, Mosnier E, Moreau B, et al. (2019) Decreased antibiotic susceptibility of Enterobacteriaceae causing community-acquired urinary tract infections in French Amazonia. Medecine Et Maladies Infectieuses 49(1): 63-68.
-
Guillard F, Merens A, Dortet L, Janvier F, Lebrun C, et al. (2019) Evaluation of the prevalence of antibiotic resistance in enterobacterales isolated from urinary specimens in French emergency departments. Médecine et Maladies Infectieuses 49: S111-S112.
-
Hailaji NSM, Salem MO, Ghaber SM (2016) Antibiotic susceptibility of uropathogenic bacteria in the city of Nouakchott-Mauritania. Progrès En Urologie 26: 346-
-
Garnotel E, Astier H, Surcouf C, Bayette J, Bouige A, et al. (2017) Antibiotic susceptibility of _Escherichia_ _coli_ isolated from community urinary tract infections: study AFORCOPI-BIO, 2015. Revue Francophone Des Laboratoires 66-73.
-
Martin A, Fahrbach K, Zhao Q, Lodise T (2018) Association between carbapenem resistance and mortality among adult, hospitalized patients with serious infections due to Enterobacteriaceae: results of a systematic literature review and meta-analysis. Open forum infectious diseases, Oxford University Press, USA, Vol 5.
-
Friedman ND, Carmeli Y, Walton AL, Schwaber MJ (2017) Carbapenem-resistant Enterobacteriaceae: a strategic roadmap for infection control. Infection Control & Hospital Epidemiology 38: 580-594.
-
Larkin PM, Realegeno S, Ward KW, Garner OB, Yang S (2020) An unusual carbapenem-resistant _Escherichia_ _coli_ carrying plasmid-mediated AmpC and mutated ompC in a patient with recurrent urinary tract infections. IDCases 20: e00781.
-
Smaoui S, Abdelhedi K, Marouane C, Kammoun S, Messadi-Akrout F (2015) Antibiotic resistance of enterobacterales responsible for community urinary tract infections ŕ Sfax (Tunisia). Médecine et Maladies Infectieuses 8: 335-337.
-
Hamouche E, Sarkis DK (2012) Evolution of antibiotic susceptibility of _Escherichia coli_, Klebsiella pneumoniae, Pseudomonas aeruginosa and Acinetobacter baumanii in a Beirut University Hospital between 2005 and 2009. Pathology Biology 60: e15-20.
-
Goro AA (2021) Study of antibiotic resistance in enterobacterales isolated in Bamako from January 2020 to June 2020. Thesis, USTTB.
-
Chenia HY, Pillay B, Pillay D (2006) Analysis of the mechanisms of fluoroquinolone resistance in urinary tract pathogens. J Antimicrob Chemother 58: 1274-1278.
-
Diagnosis and antibiotic therapy of community-acquired bacterial urinary tract infections in adults. Medicine and Infectious Diseases 38: S203-S252.
-
Fabre R, Mérens A, Lefebvre F, Epifanoff G, Cerutti F, et al. (2010) Antibiotic susceptibility of _Escherichia_ _coli_ isolated from community-acquired urinary tract infections. Médecine et Maladies Infectieuses 40: 555- 559.
-
Bruyere F, Goux L, Bey E, Cariou G, Cattoir V, et al. (2020) Adult urinary tract infections: comparison of French and European recommendations. Infectious Diseases Committee of the French Urology Association (CIAFU), Progrès en Urologie 30: 472-481.
-
Doublet JD (2015) About the updated recommendations for the diagnosis and antibiotic therapy of adult bacterial urinary tract infections. Progrès en Urologie–FMC 25: F99-105.
-
Salem MLO, Ghaber SM, Baba SEWO, Maouloud MMO (2016) Antibiotic susceptibility of community destaphylococcus aureus strains in the Nouakchott region (Mauritania). The Pan African Medical Journal 24.
-
Elhamzaoui S, Benouda A, Allali F, Abouqual R, Elouennass M (2009) Antibiotic susceptibility of Staphylococcus aureus strains isolated from two teaching hospitals in Rabat, Morocco. Médecine et Maladies Infectieuses 39: 891-895.
-
Maiga II, Rochereau A, Douyon AA, Coulibaly S (2000) Sensibilite de Staphylococcus aureus aux antibiotiques a l’hopital du Point G a Bamako (Mali). Medecine et Maladies Infectieuses 10: 666-668.
- Antifungal Activity of New Acetophenone Derivatives
- Interconnected Microbiomes Human Health Within an Environmental Framework
- Silkworm-Based Vaccine Production for H5N1: A One Health Approach to Pandemic Preparedness
- Microbial Diversity and Lipolytic Activity of Bacteria and Fungi from Oil-Contaminated Sites in Makurdi Metroplois
- Epidemiology and Sensitivity to Antibiotics of Germs Isolated from Blood Cultures in the Laboratory of the National Hospital Center of Nouakchott-Mauritania
- Immobilization of Trametes Versicolor Laccase onto Silica Aerogel via Covalent Attachment Method