Post Marketing Surveillance of Antihypertensive Medicines in Tanzania
Background: Globally, cardiovascular diseases (CDVs) are amongst of the life threatening non- communicable diseases. The World Health Organization (WHO) reports indicate that CDVs is number one cause of deaths worldwide, largely in developing countries. Hypertension is a major risk factor for CVDs accounting for 9.4 million deaths worldwide every year. The prevalence of hypertension amongst Tanzanian is reported to be as high as 17%. Early detection and appropriate management of hypertension with quality and effective medicines is of clinical importance. The growing market of substandard and/or falsified medicines is a threat as it can result in treatment failure and unnecessary increase of healthcare cost. Objective: The surveillance was done by Tanzania Food and Drugs Authority with the aim of monitoring the quality of anti-hypertensive medicines circulating on the Tanzania mainland market. Methodology: Selected antihypertensive medicines were sampled from Medical Store Department, private and public healthcare facilities and pharmaceutical outlets from eleven (11) selected regions. All samples were subjected to product information review. All nifedipine samples were subjected to tier I quality screening test using the Global Pharma Health Fund® Mini-Lab kits. All samples which were not screened and about 10% of those passed the screening test were subjected to tier II confirmatory testing at Tanzania Food and Drugs Authority –WHO prequalified laboratory. Results: A total of 170 samples of antihypertensive were collected of which 63.5% (108/170) failed to comply with product information requirements. All 69 samples of nifedipine subjected to tier I screening test, passed disintegration and identification test by thin layer chromatography. A total of 90 samples were subjected to tier II confirmatory test ofwhich included (7) nifedipine, (32) atenolol, (27) captopril and (24) furosemide, all passed identification, disintegration, weight variation and appearance tests. Also all samples of atenolol, captopril and furosemide passed assay test. However, of the tested samples of nifedipine, 45.4% (5/11) failed assay test by having low contents of active ingredients with results ranged between 69.4% and 79.5% (Limit 90-110%). All batches of failed nifidipine tables were recalled from the market. Conclusion: Majority of the surveyed antihypertensive medicines were found to meet quality standards. However, the observed failure in assay of some nifedipine samples from a single manufacturer is a sign of availability of substandard medicines on the market and thus, calls for further vigilance of this product on the market.
Introduction
Globally, there is evidence of the growing burden of non communicable diseases (NCDs) such as cardiovascular diseases (CDVs), cancer, diabetes and chronic respiratory diseases especially in developing countries such as Tanzania [1]. The NCDs are reported to account for 60% of global death, largely in developing countries. In Tanzania, NCDs accounts for an approximate 31% of all total deaths [2]. Worldwide cardiovascular diseases (CDVs) are amongst of the life threatening NCDs [3]. The growing burden of death due to CDVs is decreasing in developed countries and drastically increasing in developing countries including Tanzania [3, 4]. According to the World Health Organisation (WHO), number one causes of deaths worldwide are CDVs. It is estimated that each year about 17.7 million people die from CDVs accounting to 31% of all global deaths, with more than 75% occurring in developing countries [1, 3]. In Tanzania CDVs are the second leading causes of death amongst patients with NCDs, accounting to 9% of total deaths. Unfortunately, majority of these deaths are prematurely and could have been prevented.
Hypertension is reported to be a major risk factor for CVDs, and currently is of increase in developing countries. Worldwide, about one billion people are reported to have uncontrolled hypertension [5]. It accounts for 9.4 million deaths worldwide every year. The prevalence of hypertension in African countries is reported to be as high as 46%, in adults aged 25 years and above. It is also responsible for at least 45 and 51% of death due to heart disease and stroke, respectively. In Tanzania, prevalence of hypertension ranges between 16 to 17% and it is high in urban and than in rural areas [6]. Healthy lifestyle is a main way of preventing hypertension. Avoiding complications of hypertension, early detection and appropriate management with quality and effective medicines is very crucial [5, 7]. However, accessibility to quality medicines especially in African countries is still a problem, as much as the growing market of substandard and/or falsified medicines is more of a concern [8].
Availability of substandard medicines on the market of various African countries has been largely reported [9, 10, 11, 12]. However, majority of these reports were on medicines against infectious diseases [13, 14, 15, 16, 17]. So far, there is no much being done to monitor the quality of antihypertensive medicines circulating on the market worldwide. A previous study conducted in Rwanda to assess the quality of antihypertensive medicines, revealed substandard antihypertensive drugs at a rate of 20% at the time of purchase [18]. Equally, in this study the potency of majority of antihypertensive was deteriorating with time due to tropical climatic condition. Report from a recent study on the quality of antihypertensive drugs from ten (10) sub-Saharan African countries revealed that nearly one-quarter of the available generic antihypertensive drugs were of poor quality [19].
The use of substandard antihypertensive medicines is of more risk to patients as it can contribute to disease complications, premature death and increase of healthcare cost unnecessarily. Therefore, systematic and continuous quality monitoring of antihypertensive medicines circulating on the market is vital to the national medicines regulatory authorities. This survey was aimed to assess the quality of selected antihypertensive generic medicines namely atenolol, captopril, nifedipine, and furosemide, circulating on the Tanzania market.
Methodology
Study design
This was a cross sectional prospective study.
Sampling
Four (4) generic antihypertensive namely captopril tablets (25mg), furosemide tablets (40mg), atenolol tablets (50mg) and nifedipine tablets (50mg) were involved in the survey. Selection criteria for the antihypertensive drugs included medicines of low cost which majority of population can afford and those available in almost all medicines distribution levels. Selected medicines were sampled from 11 out of 26 regions of Tanzania mainland namely; Dar es Salaam, Dodoma, Geita, Katavi, Kilimanjaro, Lindi, Mara, Mbeya, Mtwara, Mwanza and Ruvuma. The regions were selected based on the pre-defined criteria including highly populated regions, regions bordering other countries, regions with advanced urbanization, regions reported to have medicines quality problems and those which were not included in the previous post market surveillance (PMS) programmes.
Both systematic and purposive sampling techniques were used to obtain the sampling sites at regions and district levels down the medicines distribution channel. Samples were collected from Medical Store Department (MSD), public and private hospitals, dispensaries, heath centres, wholesale and retail pharmacies. The focus was on both foreign and locally manufactured products.
Samples were collected by trained drug inspectors according to the prepared sampling plan and internal standard operation procedures (SOP). Only two (2) brands per surveyed medicines type, available at the sampling site were collected in their original containers and their details filled in the sample collection tool. Each collected sample was coded according to the prescribed coding format. Coded samples with their respective sample collection tool were kept in the labelled sampling envelope and sealed. Storage and handling of samples during collection, transportation and before analysis adhered to manufacturer’s instruction and TFDA internal sample chain of custody procedures.
Quality Evaluation
Product Information Review: All samples were subjected to product information review (PIR) which involved visual examination of primary and secondary pack, package information leaflets (PIL) and product appearance, against the approved product information by TFDA. The information reviewed were product brand and generic name, dosage form and strength, name and address of the manufacturer, batch or lot number, TFDA registration number, manufacturing and expiration dates, storage condition, PIL and language. Observations were recorded in PIR results forms. Tier 1 Laboratory Screening: All samples of nifedipine were subjected to preliminary quality screening, of which disintegration test and identification by Thin Layer Chromatography (TLC) were performed using Global Pharma Health Fund® (GPHF) Mini-Lab kits. Nonetheless, samples of atenolol, captopril and furosemide were not screened due to absence of their method in the GHPF mini-lab kits. Visual Inspection: The physical appearance of all the dosage forms collected samples were examined for discolouration, odour and presence or absence of powder at the bottom of the secondary container. Simple Disintegration Test: Simple disintegration test: It was used to test the possibility of solid dosage form to break into small particles and thus, can dissolve and undergo dissolution to release active pharmaceutical ingredient. This was done using a 100 ml wide neck glass bottle filled with water heated to 37ºC. The tablets were shaken occasionally for about 30 minutes. The product was considered as failed the test if did not disintegrate within 30 minutes, after repeating the test three times consecutively. Identification by TLC: TLC method was used for product identification and qualitative determination of active ingredients, related substances and impurities present in the dosage forms. This method employed the principle of comparing spots obtained between test and reference solution according GHPF mini-lab kits manuals. The principal spot obtained with the test solution was required to correspond with the chromatographic runs of the standard solutions in terms of colour, shape, size, intensity and retardation factor (Rf) value for the sample to pass the test. The test sample was considered failed if the % error of Rf values of the test sample was more than ten percentage (10%) from that of the standard. The failure sample was taken for confirmatory tests.
Confirmatory Test: All samples which were not screened, failed and suspicious one and ten percent (10%) of samples that passed screening were subjected to confirmatory test as per pharmacopeia procedures (Table 1) at the TFDA-WHO prequalified laboratory. Parameters that were tested included: - appearance, identification, disintegration, related substance (where applicable), weight variation and assay. Table 1 below outlined the analytical methods employed for each product.
- S/N
- Product name and dosage form
- Method
- 1
- Captopril tablet
- BP 2013
- 2
- Furosemide tablets
- BP 2013 & IP 5th edition
- 3
- Atenolol tablets
- BP 2015
- 4
- Nifedipine tablets
- USP 38NF 33
Table 1: Analytical methods.
Data Management and Analysis
The obtained data from PIR, tier I screening test and tier II confirmatory test were checked for any inconsistencies, processed and analyzed using on Microsoft office, Excel spreadsheet (version 2010). Results of PIR, screening and confirmatory testing were expressed in percentage.
Majority of the samples 52.4% (90/170) were collected from pharmacies followed by hospitals 31.2% (53/170) and few samples 2.9 % (5/170) were from dispensaries, these results are summarized in Table 2 below.
Results
Samples Collected
A total of (72%) 170 out of the targeted 236 samples were collected from public and private healthcare facilities, retail and wholesale pharmacies and Medical Store Department (MSD) as shown in Table 2. Just as, two brands of each identified type of anti-hypertensive available in the selected premises were collected. Of the collected samples from the medicine distribution outlets, more samples 27% (46/170) were collected from Dar es Salaam and the least 1.8% (3/170) from Katavi region. Out of collected samples, nifedipine tablets were collected in large quantity 41% (69/170) compared to others as depicted in Figure 1 below:
Atenolol
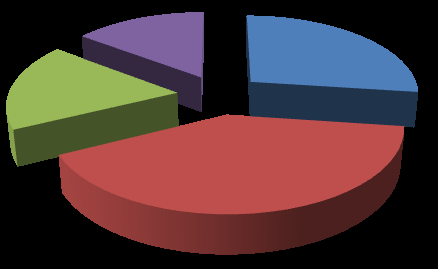
15%
27% Nifedipine
18% Captopril
Furosemide
40% Figure1: Percentage of samples collected per product.
| Medicine Distribution Levels | |||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| S/N | Product name | Health | |||||||||||||||||||||
| MSD | Pharmacy | Hospitals | Dispensary | Total | |||||||||||||||||||
| Centre | |||||||||||||||||||||||
| 1 | Atenolol | 3 | 31 | 9 | 2 | 1 | 46 | ||||||||||||||||
| 2 | Nifedipine | 2 | 44 | 16 | 3 | 4 | 69 | ||||||||||||||||
| 3 | Captopril | 4 | 9 | 15 | 2 | 0 | 30 | ||||||||||||||||
| 4 | Furosemide | 2 | 6 | 13 | 4 | 0 | 25 | ||||||||||||||||
| Total | 11 | 90 | 53 | 11 | 5 | 170 |
Table 2: Samples collected at different medicine distribution level.
Of the collected samples, majority 98.8% (168/170) were imported, amongst of the imported samples, majority were of nifedipine and atenolol 68.5% (115/168). Additionally, of the imported samples 63.1% (106/168) were from India, followed by 23.2% (39/168) from Cyprus and least were from Germany 4.2 % (7/168). These results have been summarized in the Table 3 below.
| Foreign manufacturer | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Type of product | Sample collected | Domestically manufacture | d | Imported | ||||||||||
| (country of origin) | ||||||||||||||
| Atenolol | 46 | 2(4.3%) | 35 (76.1%) | India | ||||||||||
| 4 (8.7%) | Germany | |||||||||||||
| 3 (6.5%) | Cyprus | |||||||||||||
| 2 (4.4%) | Kenya | |||||||||||||
| Nifedipine | 69 | 0 | 55 (79.7%) | India | ||||||||||
| 13 (18.8%) | Cyprus | |||||||||||||
| 1 (1.4%) | Germany | |||||||||||||
| Captopril | 30 | 0 | 22 (73.3%) | Cyprus | ||||||||||
| 6 (20%) | India | |||||||||||||
| 2 (6.7%) | Germany | |||||||||||||
| Furosemide | 25 | 0 | 14 (56%) | Kenya | ||||||||||
| 10 (40%) | India | |||||||||||||
| 1 (4%) | Cyprus | |||||||||||||
| Total | 170 | 2(1.2%) | 168(98.8%) |
Table 3: Collected samples and their country of origin of manufacturer.
Quality Evaluation
Product information review: All collected samples were subjected to product information review, a total of 63.5% (108/170) samples failed to comply with product information requirements. The highest failure rate was contributed by atenolol 29% (31/108) and the lowest by furosemide 19% (21/108) as depicted in Figure 2. A summary of failure of collected samples to comply with the product information requirements within product is signified in Figure 3.
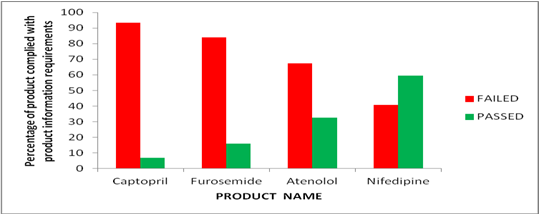
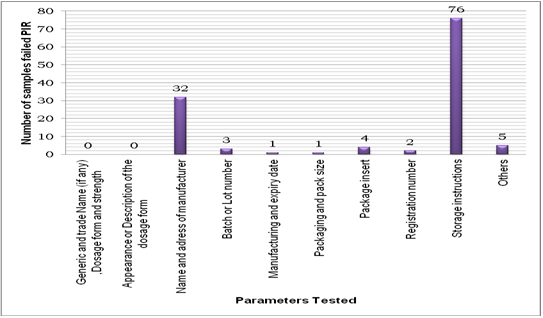
Similarly, all samples reviewed complied with the requirements of generic and brand name, strength and dosage form of the product as exemplified in the Figure 4 below. Failure to comply with storage condition requirements was the leading deficiency observed, attributing to 61.3% (76/124), followed by those which lack name and physical address of manufacturers 25.8% (32/124). TFDA registration numbers were not indicated on labels of majority of the collected samples even though, all were found to be registered in Tanzania. The major contributor of the former deficiency was atenolol 40.8% (31/76) followed by nifedipine 34.2% (26/76), and least was furosemide 11.8% (9/76) and the later was mainly contributed by captopril 81.3% (26/32). The trends are comparable to a recent survey study done on antimalarial drugs [20].
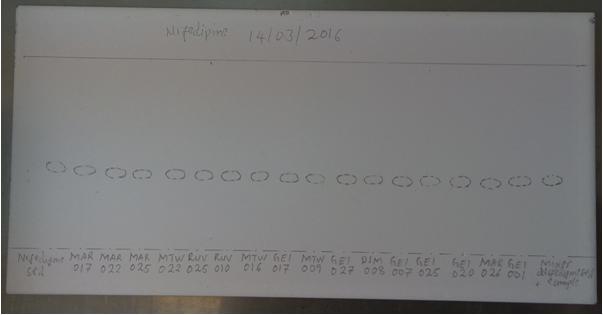
Laboratory Tier I screening test: All collected samples were subjected to visual inspection and all samples passed this test. All 69 samples of nifedipine subjected to tier I screening test, passed disintegration and identification test by TLC. Figure 5 below shows a developed TLC plate obtained from selected samples of nifedipine tablets.
confirmatory test, representing 83.3% (90/108) of the eligible number of samples as summarized in Table 4 below.
| Confirmatory testing | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Samples | S | amples Screened and | |||||||||||||||
| P | roduct nam | e | Criteria for | Actual samples selected | |||||||||||||
| collected | passed | Samples eligible | |||||||||||||||
| selection | and tested | ||||||||||||||||
| Nifedipine | 69 | 69 | 10% of samples passed screening | 7 | 7 | ||||||||||||
| Atenolol | 46 | Not screened | All samples not screened | 46 | 32* | ||||||||||||
| Captopril | 30 | Not screened | 30 | 27** | |||||||||||||
| Furosemide | 25 | Not screened | 25 | 24*** | |||||||||||||
| Total | 170 | 69 | 108 | 90 |
Table 4: Number of Samples Selected and Tested for Confirmatory Testing. * Selection based on assessment of the trend observed in
Table 4: Number of Samples Selected and Tested for Confirmatory Testing. * Selection based on assessment of the trend observed in the first 23 samples Three samples expired * One sample expired Samples of nifedipine, atenolol, captopril and furosemide were tested for appearance, identification, content uniformity by weight variation, disintegration, and assay. Moreover, captopril had additional test for related substance due to the availability of its reference standard for related substances. All samples of atenolol, captopril and furosemide passed all tested parameters, except nifedipine which failed assay test by 14.3% (1/7). This necessitated more samples from the same manufacture to be taken for confirmatory testing as described in the BP; thus, four (4) samples were tested. Again, all the additional samples of nifedipine tablets failed the assay test with results ranging between 69.4% and 79.5% (limit 90% -110%).
Discussion
The quality of medicines available in market especially in developing countries has been of a concern [21]. The prevalence of poor quality medicines jeopardizes patient safety, as it leads to treatment failure, development of drug resistance, disease complications, premature death and increase of healthcare cost to an individual and government at large [21, 22]. In this study, about 170 samples of antihypertensive medicines namely furosemide, captopril, nifedipine and atenolol were subjected to post market surveillance.
This study revealed that majority of samples were imported and specifically from India. These results are consistent with registration statistics of medicines in Tanzania where by 47% of registered medicines comes from India [23]. Among the surveyed medicines only atenolol was manufactured in Tanzania which signifies dependence of the country on medicines from abroad [24].
Results of this surveillance also revealed that availability of selected medicines especially in the targeted medicine distribution channels within the country was a challenge as shown in the results section. This was due to low stock and/or stock out of certain medicines in some regions and distribution levels along the medicines distribution channels. The study which was conducted in 2011 on availability of medicines and medical supplies has also revealed this challenge [25].
Despite, of similar sampling sites in each region, more samples 27.1% (46/170) were collected from Dar es Salaam region compared to others. This is because the region is the centre of business and as a consequence existence of many pharmaceutical outlets [26]. The least number of samples 1.8% (3/170) were collected from Katavi region because of relatively less urbanization in the respective region.
Majority of samples 52.9% (90/170) were collected from pharmacies followed by hospitals 31.2% (53/170), suggesting that various pharmaceutical products are more available in private health facilities as compared to public health facilities. These findings are in line with previous studies which have indicated that private pharmacies play a significant role in the health systems of many resource-limited countries [27, 28, 29].
The survey also has revealed an overall high failure rate (63.5%) to comply with product information requirements. The failure rate in this survey was also consistent with results of product information reviewed for other categories of medicines in the implementation of PMS programs [20, 30, 31]. The highest failure rate was contributed by inappropriate storage conditions contrary to the labelling requirements for medicinal products. Similar findings were observed in other previous studies conducted in Tanzania and India [32, 33, 34]. Majority of samples which failed were labelled store below 25°C’ which is not easy to achieve considering that Tanzania falls under ICH Zone IVb climatic condition [35]. The consequences, of failing to comply with storage condition information can be significant, such as loss of drug potency during improper storage that may impact the efficacy and safety of pharmaceuticals products and ultimately with the patient life [34]. Moreover, due to the increasing trend in non-communicable diseases especially cardiovascular diseases in developing countries, enforcement of proper product information is a key for proper prescribing, dispensing, storage and use of these products and eventually, quality of life of patients [36].
All tested samples of nifedipine disintegrated within the time limit of 30 minutes suggesting that the tablets are more likely to dissolve within the required time in vivo. The correlation between disintegration, dissolution rate and in vivo absorption has been proven [37]. Accordingly, all collected samples of nifedipine which were subjected to identification test passed it.
All tested samples of selected antihypertensive met the pharmacopeia requirement for appearance, identification, disintegration, content uniformity and assay. Failure in assay observed in one (1) batch of nifedipine was further confirmed by an additional of 4 samples of different batches from the same manufacturer, where consistent results were obtained. The failure in assay could be a result of degradation of the active ingredient attributed by light sensitivity nature of the active ingredient and less light protection capacity of the primary container [38]. The effect of tropical condition on the degradation of active ingredients of antihypertensive drugs has been also reported in a study conducted in Rwanda. Equally, these results are in accord with a recent study conducted in ten [10] developing countries, whereas, about one-quarter of the antihypertensive medicines circulating in the market were found to be of poor quality [19]. The assay failure could also be attributed by fault in manufacturing process of the product [39]. Fault in manufacturing process have been reported in others studies such as those conducted in Rwanda and American [40].
Conclusion
Presence of some substandard antihypertensive medicines circulating on Tanzanian market as revealed in this survey signifies the need for continuous monitoring of the quality of medicines post registration as an additional quality assurance measures. Markedly, the observed failure in assay of nifedipine from a single manufacturer calls for further vigilance of this product on the market.
References
-
WHO (2017) World Health Organization Non communicable Diseases Progress Monitor.
-
WHO (2014) Non Communicable Disease Country Profile.
-
WHO (2011) Global atlas on cardiovascular disease prevention and control Policies, strategies and interventions.
-
Mayige M, Kagaruki G, Ramaiy K, Swai A (2011) Non Communicable Diseases in Tanzania: a call for urgent action. Tanzania Journal Health Research 13(5): 378- 386.
-
WHO (2013) A global brief on Hypertension, silent Killer, Global Public Health Crisis.
-
Kavishe B, Biraro S, Baisley K, Vanobberghen F, Kapiga S, et al. (2015) High Prevalence of hypertension and of risk factors for non- communicable diseases (NCDs): a population based cross sectional survey of NCDS and HIV infection in Northwest Tanzania and Southern Uganda. BMC Med 13: 126.
-
WHO (2013) 2008-2013 Action plan for the Global Strategy for the Prevention and Control of Non communicable Diseases.
-
Africa Europe Faith and Justics Network (AEFJN), Quality medicines for all in Africa: Medicine fact sheet.
-
Ahmed Abdo-Rabbo, Amal Bassili and Hoda Atta (2005) The quality of anti-malarials available in Yemen. Malaria Journal 4: 28.
-
Hajjou M, Krech L, Lane-Barlow C, Roth L, Pribluda VS, et al. (2015) Monitoring of Quality of medicines – results from Africa, Asia and South America. Am J Trop Med Hyg 92(6): 68-74.
-
Almuzaini T, Choonara I, Sammons H (2013) Substandard and counterfeit medicines: a systematic review of the literature. BMJ Open 3(8).
-
Chikowe I, Osei-Safo D, Harrison J, Konadu D, Ivan Addae-Mensah I (2015) Post-marketing surveillance of anti-malarial medicines used in Malawi. Malaria Journal 14: 127.
-
Osei-Safo D, Agbonon A, Konadu DY, Harrison JJ, Edoh M, et al. (2014) Evaluation of the Quality of Artemisinin-Based Anti-malarial Medicines Distributed in Ghana and Togo. Malar Res Treat 2014: 806416.
-
John P Renschler, Kelsey M Walters, Paul N Newton, Ramanan Laxminarayan (2015) Estimated Under- Five Deaths Associated with Poor-Quality Anti- malarials in Sub-Saharan Africa. Am J Trop Med Hyg 92(6): 119-126.
-
Lalani M, Kaur H, Mohammed N, Mailk N, Wyk AV, et al. (2015) Substandard Anti-malarials Available in Afghanistan: A Case for Assessing the Quality of Drugs in Resource Poor Settings. Am J Trop Med Hyg 92(6): 51-58.
-
Jande M, Ngassapa O, Kibwage I (2000) Quality of sulfadoxine/ pyrimethamine tablets marketed in Dar es Salaam, Tanzania. East Cent Afr J Pharm Sci 3: 20- 24.
-
Minzi OM, Moshi MJ, Hipolite D, Massele AY, Tomson G, et al. (2003) Evaluation of the quality of amodiaquine and sulphadoxine/pyrimethamine tablets sold by private wholesale pharmacies in Dar Es Salaam, Tanzania. J Clin Pharm Ther 28(2): 117- 122.
-
Twagirumukiza M, Cosijns A, Pringels E, Remon JP, Vervaet C, et al. (2009) Influence of tropical climate conditions on the quality of antihypertensive drugs from Rwandan pharmacies. Am J Trop Med Hyg 81(5): 776-781.
-
Macquart de Terline D, Diop BI, Bernard M, Do B, Ikama MS, et al. (2018) Substandard drugs among five common antihypertensive generic medications: an analysis from 10 African countries. J Hypertens 36(2): 395-401.
-
Mziray S, Mwamwitwa K, Kisoma S, Augustine S, Fimbo A, et al. (2017) Post Marketing Surveillance of Anti-malarial Medicines in Tanzania. Pharm Regul Aff 6(191): 2.
-
Lon CT, Tsuyuoka R, Phanouvong S, Nivanna N, Socheat D, et al. (2006) Counterfeit and substandard antimalarial medicines in Cambodia. Trans R Soc Trop Med Hyg 100(11): 1019-1024.
-
Newton PN, Green MD, Fernández FM, Day NP, White NJ (2006) Counterfeit anti-infective drugs. Lancet Infect Dis 6(9): 602-613.
-
(2017) Tanzania Food and Drugs Authority Intergrated Management Information System - Registration Data Base.
-
Mcginnis MA (2013) Media Reports on Medicine Quality: Focusing on USAID-assisted Countries by the Promoting the Quality of Medicines program.
-
Sikika (2011) Medicines and medical supplies availability report using absorbent gauze availability survey as an entry point; a case of 71 districts and 30 health facilities across mainland Tanzania.
-
WHO (2002) Baseline Survey of the Pharmaceutical Sector in Tanzania.
-
Battersby A, Goodman C, Abondo C, Mandike R (2003) Improving the supply, distribution and use of antimalarial drugs by the private sector in Tanzania. Malaria Consortium.
-
Miller R, Goodman C (2018) Performance of retail pharmacies in low- and middle-income Asian settings : A systematic review. Health Policy Plan 31(7): 940-953.
-
Beyeler N, Liu J, Sieverding M (2015) A Systematic Review of the Role of Proprietary and Patent Medicine Vendors in Healthcare Provision in Nigeria. PLoS One 10(1).
-
TFDA (2016) Post Marketing Surveillance Report of the Quality of Selected Medicines under phase III- IX of 2011-2013 PMS Program. Tanzania Food and Drugs Authority, Dar-es-Salaam, Tanzania.
-
TFDA (2016) Post Marketing Surveillance Report of the Quality of Antimalarial, Anti-Retroviral and Anti- Tuberculous Medicines Circulating in Tanzania for the year 2012-2015. Tanzania Food and Drugs Authority, Dar-es-Salaam, Tanzania.
-
Shafaat K, Hussain A, Kumar B, ul Hasan R, Prabhat P, et al. (2013) An overview: storage of pharmaceutical products. World journal of pharmacy and pharmaceutical sciences 2: 2499-2515.
-
Kaale E, Manyanga V, Chambuso M, Liana J, Rutta E, et al. (2016) The Quality of Selected Essential Medicines Sold in Accredited Drug Dispensing Outlets and Pharmacies in Tanzania. PLoS ONE.; 11(11).
-
Ansari FA (2017) Study of various storage conditions on the pharmaceutical products and its implementation at retail store. The Pharma Innovation Journal 6(9): 475-478.
-
Climatic Zones for Stability Studies.
-
NHS, East Cheshire (2017) Dispensing and Storage of Medicines Policy.
-
Marton S, Szentmiklósi P, Rácz I (1984) Correlation between disintegration, dissolution and in vivo absorption rate in the case of compounds with benzyl-isoquinoline structures and its pharmacokinetic aspects. Pol J Pharmacol Pharm 36(4): 385-395.
-
Dinarvand R, Kouchakzadeh Z, Moghadam SH, Atyabi F (2006) Effect of Microencapsulation on Photo- Stability of Nifedipine. IJPR 5(4): 239-244.
-
Causes of Falsified and Substandard Drugs.
-
Johnston A, Holt DW (2014) Substandard drugs: a potential crisis for public health. Br J Clin Pharmacol 78(2): 218-243.
- Hydrogen Peroxide Scavenging by Methanolic Extracts of Coriander: An In Vitro Antioxidant Study
- Aromatherapy in Palliative Care: A Fragrant Quest for Relief
- Empowering Women, Securing Futures: Contraception’s Role in Socioeconomic Progress in India
- Effect of Crospovidone, Croscaramellose Sodium in Combination on the Drug Release of Anti diabetic Medication in Tablet Form
- Knowledge, Attitudes, Anxiety, and Preventive Behaviors Regarding Covid-19 Affliction among Healthcare Workers in Pakistan
- “Competitive Landscape and Brand Equivalents: Implications for ANDA (Abbreviated New Drug Application) Approval”