Early Onset of Pediatric Autoimmune Pancreatitis at the US-Mexican Border
Autoimmune pancreatitis (AIP) is an uncommon cause of pancreatitis that favorably responds to steroid therapy. Its true epidemiology remains unclear because only few cases of pediatric AIP have been reported. According to the adult criteria, AIP can be classified into 2 types: Type 1 or AIP without granulocyte epithelial lesions (GELs), and type 2 or AIP with GEL. Weexperienced two cases of pediatric AIP with unusually early age onset compared to previously reported data. With limited exceptions, our reported cases have a similar presentation, laboratory findings, radiographic findings, and positive response to steroid therapy compared to the previously reported cases. The main difference consisted in an early onset of disease (3-4 years of age) compared to the average age of onset of 11.9 years. A review of the current available reports demonstrated that more than 70 % of the cases of pediatric AIP could not be conclusively classified into the two types of AIP, raising the concern for a possibility of different pathophysiology between pediatric and adult AIP and the need for a pediatric-specific diagnostic criteria and treatment guideline for AIP.
Introduction
Pancreatic disease in children is uncommon but comprises of diverse etiologies and carries significant morbidity and mortality [1]. Although it is rare, acute pancreatitis is the most common pediatric pancreatic disease and recent literatures have shown an increasing incidence in children [1, 2, 3, 4, 5]. Autoimmune pancreatitis (AIP) in the pediatric population is thought to be an uncommon cause of acute and chronic pancreatitis but the true epidemiology remains unclear and more cases have been recently recognized [6, 7, 8, 9]. AIP can be classified into 2 types: Type 1 or AIP without granulocyte epithelial lesions (GELs), and type 2 or AIP with GEL. Type 1 is more commonly seen in elderly males with clinical presentation of obstructive jaundice, extra pancreatic involvement, and elevated serum immunoglobulin (Ig)G4. Pancreatic histopathology typically shows periductal dense infiltration of plasma cells and lymphocytes; storiform fibrosis; venulitis with lymphocytes and plasma cells frequently causing destruction of the affected vein; and profound IgG4 positive plasma cells (> 10 cells per high- power field [HPF]) [10]. Type 2 is more common in younger patients with equal sex distribution [10, 11]. Unlike type 1, patients do not have elevated serum IgG4 or other organ involvement (OOI), and they are more prone to present with abdominal pain, and have lower tendency to present with obstructive jaundice [10, 12]. Type 1 and 2 can often be distinguished by serum IgG4 level, OOI, and histology. Both types have similar radiologic pancreatic imaging findings. Computed tomography (CT) or magnetic resonance imaging (MRI) is a commonly used method for pancreatic imaging. Diffusely enlarged pancreas (especially with a capsule- like rim) without pancreatic ductal dilatation or pancreatic low density mass is highly suggestive of AIP [10]. In comparison to adults, there have been no reported cases of AIP definitive type 1 in children and radiological findings seem to be less intense [6]. Early recognition of the disease is important since the few reports in the literature available for pediatric AIP shows a drastic response to steroid therapy, which leads to avoiding unnecessary invasive procedures in children [6, 7, 8, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25]. Although there is a favorable response to steroids, some reported cases describe other autoimmune diseases later in life, particularly inflammatory bowel disease in AIP type 2 [6, 17, 25]. Up to our best knowledge, there are no defined guidelines for diagnosis and treatment of AIP in children. We will describe a small case series of early onset pediatric AIP and its comparison to the other reported cases in the literature.
Case 1
A previously healthy 4 year-old Hispanic male, presented with a four-day history of worsening severe epigastric pain and persistent emesis after being hit in the stomach by his friend. Past medical history and family histories were insignificant. Blood tests showed amylase 102 IU/L (normal range 25 – 115 IU/L), lipase 1208 IU/L (normal range 36 – 285 IU/L), and total bilirubin 0.5 mg/dL. Abdominal ultrasound (US) revealed a normal gallbladder, biliary tree, and pancreas. Magnetic resonance cholangiopancreatography (MRCP) showed peripancreatic, perihepatic and pericolic fluid, normal bile duct, and partially visualized pancreatic duct; the pancreatic duct in the region of the head was not visualized. The patient was treated with conservative management and was started on a low-fat diet after resolution of the abdominal pain, which the patient tolerated well. Since the pancreatic duct was not fully visualized, a repeat MRCP was scheduled 1 month later but the patient was lost to follow up. Two years later, at the age of six, the patient re- presented with a four-day history of epigastric pain. He denied recent trauma and had been doing well during the interim. Blood tests showed amylase 88 IU/L, lipase 525 IU/L (normal range 36 – 285 IU/L), total bilirubin 0.4 mg/dL, HDL 37 mg/dL, triglyceride 89 mg/dL, cholesterol 148 mg/dL, normal liver function tests, ANA positive with titer of 1:160, and normal IgG4 level. Abdominal US revealed focal swelling of the head of the pancreas. MRCP showed mildly enlarged pancreas with mass-like effect at the pancreatic head causing partial obstruction of the distal common bile duct and pancreatic duct (Figure 1). An ultrasound guided percutaneous pancreatic core- biopsy showed benign inflammatory fibrosis with lymphoplasmacytic infiltration, frequent eosinophils, and parenchymal acinar destruction without any neoplastic process. Granulocytic epithelial lesions (GEL) causing duct disruption was not found and IgG4 stain was negative. The patient was started on daily oral Prednisone 20 mg. Resolution of the patient’s symptoms was noted in less than 48 hours and a diagnosis of AIP probable type 2 was confirmed. At 1 month follow up, the patient’s symptoms resolved and serum lipase normalized. A repeat abdominal ultrasound at that time showed resolution of the pancreatic inflammation and normalization of the pancreatic anatomy. Oral prednisone was continued for 6 months and then slowly tapered without reoccurrence of symptoms.
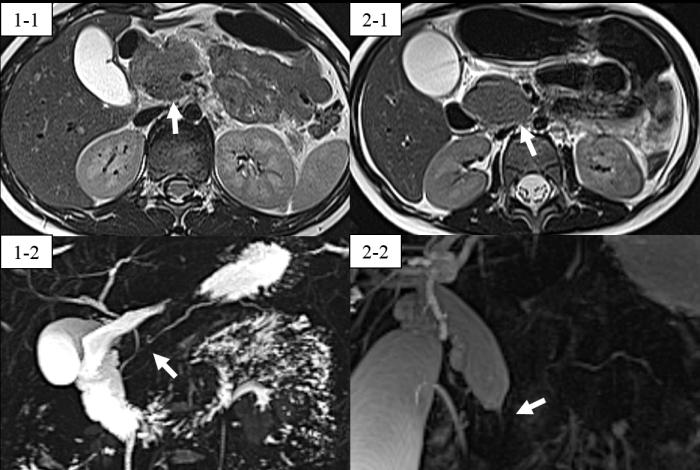
Figure 1: MRI results for case 1 and 2. 1-1 and 2-1 show a low T2 intensity mass-like effect at the pancreatic head (arrow). 1-2 shows partially obstructed pancreatic duct and distal common bile duct at the pancreatic head (arrows). 2-2 shows narrowing of the distal common bile duct at the level of the pancreatic head due to the mass- like effect (arrow).
Case 2
A previously healthy 3 year-old Hispanic female presented with a seven-day history of worsening epigastric pain, non-bloody non-bilious emesis, and mild scleralicterus. The family denied abdominal trauma, past medical history, and family history of gastrointestinal pathology. Blood tests showed lipase 30IU/L (normal range 36 – 285 IU/L), total bilirubin 7.0 mg/dL, direct bilirubin 4.9 mg/dL, AST 122IU/L, ALT 232IU/L, ALP 1118IU/L, GGT 978IU/L, ANA positive with a titer of 1:160, and IgG4 level was normal. Studies for CMV, EBV, and hepatitis A, B, and C were negative. Liver-kidney microsomal antibody and smooth muscle antibody were negative. Abdominal ultrasound showed diffuse swelling of the pancreas with markedly dilated common bile duct; mild central intrahepatic biliary ductal dilatation; no pancreatic ductal dilatation; and no evidence of stones and cholecystitis. MRCP showed enlarged pancreas with mass-like effect at the pancreatic head causing partial obstruction of the common bile duct and pancreatic duct (Figure 1). AIP type 2 was highly suspected but the family refused pancreatic biopsy. The patient was started on Methylprednisolone 20 mg IV, which was eventually changed to daily oral Prednisone 20 mg. After 48 hours of steroid therapy, there was remarkable improvement in the patient’s symptoms and laboratory markers and a diagnosis of AIP - not otherwise specified (NOS) was made. At 1 month follow up, the patient’s symptoms had completely resolved and laboratory markers normalized. Abdominal ultrasound repeated at that time showed normal pancreatic anatomy without inflammation. Prednisone was gradually tapered after 6 months of therapy without reoccurrence of abdominal pain or symptoms at 12 months follow up.
Discussion
Autoimmune pancreatitis (AIP) is a rare entity among children and there are no well-established guidelines for its diagnosis and length of therapy. There are two types of histological patterns to AIP defined by the International Consensus Diagnostic Criteria (ICDC): lymphoplasmacytic sclerosing pancreatitis (LPSP) or AIP without granulocyte epithelial lesions (GELs) and idiopathic duct-centric pancreatitis (IDCP) or AIP with GEL. The term AIP type 1 and type 2 are used for clinical profiles of LPSP and IDCP, respectively, because pancreatic histology often is not obtained. AIP type 1 is an IgG4-related disease characterized by elevated serum IgG4 levels, involves other organs with infiltration of IgG4-positive plasma cells, and is more common in elderly Asian males [10, 17, 19]. Type 2 is more common in the younger population with no gender preference, has a normal serum IgG4 level, and is commonly associated with inflammatory bowel disease, especially ulcerative colitis [10, 12, 15, 17, 19]. Because type 2 does not have serological markers, in order to make a definite diagnosis, histological confirmation of IDCP is necessary [10]. Clinically, patients with type 2 are more likely to present with abdominal pain and are less likely to present with obstructive jaundice [17]. Of all the cases that have been reported for children, none have had “AIP definitive type 1” (Table 1) [6]. The treatment for AIP is steroid administration and generally patients show good response to treatment.
presentation Serum Amylas
Symptoms at initial
Age (years
Serum
Patient numbe
Seru
m ANA
IgG4 (mg/dL)
Treatment
Patholog
y ICDC classificatio
Comorbid conditions Abdomin
CT/ERCP:
Diffusely
enlarged pancreas with
1 11 M + + + WNL /
ND ー WNL
stricture of lower bile duct and pancreatic duct.
# 6 CT: Mass-like enlargement of the pancreatic head with lower
2 14 F ND + ND WNL /
ND ー 190
bile duct stricture and caliber irregularity of the pancreatic duct.
CT: Pancreatic head mass and dilated common
3 10 M + + + WNL /
WNL ー WNL
bile duct CT: Pancreatic head mass with dilated common bile # 7
4 15 M ND + + WNL /
WNL ー WNL
duct and pancreatic duct CT - guided / Lymphoplasmacytic
Scarce + Definitive
AIP-2 Steroid therapy + ー None
infiltration with neutrophils infiltrating the lining epithelium of pancreatic ducts Endoscopic papillotomy and CT - guided / Lymphoplasmacytic infiltration, periductal and lobular ー + AIP therapy UC 1 year later No steroid neutrophilic infiltation biliary stent insertion.
PD / Ductocentriclymphoplasmacytic
31 cells/HP + AIP PD No steroid therapy None
inflammation and fibrosis F
Transduodenal laparoscopic TCB /
10 cells/HP ND Probable
AIP-1 Steroid therapy + ー Developed Celiac disease 1 year later Ductocentriclymphoplasmacytic inflammation and venulitis F
| 5 | 11 | F | + | ー | ND | High / High | ー | Elev ate d | US: Mildly prominent pancreatic head and body, and dilated pancreatic duct ERCP: Irregularity and beading of pancrea tic duct | EUS-FNA / Inconclusive | ND | ND | Probabl eAIP -1 | Observation initially but started steroids later for relapse. | + | + | None | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| # 8 | 6 | 14 | F | + | ND | ND | High / ND | ー | WNL | CT/MRCP: Pancreatic head enlargement. Dilated pancreatic duct with narrow distal portion. | Biospy not performed | AIP - NOS | Steroid therapy | + | + | |||
| # 9 | 7 | 11 | M | + | ー | ー | WNL / High | ー | WNL | MRCP: Focal swelling of the pancreatichead, delayed contrast enhancement, irregular pancreatic duct. | Laparotomy / Periductal fibrosis with lymphocytic and plasma cell infiltration. | ND | ND | AIP | ND | ND | ||
| #12 | 8 | 9 | F | + | ー | + | WNL / High | ー | WNL | CT / MRCP / EUS: Pancreatic head enlargement and pancreatic duct dilatation, beaded appearance. | EUS - FNA / Lymphocytic infiltration, marked fibr osis, and acinar atrophy | ー | ー | Probable AIP -2 | Initially treated with observation but relapsed. Steroid Therapy. | + | ー | |
| # 13 | 9 | 10 | M | + | ー | + | High/ WNL | ー | WNL | US / MRCP: Enlarged pancreas, multiple stenoses of the pancreatic duct, and dilatation o f biliary tract. | Not performed | AIP - NOS | Steroid therapy | + | ー | |||
| # 14 | 10 | 7 | M | + | ND | WNL / High | ND | WNL | CT / MRCP: Pancreatic head mass with irregular pancreatic duct. | CT - guided / Duct centric pancreatitis | ND | ND | AIP - NOS | Steroid therapy | + | ー | ||
| #15 | 11 | 16 | M | ー | + | + | WNL / WNL | ND | WNL | CT/MRI: Enlarged head of the pancreas and dilated biliary tract | Laparotomy / Periductal lymphoplasmocytic infiltration | ND | ND | AIP - NOS | Steroid therapy | + | ー | Diabete Mellitus |
| # 16 | 12 | 15 | F | + | ー | ND | ND / ND | ND | ND | Method ND:No pancreatic swelling. Main pancreatic duct stenosis. | Distal pancreatectomy / Idiopathic duct-c entric pancreatitis | ND | ND | Definitiv e AIP-2 | Distal pancreat ectomy . | No steroi d therapy | ||
| # 17 | 13 | 14 | M | + | ー | + | ND / WNL | + | Elevated | US : Bulky pancreatic he ad and body. MRCP: High T2 and low T1 signal surrounding the head and neck of the pancreas with common bile duct dilatation. | Laparotomy / ND | 90 cells /HPF in lymph node biopsy | ND | Probable AIP -1 | Steroid therapy | ND | ND | Developed UC 6 months later |
| 14 | 11 | M | + | ー | + | ND / High | + | Elevated | US / MRCP: Bulky pancreas. Biliary trac t dilatation. | ND / ND | 12 cells /HPF in liver biopsy | ND | Probable AIP -1 | Steroid therapy | + | + | Developed IBD a few weeks later. | |
| 15 | 7 | M | + | ー | ND | ND / High | ー | WNL | US / MRCP: Diffusely enlarged pancreas. | ND / ND | > 10 cells /HPF in liver biopsy | ND | Probabl e AIP-1 | Steroid therapy | ND | ND | Possible IBD | |
| # 18 | 16 | 10 | F | + | ー | ND | High / High | ー | WNL | MRCP: Diffusely enlarged pancreas and irregular main pancreatic duct. | Not performed | AIP - NOS | Steroid therapy | + | ー | |||
| # 19 | 17 | 13 | F | + | + | ND | WNL / WNL | ー | WNL | CT / EUS / ERCP: Multiple pancreatic masses, stricture at the distal common bile duct, and bilia ry dilatation. | EUS - FNA / Lymphocytic infla mmatory infiltrate | ND | ND | Probabl e AIP-1 | Initially treated with pancreatic stent insertion but relapsed and started stero id therapy. | + | + | Fibrosing mediastinitis 3 months later |
| # 20 | 18 | 8 | F | + | ND | + | WNL / WNL | ND | WNL | MRCP: Small volume pancreas and low-grade inflammation throughout. Collapsed pancreatic duct. | EUS - FNA / Insufficient tissue for analysis | ND | ND | AIP - NOS | Steroid therapy | + | ー | |
| # 21 | 19 | 15 | F | + | + | ー | ND / ND | ー | WNL | US / CT / EUS / MRCP: Pancreatic head mass with delayed contrast enhancement. Enlarged and irregular main pancrea tic duct. | EUS - FNA / Periductal lymphocytic infiltration a nd obliterative phlebitis. | > 10 cells /HPF in liver biopsy | ND | Probabl e AIP-1 | Steroid therapy | + | ー | |
| # 22 | 20 | 10 | M | ND | WNL | ND | ND / ND | ー | + | Definitiv e AIP-2 | Steroid therapy | + | ND | Chronic glomerulonephritis , Evan's syndrome | ||||
| # 23 | 21 | 12 | M | + | + | ND | WNL / ND | ー | WNL | MRCP: Enlarged pancreatic head with obstruction of the common bile and pancreatic duct. | US guided percutaneous pancreatic corebiopsy / Fibrous tissue with lymphocytic and plasma cell infiltration | ND | ND | AIP | Biliary stent placement with pancreatic enzyme supplementation | No steroi d therapy | ||
| # 24 | 22 | 10 | M | + | + | + | ND / ND | ND | WNL | CT / MRCP / EUS: Pancreatic head mass, dilatation of the distal pancreatic duct, and dilated common bile duct with a taper at the level of the pancreas. | PD / Lymphoplasmacytic infiltration without out e vidence of malignancy. | ND | ND | AIP | PD | No steroi d therapy | ||
| # 25 | 23 | 9 | ND | + | + | ND | ND / ND | ND | WNL | MRI / EUS: Diffusely enlarged pancreas with biliary stricture. | EUS - TCB / Features consi stent with AIP | ND | + | Definitiv e AIP-2 | Steroid therapy | + | ー | |
| 24 | 9 | ND | + | + | ND | ND / ND | ND | WNL | MRCP / EUS: Diffusely enlarged pancreas and irregular pancreatic duct | EUS - TCB / Features consi stent with AIP | ND | + | Definitiv e AIP-2 | Steroid therapy | + | ー | ||
| 25 | 14 | ND | ー | ー | ND | ND / ND | ND | 274 | CT / EUS: Diffusely enlarged pancreas and irregular pancreatic duct. | EUS - TCB / Features consi stent with AIP | ND | + | Definitiv e AIP-2 | Observation | No steroi d therapy | Crohn's disease | ||
| 26 | 16 | ND | ー | ー | ND | ND / ND | ND | WNL | MRI: Diffusely enlarged pancreas. EUS: Irregular main pancreat i c duct. | EUS - TCB / Features consi stent with AIP | ND | + | Definitiv e AIP-2 | Steroid therapy | + | ー | ||
| 27 | 17 | ND | ー | ー | ND | ND / ND | ND | WNL | CT / EUS / ERCP: Diffusely enlarged pancreas and irregular main pancreatic duct. | EUS - TCB / Features consi stent with AIP | ND | + | Definitiv e AIP-2 | Steroid therapy | + | ー | ||
| 28 | 17 | ND | ー | ー | ND | ND / ND | ND | WNL | EUS: Irregular main pancr eatic duct. | EUS - TCB / Likely AIP | ND | + | Definitiv e AIP-2 | Observation | No steroi d therapy | |||
| 29 | 18 | ND | ー | ー | ND | ND / ND | ND | WNL | EUS: characteristic features of AIP. | EUS- TCB / Nondiagno stic sample | ND | ND | Probable AIP -2 | Observation | No steroi d therapy | Crohn's disease | ||
| #26 | 30 | 14 | F | Details unknown | AIP | Details Unknown | ||||||||||||
| 31 | 17 | F | AIP | |||||||||||||||
| Case 1 | 32 | 6 | M | + | ー | ー | WNL / WNL | + | WNL | MRCP: Mildly enlarged pancreas with masslike effect at the pancreatic head causing partial obstruction of the distal common bile duct and pancreatic duct. | US guided percutaneous pancreatic corebiopsy / Benign inflammatory fibrosis with lymphoplasmacytic infiltration, frequent eosinophils, and parenchymal acinar destruction | ー | ー | Probable AIP -2 | Steroid therapy | + | ー |
- MRCP:
- Enlarged pancreas with mass-like effect at the pancreatic
- Case 2
- 33
- 3
- F
- +
- +
- ー
- NP /
- WNL
- +
- WNL
- NP
- AIP - NOS Steroid therapy
- +
- ー
- None head causing partial obstruction of the distal common bile duct and pancreatic duct.
- ANA: Antinuclear antibody, Elevated: More than 2 folds of upper limit of normal, ERCP: Endoscopic retrograde pancreatography, EUS: Endoscopic ultrasonography, FNA: Fine needle aspiration, High: More than 3 folds of normal upper limit, HPF: High power field, IBD: Inflammatory bowel disease, MRCP: Magnetic resonance cholangiopancreatography, ND: Not described, NP: Not performed, PD: Whipple pancreaticoduodenectomy, TCB: Trucut biopsy, UC: Ulcerative colitis, US: Ultrasound, WNL: Within normal limit (Including less than 3 folds of normal upper limit for serum amylase and lipase, and less than 2 folds of normal upper limit for IgG4).
Table 2: Brief description of presentation, diagnosis, and treatment of previous cases of AIP and two cases we
association with other autoimmune diseases (i.e. inflammatory bowel disease) to decrease the morbidity when followed as an outpatient. Also, approximately 70% of the cases reported could not be clearly classified as either type 1 or type 2, and treatment methods differed depending on the reported cases, raising the question that there may be a need to create a pediatric-specific diagnostic criteria and treatment guideline for AIP.
Reference
1. Jolley CD (2010) Pancreatic disease in children and adolescents. Curr Gastroenterol Rep 12(2): 106-113.
2. Lopez MJ (2002) The changing incidence of acute pancreatitis in children: a single-institution perspective. J Pediatr 140(5): 622-624.
3. Werlin SL, Kugathasan S, Frautschy BC (2003)
Pancreatitis in children. J Pediatr Gastroenterol Nutr 37(5): 591-595.
4. Mark A, Salvatore (2006) Acute Pancreatitis in the Pediatric Population: a large population-based study. J Pediatr Gastroenterol Nutr 43: E73.
5. Yadav D, Lowenfels AB (2006) Trends in the epidemiology of the first attack of acute pancreatitis: a systematic review. Pancreas 33(4): 323-330.
6. Zen Y, Grammatikopoulos T, Hadzic N (2014)
Autoimmune pancreatitis in children: insights into the diagnostic challenge. J Pediatr Gastroenterol Nutr 59(5): e42-45.
7. Friedlander J, Quiros JA, Morgan T, Zhang Z, Tian W,
et al. (2012) Diagnosis of autoimmune pancreatitis vs neoplasms in children with pancreatic mass and biliary obstruction. Clin Gastroenterol Hepatol 10(9): 1051-5.1.
8. Takase M, Imai T, Nozaki F (2010) Relapsing
autoimmune pancreatitis in a 14-year-old girl. J Nippon Med Sch 77(1): 29-34.
9. Refaat R, Harth M, Proschek P, Lindemayr S, Vogl TJ
(2009) Autoimmune pancreatitis in an 11-year-old boy. Pediatr Radiol 39(4): 389-392.
10. Shimosegawa T, Chari ST, Frulloni L, Kamisawa T,
Kawa S, et al. (2011) International consensus diagnostic criteria for autoimmune pancreatitis: guidelines of the International Association of Pancreatology. Pancreas 40(3): 352-358.
11. Maire F, Le Baleur Y, Rebours V, Vullierme MP,
Couvelard A, et al. (2011) Outcome of patients with type 1 or 2 autoimmune pancreatitis. Am J Gastroenterol 106(1): 151-156.
12. Patel Z, Patel S, Grendell J, Marciano T (2015) Type 2
autoimmune pancreatitis: case report of a 9-year-old female and a review of the literature. Clin J Gastroenterol 8(6): 421-425.
13. Gargouri L, Ponsot P, Viala J, Belarbi N, Martinez C, et al. (2009) Recurrent autoimmune pancreatitis in a 10-year-old boy. J Pediatr Gastroenterol Nutr 48(3): 374-377.
14. Long J, Birken G, Migicoysky B (2015) Autoimmune
pancreatitis in a child presenting as a pancreatic mass. J Pediat Surg Case R 3(3): 111-113.
15. Blejter J, Weller S, Pace R, Cusumano H, Giambini D
(2008) Autoimmune pancreatitis: an adolescent case and review of literature. J Pediatr Surg 43(7): 1368- 1372.
16. Notohara K, Burgart LJ, Yadav D, Chari S, Smyrk TC
(2003) Idiopathic chronic pancreatitis with periductal lymphoplasmacytic infiltration: clinicopathologic features of 35 cases. Am J Surg Pathol 27(8): 1119-1127.
17. Bolia R, Chong SY, Coleman L, MacGregor D, Hardikar
W, et al. (2016) Autoimmune Pancreatitis and IgG4 Related Disease in Three Children. ACG Case Rep J 3(4): e115.
18. Hasosah MY, Masawa L, Jan A, Alsaleem K (2016) A
Case Report of Childhood Recurrent Autoimmune Pancreatitis: A Rare Emerging Entity. J Clin Diagn Res 10(6) : 1-2.
19. Mannion M, Cron RQ (2011) Successful treatment of pediatric IgG4 related systemic disease with mycophenolate mofetil: case report and a review of the pediatric autoimmune pancreatitis literature. Pediatr Rheumatol Online J 9(1): 1.
20. Galloway DP, Wallihan D, Smith MT, Abu-El-Haija M
(2016) An Unusual Presentation of Pediatric Autoimmune Pancreatitis. Pancreas 45(2): 1-2.
21. Neuzillet C, Lepere C, El Hajjam M, Palazzo L, Fabre M,
et al. (2010) Autoimmune pancreatitis with atypical imaging findings that mimicked an endocrine tumor. World J Gastroenterol 16(23): 2954-2958.
22. Detlefsen S, Mohr Drewes A, Vyberg M, Kloppel G
(2009) Diagnosis of autoimmune pancreatitis by core needle biopsy: application of six microscopic criteria. Virchows Arch 454(5): 531-539.
23. El-Matary W, Casson D, Hodges S, Davison S, McClean,
P et al. (2006) Successful conservative management of idiopathic fibrosing pancreatitis in children. Eur J Pediatr 165(8): 560-565.
24. Bartholomew SV, Zigman A, Sheppard B (2006)
Lymphoplasmacytic sclerosing pancreatitis presenting as a pancreatic head mass in a child: case report and management recommendations. J Pediatr Surg 41(5): 23-25.
25. Fujii LL, Chari ST, El-Youssef M, Takahashi N,
Topazian MD et al. (2013) Pediatric pancreatic EUS- guided trucut biopsy for evaluation of autoimmune pancreatitis. Gastrointest Endosc 77(5): 824-828.
26. Zamboni G, Luttges J, Capelli P, Frulloni L, Cavallini G
et al. (2004) Histopathological features of diagnostic and clinical relevance in autoimmune pancreatitis: a study on 53 resection specimens and 9 biopsy specimens. Virchows Arch 445(6): 552-563.
References
-
Jolley CD (2010) Pancreatic disease in children and adolescents. Curr Gastroenterol Rep 12(2): 106-113.
-
Lopez MJ (2002) The changing incidence of acute pancreatitis in children: a single-institution perspective. J Pediatr 140(5): 622-624.
-
Werlin SL, Kugathasan S, Frautschy BC (2003) Pancreatitis in children. J Pediatr Gastroenterol Nutr 37(5): 591-595.
-
Mark A, Salvatore (2006) Acute Pancreatitis in the Pediatric Population: a large population-based study. J Pediatr Gastroenterol Nutr 43: E73.
-
Yadav D, Lowenfels AB (2006) Trends in the epidemiology of the first attack of acute pancreatitis: a systematic review. Pancreas 33(4): 323-330.
-
Zen Y, Grammatikopoulos T, Hadzic N (2014) Autoimmune pancreatitis in children: insights into the diagnostic challenge. J Pediatr Gastroenterol Nutr 59(5): e42-45.
-
Friedlander J, Quiros JA, Morgan T, Zhang Z, Tian W, et al. (2012) Diagnosis of autoimmune pancreatitis vs neoplasms in children with pancreatic mass and biliary obstruction. Clin Gastroenterol Hepatol 10(9): 1051-5.1.
-
Takase M, Imai T, Nozaki F (2010) Relapsing autoimmune pancreatitis in a 14-year-old girl. J Nippon Med Sch 77(1): 29-34.
-
Refaat R, Harth M, Proschek P, Lindemayr S, Vogl TJ (2009) Autoimmune pancreatitis in an 11-year-old boy. Pediatr Radiol 39(4): 389-392.
-
Shimosegawa T, Chari ST, Frulloni L, Kamisawa T, Kawa S, et al. (2011) International consensus diagnostic criteria for autoimmune pancreatitis: guidelines of the International Association of Pancreatology. Pancreas 40(3): 352-358.
-
Maire F, Le Baleur Y, Rebours V, Vullierme MP, Couvelard A, et al. (2011) Outcome of patients with type 1 or 2 autoimmune pancreatitis. Am J Gastroenterol 106(1): 151-156.
-
Patel Z, Patel S, Grendell J, Marciano T (2015) Type 2 autoimmune pancreatitis: case report of a 9-year-old female and a review of the literature. Clin J Gastroenterol 8(6): 421-425.
-
Gargouri L, Ponsot P, Viala J, Belarbi N, Martinez C, et al. (2009) Recurrent autoimmune pancreatitis in a 10-year-old boy. J Pediatr Gastroenterol Nutr 48(3): 374-377.
-
Long J, Birken G, Migicoysky B (2015) Autoimmune pancreatitis in a child presenting as a pancreatic mass. J Pediat Surg Case R 3(3): 111-113.
-
Blejter J, Weller S, Pace R, Cusumano H, Giambini D (2008) Autoimmune pancreatitis: an adolescent case and review of literature. J Pediatr Surg 43(7): 1368- 1372.
-
Notohara K, Burgart LJ, Yadav D, Chari S, Smyrk TC (2003) Idiopathic chronic pancreatitis with periductal lymphoplasmacytic infiltration: clinicopathologic features of 35 cases. Am J Surg Pathol 27(8): 1119-1127.
-
Bolia R, Chong SY, Coleman L, MacGregor D, Hardikar W, et al. (2016) Autoimmune Pancreatitis and IgG4 Related Disease in Three Children. ACG Case Rep J 3(4): e115.
-
Hasosah MY, Masawa L, Jan A, Alsaleem K (2016) A Case Report of Childhood Recurrent Autoimmune Pancreatitis: A Rare Emerging Entity. J Clin Diagn Res 10(6) : 1-2.
-
Mannion M, Cron RQ (2011) Successful treatment of pediatric IgG4 related systemic disease with mycophenolate mofetil: case report and a review of the pediatric autoimmune pancreatitis literature. Pediatr Rheumatol Online J 9(1): 1.
-
Galloway DP, Wallihan D, Smith MT, Abu-El-Haija M (2016) An Unusual Presentation of Pediatric Autoimmune Pancreatitis. Pancreas 45(2): 1-2.
-
Neuzillet C, Lepere C, El Hajjam M, Palazzo L, Fabre M, et al. (2010) Autoimmune pancreatitis with atypical imaging findings that mimicked an endocrine tumor. World J Gastroenterol 16(23): 2954-2958.
-
Detlefsen S, Mohr Drewes A, Vyberg M, Kloppel G (2009) Diagnosis of autoimmune pancreatitis by core needle biopsy: application of six microscopic criteria. Virchows Arch 454(5): 531-539.
-
El-Matary W, Casson D, Hodges S, Davison S, McClean, P et al. (2006) Successful conservative management of idiopathic fibrosing pancreatitis in children. Eur J Pediatr 165(8): 560-565.
-
Bartholomew SV, Zigman A, Sheppard B (2006) Lymphoplasmacytic sclerosing pancreatitis presenting as a pancreatic head mass in a child: case report and management recommendations. J Pediatr Surg 41(5): 23-25.
-
Fujii LL, Chari ST, El-Youssef M, Takahashi N, Topazian MD et al. (2013) Pediatric pancreatic EUS- guided trucut biopsy for evaluation of autoimmune pancreatitis. Gastrointest Endosc 77(5): 824-828.
-
Zamboni G, Luttges J, Capelli P, Frulloni L, Cavallini G et al. (2004) Histopathological features of diagnostic and clinical relevance in autoimmune pancreatitis: a study on 53 resection specimens and 9 biopsy specimens. Virchows Arch 445(6): 552-563.
- Understanding Pediatric Multiple Sclerosis: Clinical Presentation, Diagnostic Criteria, Therapeutic Advances, and Supportive Care Approaches
- Hemophilia in Children
- Xia-Gibbs Syndrome- A Case Report
- A Study to Assess Effectiveness of Play Therapy in Reducing Post-Operative Pain among Children Age 2 To 5 Year who have Undergone General Surgeries in Selected Pediatric Hospitals of Vadodara
- Preterm Birth: Scope of the Problem, Cost of Care, Potential Complications and Current Guidelines for Management
- Noradrenaline: Can we Use it to Manage Hemodynamic Instability among Neonatal Septic Shock at the NICU?