Serum IgD Levels in Allergic Children with Gastrointestinal Manifestations
A large number of studies investigating various biomarkers for allergy have been published over the past decades. To this date, no single or specific biomarker for allergy has been identified. Therefore, we examined markers of inflammation and immunoglobulins in children with allergic symptoms, among which children with GI allergy, in an attempt to find new and indicative markers for GI allergy. In the present study, total serum levels of immunoglobulin (Ig)D, CM-lgE, Ig-free light chain (Ig-fLC) kappa and lambda, thymic stromal lymphopoietin (TSLP), thymus and activation-regulated chemokine (TARC/CCL17) and galectin-9 were analyzed on 117 atopic infants and children, divided into different allergic manifestations: asthma (n=7), atopic dermatitis (n=56), eosinophilic esophagitis (n=20) and gastrointestinal (GI) allergy (n=34). Elevated levels of serum IgD, without the presence of IgE, was found in children with GI allergy. Serum IgD did not correlate with other laboratory parameters of atopy such as serum cow’s milk-lgE, Ig-fLC, TSLP, TARC and galectin-9. In conclusion, serum IgD is elevated in children with GI allergy, in the absence of IgE, and can be considered as a new indicative marker for GI allergy, however, its exact role in the pathogenesis of atopy awaits further studies.
Introduction
Immunoglobulins D (IgD) represent approximately 0.2% of human circulating immunoglobulins. Term neonates have significantly lower serum IgD concentrations than children above 1 year of age, indicating that levels of IgD are maturing during the first year of life [1]. While the function of IgM, IgG, IgA and IgE is relatively well known, the function of IgD has remained elusive so far. IgD is co-expressed with IgM on the surface of most mature B cells before antigenic stimulation and functions as a transmembrane antigen receptor. A non- canonical form of class switching from IgM to IgD occurs in the human upper respiratory mucosa to generate IgD- secreting B cells that bind respiratory bacteria and their products. In addition to enhancing mucosal immunity, IgD class-switched B cells enter the circulation to ‘arm’ basophils and other innate immune cells with secreted IgD. Although the nature of the IgD receptor is still unknown, cross-linking of IgD on basophils stimulates release of immunoactivating, proinflammatory and antimicrobial mediators and might therefore play a role in allergic diseases [2]. In a study by Peng et al., the means of both total serum IgE and IgD were significantly higher in atopic patients when compared to healthy controls, with no difference for serum IgD level with age, gender or asthmatic status. Total serum IgD was not significantly correlated with total serum IgE, indicating the absence of a link in the immunoregulatory control of the two isotypes [3]. In atopic infants and children, a significantly higher serum IgD level was seen in asthmatic children and in infants with atopic dermatitis (AD) as compared to a control group with no difference between asthma and AD or co-expressed atopic conditions, but values significantly higher in severe asthma and lower in mild asthma. Again, serum IgD did not show a correlation with serum lgE [4]. In another study, serum IgD and IgE levels were compared with the clinical status of children with atopic asthma and of a control group. At baseline, IgD levels were significantly higher in the atopic asthma group compared to the control group, and normalized during the next 18 months during asthma treatment [5]. Two very recent publications show a role for IgD in rhinosinusitis [6, 7] and suggest that IgD might contribute to enhance mucosal immunity, inflammation, or respond to bacterial infections. The purpose of the study was to take advantage of a well characterized cohort of children in a reference center for food allergy, already used for analyzing children with eosinophilic esophagitis (EoE) to evaluate the potential usefulness of measuring IgD in the different conditions related to food allergy [8].
Materials and Methods
Ethics Statement
This retrospective convenience cohort study was performed in children with EoE referred to the paediatric gastroenterology department of the Hospital Necker- Enfants malades and, before that, the Hospital Saint Vincent de Paul, Paris, France. The study moved hospitals when the researcher took up a new paediatric position. Participants were recruited from the ARSENE cohort, a collection of blood and biopsy samples registered within the French Ministry of Health (number DC-2009-955), and all data were anonymized, all according the World Medical Association Declaration of Helsinki regarding ethical conduct of research involving human subjects. According to French law, organisations keeping routinely collected paediatric material need to obtain a declaration from the French Ministry of Health and written, informed consent from all parents and all children aged 11 years and older. This means that no ethic committee approval was needed for this study.
Study Population
The study was carried out in a population of children consecutively followed up for food allergy in the paediatric gastroenterology department of the Hospital Saint Vincent de Paul, Paris, France from 17 June 2009 to 3 February 2010 and in the pediatric gastroenterology department of the Hospital Necker-Enfants malades, Paris, France, from 4 February 2010 to 1 September 2010. Samples were obtained as part of the routine procedure for assessing the nutritional status and delineating elimination diet. A written informed consent was obtained from all parents as well as from children of 11 years or older. Children were labelled according their clinical presentation; asthma (n=7), AD (n=56), EoE (n=20) and gastrointestinal (GI) allergy (n=34). Asthma was considered if patients had bronchospasm on spirometry, AD was considered according to criteria proposed by Hanifin and Rajka [9], EoE was considered in patients when upper endoscopy showed, according to updated international recommendations [10], mucosal eosinophilic infiltration ≥15 eosinophils/ HPF in at least 2 biopsy samples of the lower oesophagus. Gastric and duodenal biopsies were always taken to rule out eosinophilic gastroenteritis. Gastrointestinal allergy was diagnosed according recommendation of the 2010 Expert Panel Guidelines, including medical history and physical examination, elimination diets, skin prick test, specific IgE measurements, and oral food challenges [11]. For the diagnosis of cow’s milk allergy, the ESPGHAN GI committee practical guidelines were followed [12].
Measurement of Serum Immunoglobulins IgD and IgE
Total serum IgD levels were measured using the commercial Human IgD ELISA Quantitation Set (Bethyl Laboratories, USA) according to the manufacturer’s protocol. Atopic levels of total IgD is 20.3 μg/ml [3] and all levels above were considered elevated. Measurement of food specific IgE in serum was done using the Phadia CapRast® (Uppsala, Sweden). Specific IgE values ≥ 0.35 kU/L was considered elevated [13]. Cow’s milk (CM)-IgE could be measured in the majority of the allergic children as compared to other food specific-IgEs (egg, peanut, soy, wheat, tree nuts) and was therefore chosen as the representative of food-specific IgE.
Measurement of Serum Immunoglobulin Free Light Chain (Ig-fLC)
Total kappa and lambda Ig-fLC serum concentrations were determined using an ELISA adapted from Abe et al. [14]. In short, plates were coated o/n with goat-anti mouse IgG (4 μg/ml), blocked for 1 hour and subsequently incubated with mouse-anti human kappa or lambda Ig-fLC (1 μg/ml; Fκ-C8 or Fλ-G9; both obtained from Dr. A. Solomon, Tennessee, USA) for 1 hour. After incubation with different dilutions of serum samples and standards for 1 hour, plates were incubated with HRP- labelled goat F(ab’)2-anti human kappa or lambda Ig-fLC (1:20,000) for 1 hour. Finally, TMB substrate was added and the enzymatic reaction was stopped by adding 0.9 M H2SO4. Between incubation steps, wells were washed three times with PBS-T (0.1% tween-20). Per sample, at least three data points were used to calculate the concentration. Reference levels of Ig-fLC were obtained in a cohort of 250 children with different allergic manifestations, mean kappa Ig-fLC level was 13.8 µg/ml (SD 8.0) and mean lambda Ig-fLC level was 14.8 µg/ml (SD 7.0). Ig-fLC concentrations above average + SD (for both kappa and lambda Ig-fLC 21.8 µg/ml) were considered elevated.
Measurement of Serum Thymic Stromal Lymphopoietin (TSLP), Thymus and Activation- Regulated Chemokine (TARC/CCL17) and Galectin-9
The human TSLP ELISA Ready-SET-Go!® (eBiosciences) was performed according to the manufacturer’s protocol and any measured level of TSLP was considered elevated. TARC was measured using an in-house ELISA as previously described [8]. TARC levels were calculated based on the standard curve for each assay plate and compared to cut-off values described in children diagnosed with atopic dermatitis: 1431 pg/ml for birth to 1 year-of-age, 803 pg/ml for 2-5 years and 510 pg/ml for 6 years and over [15]. Galectin-9 was measured using an in-house ELISA as previously described [16] with some minor adjustments. In short, high-binding EIA/RIA 96-well plate (Costar) were coated with polyclonal anti-human galectin-9 antibodies (R&D Systems) in PBS overnight at 4°C. Plates were blocked 1 hour with PBS/1% BSA. Samples (serial dilution series starting 1:4) and standard curve (recombinant human galectin-9; 39 – 40,000 pg/ml) were added for 2 hours and then incubated 1 hour with biotinylated anti-human galectin-9 antibodies (R&D Systems) in PBS/1% BSA. Plates were incubated 1 hour with poly-HRP-streptavidin (Sanquin) followed by incubation with the substrate tetramethylbenzidine (TMB; Perbio Science). The reaction was stopped with 2 M H2SO4 and optical density (OD) was measured at 450 nm. Galectin-9 levels were calculated based on the standard curve for each assay plate. In order to obtain reference values for galectin-9, we analysed serum levels of galectin-9 of 250 children visiting the paediatric gastroenterology department with different allergic manifestations - skin, gastrointestinal, respiratory and EoE – and levels above average + SD (36.6 µg/ml) were considered elevated.
Statistical Analysis
All analyses were performed using the statistical software package SPSS 15.0. Normal distribution was tested using the Shapiro-Wilk test and variances using the Levene’s test. When the data were normally distributed and the variances were equal, a two-tailed two-sample t- test was used to compare groups. When the data were not normally distributed, a two-tailed Mann-Whitney test was used to compare groups and a Satterthwaite correction was done for differences in group size. Comparison of percentages was done by using a two-tailed Pearson Chi- Square test. Values of P less than 0.05 were considered significant.
Results
Serum Immunoglobulins IgD, CM-IgE and Ig-fLC
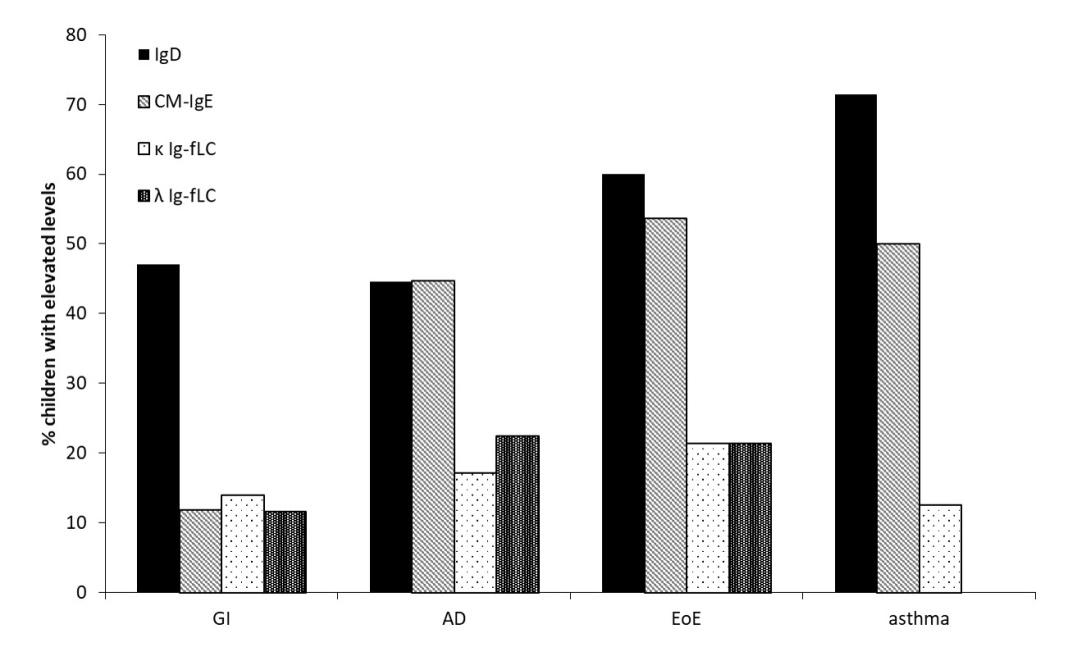
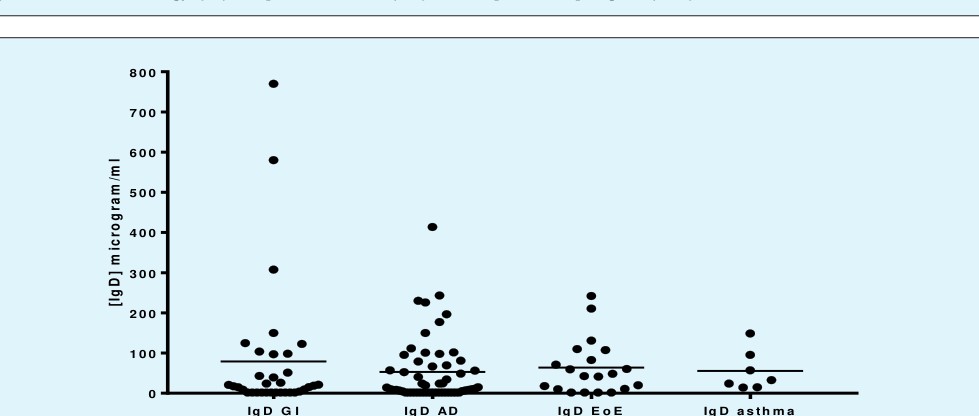
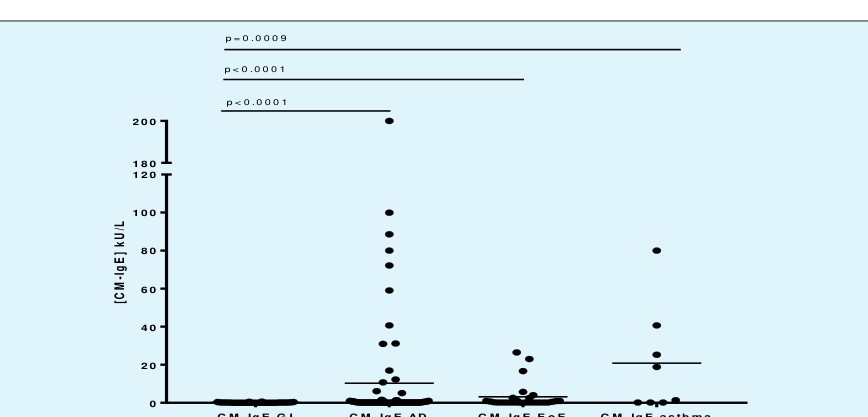
Our data showed that elevated levels of IgD were present during all allergic manifestation (Figure 1), mostly accompanied with similar elevated levels of CM- IgE, however in GI allergy only IgD seems to play a role. When comparing IgD and IgE levels per patient, there was no correlation between IgD and IgE (data not shown). Elevated levels of both kappa- and lambda Ig-fLC were not very common during allergic manifestations and absolute levels did not show differences between groups (data not shown). IgD absolute levels seemed to be the highest in GI allergy, followed by AD and EoE, and lowest levels were found in asthmatic children (Figure 2), although there were no statistical differences between the groups. CM- IgE absolute levels were high in AD and asthma, and moderate in EoE, however all groups were significantly different (both t-test and ANOVA) from GI allergy where virtually no IgE could be detected (Figure 3).
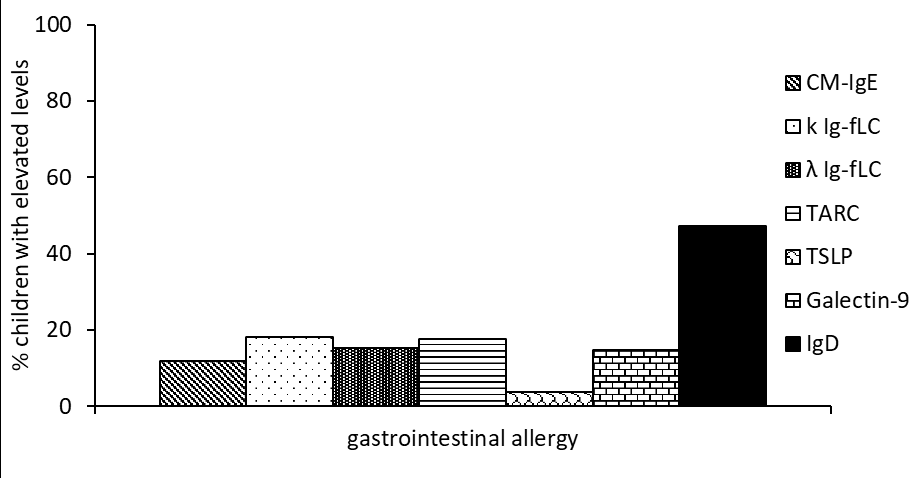
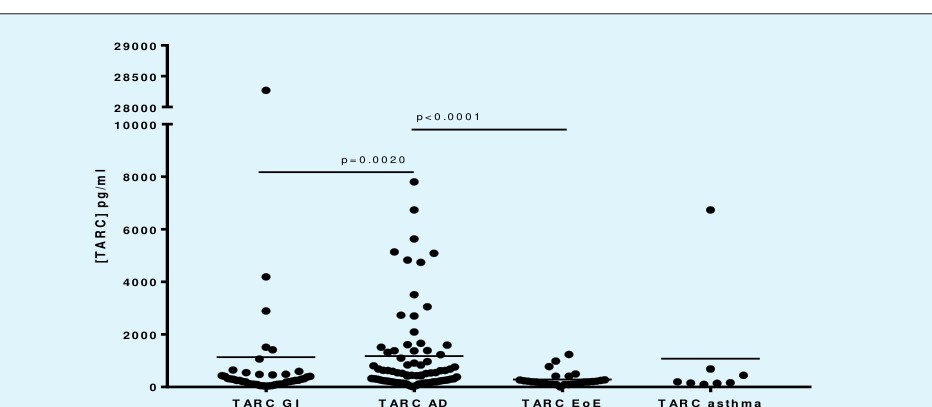
In the same cohort, also other markers were measured in an attempt to identify specific markers for food allergy, among which the cytokine TSLP [17, 18, 19], the chemokine TARC [20, 21] and the β-galactoside-binding protein galectin-9 [16, 22] for their known role in allergic diseases. Studying the elevated levels of these markers together with IgD, CM-IgE and Ig-fLCs in children with GI allergy, none of the markers seemed to play an important role in GI allergy, except for IgD which was elevated in 50% of the children suffering from GI allergy (Figure 4). Absolute levels of the markers showed no differences in the case of TSLP or galectin-9 (data not shown), and our data confirmed the known role of TARC in AD [15, 20, 21, 23, 24, 25, 26], with levels significantly higher in the AD group when compared to GI allergy, EoE and asthma groups (Figure 5).
Discussion
This study is the first to show that elevated serum IgD, in absence of IgE, might be considered in research for markers of GI allergy. The role of serum IgD in disease is still unclear. Increased serum IgD levels are found in patients with various types of immunodeficiency diseases, in severe recurrent infections of the respiratory tract, and in single patients with a variety of clinical syndromes or abnormalities [27]. Some studies showed IgD antibody specificity to nuclear antigens in patients with autoimmune disease [28], to insulin in diabetics and to benzylpenicilloyl epitope in some patients with penicillin allergy [29, 30]. During immune responses, human B cells go through an isotypic switch, influenced by different cytokines, from IgM-IgD to IgG1-4, IgA1-2 or IgE [31, 32]. While IgM is first expressed by pre-B cells, IgD emerges later during B cell ontogeny, being mostly expressed at the transitional and mature B cell stage. In humans, a small subset of B cells express IgD but not IgM. These IgM-IgD+ B cells are found in the circulation as well as in tonsils, nasal cavities, lachrymal glands and salivary glands, but are rarely detected in non-respiratory mucosal areas. The specific topography of IgM-IgD+ B cells may result from the expression of tissue homing receptors that do not favor colonization of extra-respiratory mucosal sites such as the intestine. In addition to enhancing mucosal immunity, IgD class-switched B cells enter the circulation to ‘arm’ basophils and other innate immune cells with secreted IgD. Although the nature of the IgD receptor remains elusive, cross-linking of IgD on basophils stimulates release of immune activating mediators such as interleukin (IL)-1β, IL4, IL-8, IL-13, tumor necrosis factor- α, interferon γ-induced protein 10, and B-cell activating factor [2]. Disorders involving the gastrointestinal tract constitute one of the main causes of pediatric consultations, and a subset of these disorders has been attributed to immunologic reactions to foods. In contrast to IgE- mediated reactions, non-IgE- mediated gastrointestinal food allergic disorders are characterized by subacute and/or chronic symptoms and are likely under-diagnosed. GI allergy occurs in a different epithelium (absorptive, columnar, as opposed to squamous in skin and esophagus), in a environment where food allergens have already been digested, as opposed to any other organ involved in allergy. This might explain that classical markers used for allergy are not expressed in GI allergy and therefore there is a need for discovery of other diagnostic markers [33]. The significance of elevated levels of IgD in allergic subjects remains elusive. Elevated IgD levels are mostly not correlated with elevated IgE, as we also observe in our GI allergy group. This indicates that immunoregulatory controls of the basal levels of the two isotypes are not linked. Thus, an increase in serum IgD is probably not a consequence of the presence of IgE but rather represent an additional qualitative difference in the immunological make-up of atopic patients. In children with atopic asthma IgD levels decreased with time, whilst IgE increased. In genetically predisposed patients, the increase in IgD during the initial process of allergic sensitization might represent a non-specific response or an attempt of the organism to block asthma, favoring therefore immunologic tolerance [34].
Conclusion
In conclusion, serum IgD is elevated in children with GI allergy in the absence of IgE, and does not show a correlation with other laboratory parameters of atopy such as serum cow’s milk-lgE, Ig-fLC, TSLP, TARC and galectin-9. Therefore, it might be considered as a new indicative marker for GI allergy; however, its exact role in the pathogenesis of atopy awaits further studies.
References
-
Josephs SH, Buckley RH (1980) Serum IgD concentrations in normal infants, children, and adults and in patients with elevated IgE. J Pediatr 96(3): 417-420.
-
Chen K, Cerutti A (2011) The function and regulation of immunoglobulin D. Curr Opin Immunol 23(3): 345- 352.
-
Peng Z, Fisher R, Adkinson NF Jr (1991) Total serum IgD is increased in atopic subjects. Allergy 46(6): 436- 444.
-
Gamal YE, Awad Z, Zaghloul M, Fouad A (1996) 411Total serum IgD in atopic infants and children. J Allergy Clin Immunol 97(1): 285.
-
Salpietro DC, Masaracchio A, Turiaco A, Di Bella MR, Toscano V, et al. (2001) Serum IgD levels in children with atopic asthma. A longitudinal study. Minerva Pediatr 53(1): 1-5.
-
Min JY, Nayak JV, Hulse KE, Stevens WW, Raju PA, et al. (2017) Evidence for altered levels of Immunoglobulin D in the nasal airway mucosa of patients with chronic rhinosinusitis. J Allergy Clin Immunol 140(6): 1562-1571.
-
Sokoya M, Ramakrishnan VR, Frank DN, Rahkola J, Getz A, et al. (2017) Expression of immunoglobulin D is increased in chronic rhinosinusitis. Ann Allergy Asthma Immunol 119(4): 317-323.
-
Knipping K, Colson D, Soulaines P, Redegeld F, Garssen J, et al. (2014) Serum immunoglobulin free light chain levels are higher in girls than boys during eosinophilic oesophagitis. Acta Paediatr 103(7): 766- 774.
-
Hanifin JM, Rajka G (1980) Diagnostic features of atopic dermatitis. Acta Derm Venereol (Stockh) 60(92): 44-47.
-
Liacouras CA, Furuta GT, Hirano I, Atkins D, Attwood SE, et al. (2011) Eosinophilic esophagitis: updated consensus recommendations for children and adults. J Allergy Clin Immunol 128(1): 3-20.
-
Sicherer SH, Sampson HA (2014) Food allergy: Epidemiology, pathogenesis, diagnosis, and treatment. J Allergy Clin Immunol 133(2): 291-307.
-
Koletzko S, Niggemann B, Arato A, Dias JA, Heuschkel R, et al. (2012) Diagnostic approach and management of cow's-milk protein allergy in infants and children: ESPGHAN GI Committee practical guidelines. J Pediatr Gastroenterol Nutr 55(2): 221-229.
-
Saarinen UM, Juntunen K, Kajosaari M, Björkstén F (1982) Serum immunoglobulin E in atopic and non- atopic children aged 6 months to 5 years. A follow-up study. Acta Paediatr Scand 71(3): 489-494.
-
Abe M, Goto T, Kosaka M, Wolfenbarger D, Weiss DT, et al. (1998) Differences in kappa to lambda (kappa:lambda) ratios of serum and urinary free light chains. Clin Exp Immunol 111(2): 457-462.
-
Fujisawa T, Nagao M, Hiraguchi Y, Katsumata H, Nishimori H, et al. (2009) Serum measurement of thymus and activation-regulated chemokine/CCL17 in children with atopic dermatitis: elevated normal levels in infancy and age-specific analysis in atopic dermatitis. Pediatr Allergy Immunol 20(7): 633-641.
-
de Kivit S, Saeland E, Kraneveld AD, van de Kant HJ, Schouten B, et al. (2012) Galectin-9 induced by dietary synbiotics is involved in suppression of allergic symptoms in mice and humans. Allergy 67(3): 343-352.
-
Lee EB, Kim KW, Hong JY, Jee HM, Sohn MH, et al. (2010) Increased serum thymic stromal lymphopoietin in children with atopic dermatitis. Pediatr Allergy Immunol 21(2): e457-e460.
-
Chauhan A, Singh M, Agarwal A, Paul N (2015) Correlation of TSLP, IL-33, and CD4 + CD25 + FOXP3 + T regulatory (Treg) in pediatric asthma. J Asthma 52(9): 868-872.
-
Shoda T, Matsuda A, Arai K, Shimizu H, Morita H, et al. (2016) Sera of patients with infantile eosinophilic gastroenteritis showed a specific increase in both thymic stromal lymphopoietin and IL-33 levels. J Allergy Clin Immunol 138(1): 299-303.
-
Furue M, Matsumoto T, Yamamoto T, Takeuchi S, Esaki H, et al. (2012) Correlation between serum thymus and activation-regulated chemokine levels and stratum corneum barrier function in healthy individuals and patients with mild atopic dermatitis. J Dermatol Sci 66(1): 60-63.
-
Hijnen D, De Bruin-Weller M, Oosting B, Lebre C, De Jong E, et al. (2004) Serum thymus and activation- regulated chemokine (TARC) and cutaneous T cell- attracting chemokine (CTACK) levels in allergic diseases: TARC and CTACK are disease-specific markers for atopic dermatitis. J Allergy Clin Immunol 113(2): 334-340.
-
Niki T, Tsutsui S, Hirose S, Aradono S, Sugimoto Y, et al. (2009) Galectin-9 is a high affinity IgE-binding lectin with anti-allergic effect by blocking IgE-antigen complex formation. J Biol Chem 284(47): 32344- 32352.
-
Song TW, Sohn MH, Kim ES, Kim KW, Kim KE (2011) Increased serum thymus and activation-regulated chemokine and cutaneous T cell-attracting chemokine levels in children with atopic dermatitis. Clin Exp Allergy 36(3): 346-351.
-
Machura E, Rusek-Zychma M, Jachimowicz M, Wrzask M, Mazur B, et al. (2011) Serum TARC and CTACK concentrations in children with atopic dermatitis, allergic asthma, and urticaria. Pediatr Allergy Immunol 23(3): 278-284.
-
Fujisawa T, Fujisawa R, Kato Y, Nakayama T, Morita A, et al. (2002) Presence of high contents of thymus and activation-regulated chemokine in platelets and elevated plasma levels of thymus and activation- regulated chemokine and macrophage-derived chemokine in patients with atopic dermatitis. J Allergy Clin Immunol 110(1): 139-146.
-
Jahnz-Rozyk K, Targowski T, Paluchowska E, Owczarek W, Kucharczyk A (2005) Serum thymus and activation-regulated chemokine, macrophage- derived chemokine and eotaxin as markers of severity of atopic dermatitis. Allergy 60(5): 685-688.
-
Buckley RH, Fiscus SA (1975) Serum IgD and IgE concentrations in immunodeficiency diseases. J Clin Invest 55(1): 157-165.
-
Luster MI, Leslie GA, Bardana EJ (1976) Structure and biological functions of human IgD. VII. IgD antinuclear antibodies in sera of patients with autoimmune disorders. Int Arch Allergy Appl Immunol 52(1-4): 212-218.
-
Lertora JJ, Gomez-Perez FJ, Leslie GA (1975) Structure and biological functions of human IgD. V. Insulin antibodies of the IgD class in sera from some diabetic patients. Int Arch Allergy Appl Immunol 49(5): 597- 606.
-
Gleich GJ, Bieger RC, Stankievic R (1969) Antigen combining activity associated with immunoglobulin D. Science 165(3893): 606.
-
Tamma SM, Coico RF (1992) IgD-receptor-positive human T lymphocytes. II. Identification and partial characterization of human IgD-binding factor. J Immunol 148(7): 2050-2057.
-
Servet-Delprat C, Bridon JM, Blanchard D, Banchereau J, Brière F (1995) CD40-activated human naive surface IgD+ B cells produce IgG2 in response to activated T-cell supernatant. Immunology 85(3): 435- 441.
-
Kalach N, Kapel N, Waligora-Dupriet AJ, Castelain MC, Cousin MO, et al. (2013) Intestinal permeability and fecal eosinophil-derived neurotoxin are the best diagnosis tools for digestive non-IgE-mediated cow's milk allergy in toddlers. Clin Chem Lab Med 51(2): 351-361.
-
Norvell A, Monroe JG (1996) Acquisition of surface IgD fails to protect from tolerance-induction. Both surface IgM- and surface IgD-mediated signals induce apoptosis of immature murine B lymphocytes. J Immunol 156(4): 1328-1332.
- Understanding Pediatric Multiple Sclerosis: Clinical Presentation, Diagnostic Criteria, Therapeutic Advances, and Supportive Care Approaches
- Hemophilia in Children
- Xia-Gibbs Syndrome- A Case Report
- A Study to Assess Effectiveness of Play Therapy in Reducing Post-Operative Pain among Children Age 2 To 5 Year who have Undergone General Surgeries in Selected Pediatric Hospitals of Vadodara
- Preterm Birth: Scope of the Problem, Cost of Care, Potential Complications and Current Guidelines for Management
- Noradrenaline: Can we Use it to Manage Hemodynamic Instability among Neonatal Septic Shock at the NICU?