Neurocysticercosis in A Hematopoietic Stem Cell Transplanted Patient
We present the case of a 17 year-old-boy who underwent a haploidentical hematopoietic stem cell transplantation (HSCT) for high risk acute lymphoblastic leukemia. Six moths latter the patient presented in the Emergency Room with a generalized tonic-clonic seizure. He was diagnose of neurocysticercosis was made. The differential diagnosis of seizures is complex in these patients since they already have multiple problems and are under treatment with various drugs. Several causes may be implicated such us: viral or bacterial infections, bleeding, electrolyte disorders and drugs toxicities, to name a few. But we should also keep in mind, especially in these complicated patients, less common causes of seizures, as the one seen in this case. Neurocysticercosis is a disorder caused by the Taenia solium larva. It is the most common parasitosis of the central nervous system. The treatment of symptomatic neurocysticercosis includes antihelminthic therapy, corticosteroids and antiepileptic drugs. The knowledge of these pathology is vital to guide the proper treatment. We believe that it would be interesting to be published in your journal. Thank you in advance, The author.
Letter to Editor
Neurocysticercosis (NCC) is considered a serious public health problem in countries such as Latin America, Letter to Editor China, South- East Asia, Indonesia, Haiti and Sub-Saharan Africa. It is becoming more commonly diagnosed in developed countries due to increasing immigration from, and more frequent travel to, countries where the disease is endemic_._ It is one of the leading etiologies of acquired epilepsy worldwide.
Neurocysticercosis (NCC) is a disorder caused by infestation of the central nervous system with Taenia solium larvae [1]. Humans are the only definitive hosts for the adult tapeworm, whereas both pigs and humans may act as intermediate hosts for the larval form called cysticercus. Humans acquire infection by ingestion of its eggs from contaminated food or by direct hand-to-mouth transfer. Once exposed to gastric acid, the eggs hatch into larvae (oncospheres) penetrate the intestinal wall, and disseminate throughout the body, including central nervous system, skeletal muscle, subcutaneous tissue, and eyes [1, 2]. Here they mature into cysticerci. Within the brain, the cysts tend to locate in the richly irrigated gray matter in the parietal lobes. It is the most common parasitosis of the central nervous system (CNS). Infectious diseases are important complications of immunosuppressed patients, but NCC in transplant recipients is uncommon [3, 4].
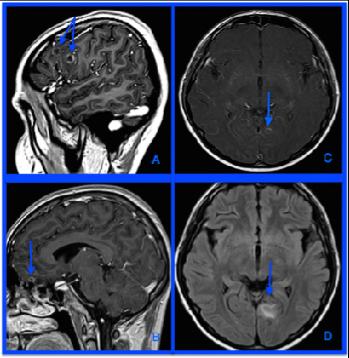
HSCT from peripheral blood source, with CD3+/CD19+ depletion without relevant complication. The donor was his 13 year-old- sister. In April 2009 the patient presented in the Emergency Room with a generalized tonic-clonic seizure that lasted for five minutes. He was previously asymptomatic and refer no headache, fever, or previous trauma. Neurological examination was unremarkable. Biochemical and microbiologic serum studies were normal, including plasma serology for cysticercosis. Neuroimaging findings, computed tomography scan (CT) and magnetic resonance imaging (MRI) were compatible with NCC. Four cystic intraparenchymatous lesions where seen: two in the right frontal lobe, a small one in left frontal gyrus rectus and one in occipital lobe. They show rim-enhancement after contrast administration and surrounding edema on FLAIR T2-weighted images (Figure 1). Anticonvulsant treatment was started with phenytoin and levetiracetam. Lumbar puncture revealed normal CSF analysis (red blood cells 2/mm3, white blood cells 2mm3, protein 33 mg/dL, and glucose 52 mg/dL). PCR for Taenia Solium was positive in cerebrospinal fluid, with no evidence of leukemic, or infection. The patient began treatment with praziquantel and systemic steroids. Treatment lasted for 2 weeks and it was completed without complications or neurological symptoms. Eight years follow-up the patient remains asymptomatic and in complete remission.
We present a case of a a17-year-old Hispanic boy, who emigrated to Spain ten years earlier. He was born in Perú, and his family moved to Spain, when he was little. They used to travel once a year to Peru to visit his family. He was diagnosed with pre-B cell ALL in June 2008. He had a normal karyotype at diagnosis without CNS infiltration, adenopathies, medistinic mass, splenomegaly or testicular involvement. He showed poor response to initial treatment, reaching first complete remission in September 2008 after FLA-GIDA chemotherapy. He was referred for matched sibling HSCT in a molecular complete remission. Our patient received haploidentical
Increasing numbers of NCC are observed in the developed world, in areas with large migrant populations [1]. It is a condition that must always be considered in the differential diagnosis in transplant patients with CNS involvement and cystic lesions in neuroimaging [2, 3, 4]. The natural history of neurocysticercosis in the setting of transplant recipients is not well understood. Few available reports have been published in the context of solid organ transplantation and one in HSCT in an adult woman [1, 3, 6, 7]. The clinical manifestations of NCC are presented mainly by the parasite’s mass effect and the host- immune response built up against the parasite. Children present more often with seizures (84-87%), that are generally brief, lasting less than 5 minutes. Other symptoms, such as headache, hemiparesis, and ataxia, may be present and are determined by the cyst location within the neuraxis [8]. Diagnosis of NCC is a challenge that incorporates clinical, radiologic, immunologic, and epidemiologic criteria. A set of diagnostic criteria based on the objective evaluation of this data have been proposed to diagnose patients with suspected neurocysticercosis [9](Table 1).
| Diagnostic criteria and degrees of diagnostic certainty for neurocysticercosis | ||
| Diagnostic Criteria | ||
| Absolute | ||
| ● Histologic demonstration of the parasite from biopsy of a brain or spinal cord lesion | ||
| ● Evidence of cystic lesions showing the scolex on neuroimaging studies | ||
| ● Direct visualization of subretinal parasites by fundoscopic examination | ||
| Major | ||
| ● Evidence of lesions highly suggestive of neurocysticercosis on neuroimaging studies | ||
| ● Positive serum immunoblot for the detection of anticysticercal antibodies | ||
| ● Resolution of intracranial cystic lesions after therapy with albendazole or praziquantel | ||
| ● Spontaneous resolution of small single enhancing lesions | ||
| Minor | ||
| ● Evidence of lesions suggestive of neurocysticercosis on neuroimaging studies | ||
| ● Presence of clinical manifestations suggestive of neurocysticercosis | ||
| ● Positive CSF ELISA for detection of anticysticercal antibodies or cysticercal antigens | ||
| ● Evidence of cysticercosis outside the central nervous system Epidemiologic: | ||
| Epidemiologic | ||
| ● Individuals coming from or living in an area where cysticercosis is endemic | ||
| ● History of frequent travel to disease-endemic areas | ||
| ● Evidence of household a contact with T. solium infection | ||
| Degrees of Diagnostic Certainty | ||
| Definitive | ||
| ● Presence of one absolute criterion | ||
| ● Presence of two major plus one minor or one epidemiologic criteria | ||
| Probable | ||
| ● Presence of one major plus two minor criteria | ||
| ● Presence of one major plus two minor or one epidemiologic criteria | ||
| ● Presence of three minor plus one epidemiologic criteria |
Table 1: Diagnostic criteria for neurocysticercosis.
The NCC treatment depends on the number, location, viability of parasites in CNS and host inmnune situation. Currently anticysticercal therapy has been marked by intense controversy. Recent data from endemic regions have led to the emergence of a growing body of literature to guide anthelmintic therapy in NCC, even in the setting of HSCT [3]. Many studies have documented that antiparasitic therapy results in death and resolution of viable cysts, but the clinical benefit of this treatment has been questioned. Other recent descriptions of spontaneous resolution of parenchymal cysticercosis with benign evolution, risks of complications and reports of no long-term benefits have reinforced the debate over the usefulness and safety of anticysticercal therapy [3, 9]. The
treatment modalities available to patients with NCC include surgery, symptomatic therapy and antiparasitic drugs. All patients with seizures require symptomatic therapy with antiepileptic drugs. For viable parenchymal cysts, anticysticercal drugs such as albendazole or praziquantel, in combination with corticosteroids to suppress post-treatment edema is indicated [2, 3, 4]. When cyst are accesible minimally invasive surgery is an option. Treatment of patients with asymptomatic central nervous system lesions is primarily conservative. Conservative management without anthelmintics, steroids, or anti-epileptics can be a valid strategy in selected cases (asymptomatic, pre- existing, stable, solitary lesions affecting noncritical areas of the brain) [3].
In the setting of an immunocompromised state in the contexto of HSCT, the benefits of treating the disease, appear to be significant, but must be carefully balanced against the risk of toxicity from anthelmintics, anti- epileptics, and corticosteroids, along with the possible mitigation of a graft-versus-malignancy effect [3, 9, 10].
References
-
Barra V, Moreno A, Fundora Y, Meneu JC , Jiménez de los Galanes SF, et al. (2007) Second case of neurocysticercosis in a patient with liver transplantation (first case in Spain): A Case Report. Transplant Proc 39(7): 2454-2457.
-
Del Brutto OH (2014) Clinical management of neurocysticercosis. Expert Rev Neurother 14(4): 389- 396.
-
Purve S, Lu K, Mukkamalla SK, Anandi P, Dumitriu B, et al. (2015) Kranick Conservative management of neurocysticercosis in a patient with hematopoietic stem cell transplantation: a case report and review. Transpl Infect Dis 17(3): 456-462.
-
Pratibha Singhi, Sunit Singhi (2004) Topic Review: Neurocysticercosis in Children. J Child Neurol 19(7): 482-492.
-
García HH, Del Brutto OH (2003) Imaging findings in neurocysticercosis. Acta Trop 87(1): 71-78.
-
Gordillo-Paniagua G, Munoz-Arizpe R, Ponsa-Molina R (1987) Unusual complication in a patient with renal transplantation: cerebral cysticercosis. Nephron 45(1): 65-67.
-
Hoare M, Gelson WT, Antoun N, Alexander GJ (2006) Early recurrence of neurocysticercosis after orthotopic liver transplant. Liver Transplant 12(3): 490-491.
-
Walker M, Zunt Jr (2005) Parasitic central nervous system infections in immunocompromised hosts. Clin Infect Dis 40(7): 1005-1015.
-
Del Brutto OH (2014) Neurocysticercosis. Hand book Clinical Neurology 121: 1445-1459.
-
Takayanagui OM, Odashima NS, Bonato PS, Lima JE, Lanchote VL (2011) Medical management of neurocysticercosis. Expert Opin Pharmacother 12(18): 2845-2856.
- Understanding Pediatric Multiple Sclerosis: Clinical Presentation, Diagnostic Criteria, Therapeutic Advances, and Supportive Care Approaches
- Hemophilia in Children
- Xia-Gibbs Syndrome- A Case Report
- A Study to Assess Effectiveness of Play Therapy in Reducing Post-Operative Pain among Children Age 2 To 5 Year who have Undergone General Surgeries in Selected Pediatric Hospitals of Vadodara
- Preterm Birth: Scope of the Problem, Cost of Care, Potential Complications and Current Guidelines for Management
- Noradrenaline: Can we Use it to Manage Hemodynamic Instability among Neonatal Septic Shock at the NICU?