Blood-Transfusion-Associated Necrotizing Enterocolitis (TANEC)
We are reporting here 3 cases of preterm babies who had severe fatal necrotizing enterocolitis in our NICU within 48 hours of packed RBCs transfusion. All the cases happened over one-month period. They were all relatively stable before blood transfusion. The transfusion was given for anemia of prematurity as hemoglobin and hematocrit were low. Within 48 hours of the transfusion, they started to have abdominal distension and hypoactivity and rapidly progressed to severe necrotizing enterocolitis and despite all supportive measures and pediatric surgeon involvement they died within one day. We report these cases to alert neonatologists about blood transfusion associated Necrotizing enterocolitis (TANEC) which is usually severe and can be fatal as in our cases.
Introduction
Necrotizing enterocolitis is the most common gastrointestinal disease in neonates and specifically in preterm babies. The incidence of disease increases with decreasing gestational age. The incidence is about 6-7 percent in very low birth weight (VLBW) and increases to 11.5 percent in babies less than 750g [1, 2, 3]. The cause of this life-threatening condition is multifactorial with no definite reason. The condition causes damage to the intestinal tract ranging from mucosal injury to full thickness necrosis and perforation. TANEC is a severe neonatal gastrointestinal reaction temporally related to a transfusion of packed blood red cells (PRBCs) for anemia in very low birth weights. This condition (TANEC) was recently recognized and there is many reports and studies support the relation between transfusion and gut injury in the form of necrotizing enterocolitis [4, 5]. Different mechanisms have been suggested to explain this relationship and they will be discussed here.
Case 1
Preterm 26 weeks gestational age, third quadruplet, birth weight 810g born by emergency Lower segment Cesarean section (LSCS) with apgar score 6 and 8 at 1 and 5 minutes respectively. Initially he required full ventilation and one dose of Surfactant (survanta) because of clinical and radiological respiratory distress in addition to increasing oxygen requirements. He was extubated to nasal Continuous positive airway pressure (CPAP) on day 3 of life and tolerated well. He was started enteral feeding on day 2 and gradually increased to full feeding over 2 weeks. He tolerated the enteral feeding well without any abdominal signs. His brain ultrasound showed intraventricular hemorrhage grade II which was resolving on serial ultrasounds. On day 19 of life, he was still on nasal CPAP and on full orogastric feeding, his hemoglobin was low in the blood gases, and full blood count showed hemoglobin of 9.2gm/dl and hematocrit of 26. He received packed red blood cell transfusion.
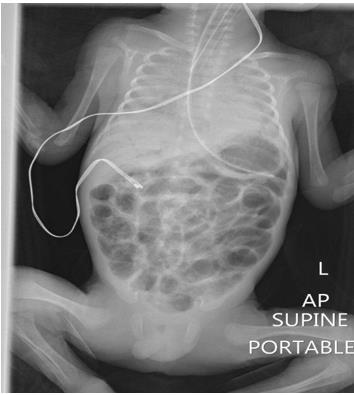
After 18 hours of blood transfusion, he started to have abdominal distension and became less active with increasing respiratory distress. Blood gases showed mixed metabolic and respiratory acidosis, pH 6.8, pco2 91, Hco3 16, BE -15. He was intubated immediately and sepsis screen was collected and started on triple antibiotics (vancomycin, meropenem and flagyl). Abdominal x-ray showed picture suggestive of necrotizing enterocolitis (Figure 1). Over the next few hours, he deteriorated very fast with bleeding from nasogastric tube, metabolic acidosis and hypotension which was resistant to treatment. Despite all supportive and aggressive measures, he died within few hours.
Case 2
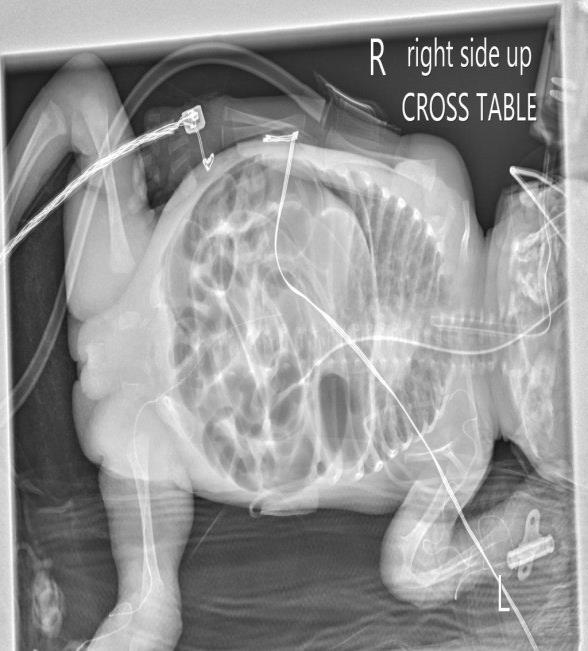
Preterm 25 weeks gestational age, birth weight 600g, had respiratory distress syndrome and received one dose of Surfactant (Survanta). Feeding started and increased gradually to full feeding at 18 days old. Extubation to noninvasive ventilation failed several times. She remained on ventilator with minimal parameters till day 38 when her hemoglobin dropped to 8.3 gm/dl and hematocrit was 25. Packed RBCs was transfused and after 26 hours, she became hypoactive with abdominal distension. Abdominal x-ray showed Necrotizing enterocolitis with pneumatosis intestinalis (Figures 2 & 3). Sepsis screen was sent and antibiotics was started, blood culture was negative, CRP 35, platelets was normal. She deteriorated very fast and died within 10 hours.

Case 3
Preterm 25 weeks gestational age, birth weight 630g. He had respiratory distress syndrome and received one dose of Surfactant (Survanta). Feeding started and increased gradually to full feeding at 2 weeks of age. Extubation to noninvasive ventilation failed and he remained on ventilator with minimal parameters till age 27 when his hemoglobin was 9.6gm/dl and hematocrit was 29. Packed RBCs was transfused and after 36 hours, he started to have abdominal distension and abdomen x- ray showed necrotizing enterocolitis with pneumatosis intestinalis (Figure 4). He deteriorated rapidly and developed severe hypotension and despite all resuscitative measure, he died within 15 hours.

Discussion
Necrotizing enterocolitis is one of the most devastating diseases can happen in Neonatal Intensive Care Unit (NICU). It is an emergency medical and surgical problem, which needs rapid diagnosis and intervention. It has high morbidity and mortality. The incidence is 1 to 3 per 1000 live births and 1 to 7.7 % of admissions to NICU [6]. The incidence increases with decreasing gestational age with incidence of 6 to 7 percent in very low birth weight infants (BW less than 1500gm) [1, 2, 3]. Although the association between Necrotizing Enterocolitis (NEC) and blood transfusion was described as early as 1987 [7]. In recent years, researchers have conducted retrospective observational studies to examine the occurrence of NEC within 48 hours of transfusion. The incidence of Transfusion-associated Necrotizing Enterocolitis (TANEC) varies from 20–35% of NEC cases and reports suggest that infants with TANEC are more likely to develop more surgical NEC [4, 5].
Since 2010, several papers have been published showing the relation between blood transfusion and necrotizing enterocolitis. Although there is no randomized controlled study showing this relation, there are many case reports and observational studies, which suggest this association.
A meta-analysis of observational data was published in 2012 concluded that Recent exposure to transfusion was associated with NEC in neonates and TANEC patients were at higher risk of mortality [5].
Another study in 2014 concluded that blood transfusion is a strong risk factor for NEC [8].
On the other hand, two recent reports did not find PRBC transfusion as a risk factor for NEC [9, 10]. The pathophysiology for transfusion associated NEC is unknown. The most accepted theory is a ‘‘two hits’’ model in which host neutrophils are ‘‘primed’’ by an antecedent illness followed by the passive transfusion of biological response mediators [11, 12]. Biological response mediators are either donor antibodies (eg, HLA or neutrophil antigen) or another class of activators such as bioactive lipids, free hemoglobin, red blood cell membrane fragments, cytokines, and so forth, accumulated in stored blood products. Another theory is that there is a perfusion alteration during the transfusion although Marin concluded that gut oxygenation did not change related to feeding during a transfusion based on a study of 8 infants using NIRS [13].
Can anemia itself cause NEC? Animal studies showed that anemia can impair gut blood flow and increase oxygen extraction as a compensatory mechanism [14, 15]. Our cases were hemodynamically stable before the blood transfusion and the current data did not show evidence relating NEC to anemia.
The relation between TANEC and feeding during the transfusion is unclear. Feeding may affect oxygen balance near the critical O2 point by contributing to reduced oxygen availability arising from red blood cell deficits in 2,3 DPG, abnormal red blood cell rheology, and changes in nitric oxide availability [16]. All our cases were on feeding during transfusion. In two reports the effect of withholding feeding during transfusion are described [17, 18]. Both studies report a drastic reduction in the unit’s NEC rate after the practice change and a near- eradication of TANEC. Unfortunately, some may consider the quality of these studies to be inferior but it is difficult to argue with the impact of the practice change on NEC rates. Holding feeding during transfusion may reduce the incidence TANEC rates but more prospective randomized controlled trials are needed to validate this practice.
The clinical presentations of our cases were severe and associated with rapid deterioration and all of them died within 24 hours of presentation. This presentation was uncommon in our unit in usual cases of NEC. This finding was found in other studies who reported higher morbidity and mortality [19].
Conclusion
We are reporting three cases of transfusion related NEC in moderately anemic preterm babies, a condition which has been described in many reports. All the cases were clinically stable before the transfusion and were on full feeding during the transfusion. Some reports showed decreased incidence of TANEC after withholding the feeding during transfusion. Randomized controlled studies are needed to confirm this evidence. The clinical presentation of the three cases were severe with rapid deterioration and all of them died within 24 hours. This should alert the neonatologists about the severity of this condition.
References
-
Horbar JD, Badger GJ, Carpenter JH, Fanaroff AA, Kilpatrick S, et al. (2002) Trends in mortality and morbidity for very low birth weight infants, 1991- 1999. Pediatrics 110: 143.
-
Sankaran K, Puckett B, Lee DS, Seshia M, Boulton J, et al. (2004) Variations in incidence of necrotizing enterocolitis in Canadian neonatal intensive care units. J Pediatr Gastroenterol Nutr 39(4): 366-372.
-
Lee SK, McMillan DD, Ohlsson A, Pendray M, Synnes A, et al. (2000) Variations in practice and outcomes in the Canadian NICU network: 1996-1997. Pediatrics 106(5): 1070-1079.
-
Christensen RD, Lambert DK, Henry E, Wiedmeier SE, Snow GL, et al. (2010) Is "transfusion-associated necrotizing enterocolitis" an authentic pathogenic entity? Transfusion (Paris). 50(5): 1106-1112.
-
Mohamed A, Shah PS (2012) Transfusion associated necrotizing enterocolitis: a meta-analysis of observational data. Pediatrics 129(3): 529-540.
-
Kosloske AM (1994) Epidemiology of necrotizing enterocolitis. Acta Paediatr Suppl 396: 2-7.
-
McGrady GA, Rettig PJ, Istre GR, Jason JM, Holman RC, et al. (1987) An outbreak of necrotizing enterocolitis. Association with transfusions of packed red blood cells. Am J Epidemiol 126(6): 1165-1172.
-
Gephart SM, Spitzer AR, Effken JA, Dodd E, Halpern M, et al. (2014) Discrimination of Gut Check (NEC): a clinical risk index for necrotizing enterocolitis. J Perinatol 34(6): 468-475.
-
Kirpalani H, Zupancic JA (2012) Do transfusions cause necrotizing enterocolitis? The complementary role of randomized trials and observational studies. Semin Perinatol 36(4): 269-276.
-
Sharma R, Kraemer DF, Torrazza RM, Mai V, Neu J, et al. (2014) Packed red blood cell transfusion is not associated with increased risk of necrotizing enterocolitis in premature infants. J Perinatol 34(11): 858-862.
-
Lee J, Gladwin M (2010) Bad blood: the risks of red cell storage. Nat Med 16(4): 381-382.
-
Frenette P, Mohandas N (2010) Bad blood: A trigger for TRALI. Nat Med 16: 382-383.
-
Marin T, Moore J, Kosmetatos N, Roback JD, Weiss P, et al. (2013) Red Blood Cell Transfusion-Related Necrotizing Enterocolitis in Very Low Birth Weight Infants: A Near-Infrared Spectroscopy Investigation. Transfusion 53(11): 2650-2658.
-
Krimmel G, Baker R, Yanowitz T (2009) Blood transfusion alters the superior mesenteric artery blood flow velocity response to feeding in premature infants. Am J Perinatol 26(2): 99-105.
-
Szabo J, Mayfield S, Oh W, Stonestreet B (1987) Postprandial gastrointestinal blood flow and oxygen consumption: effects of hypoxemia in neonatal piglets. Pediatr Res 21(1): 93-98.
-
Bennett-Guerrero E, Veldman T, Doctor A, Telen M, Ortel T, et al. (2007) Evolution of adverse changes in stored RBCs. Proc Natl Acad Sci USA 104(43): 17063- 17068.
-
El-Dib M, Narang S, Lee E, Massaro AN, Aly H (2011) Red blood cell transfusion, feeding and necrotizing enterocolitis in preterm infants. J Perinatol 31(3): 183-187.
-
Stritzke AI, Smyth J, Synnes A, Lee SK, Shah PS (2013) Transfusion-associated necrotising enterocolitis in neonates. Arch Dis Child Fetal Neonatal Ed 98(1): 10- 14.
-
Perciaccante JV, Young TE (2008) Necrotizing Enterocolitis associated with packed red blood cell transfusions in premature neonates. E-PAS. 5839.8.
- Understanding Pediatric Multiple Sclerosis: Clinical Presentation, Diagnostic Criteria, Therapeutic Advances, and Supportive Care Approaches
- Hemophilia in Children
- Xia-Gibbs Syndrome- A Case Report
- A Study to Assess Effectiveness of Play Therapy in Reducing Post-Operative Pain among Children Age 2 To 5 Year who have Undergone General Surgeries in Selected Pediatric Hospitals of Vadodara
- Preterm Birth: Scope of the Problem, Cost of Care, Potential Complications and Current Guidelines for Management
- Noradrenaline: Can we Use it to Manage Hemodynamic Instability among Neonatal Septic Shock at the NICU?